
Abstract
Background:
Fecal occult blood tests are recommended for colorectal cancer screening, but are only effective if colonoscopy follows positive results. Patients with positive results often do not complete follow-up. This study examined the association between patient comprehension and adherence to colonoscopy after positive FIT (Fecal Immunochemical Test).
Methods:
Five hundred twenty-two patients completed a telephone questionnaire regarding the FIT and its implications 120 days after a positive result. Patients were asked whether they had the test, received the results, and required follow-up. These questions were used to identify the degree to which patients understood medical information. A participant who answered “no” to any question was defined as having “low comprehension” regarding the FIT, and participants who answered “yes” to all 3 questions, as having “high comprehension”.
Results:
Comprehension and colonoscopy adherence were significantly associated. Adherence to colonoscopy was significantly higher among participants with high comprehension, after adjusting for gender, age, education, ethnicity, and socio-economic status.
Conclusions:
This study demonstrates a link between health comprehension and patient follow-up after positive FIT and contributes to understanding the implications of health comprehension in terms of health promotion. We recommend patients undergoing screening tests receive clear explanations regarding need for follow-up of positive results thus reducing health disparities associated with health comprehension.
Keywords
Introduction
Colorectal cancer (CRC) is a major cause of morbidity and mortality throughout the world, and it is the second leading cause of cancer incidence and mortality in developed countries. Screening for CRC is recommended for people aged 50 to 75 either with direct visualization via colonoscopy every 5 to 10 years, or using a two-stage process: an annual or biannual fecal occult blood test (FOBT) followed by a colonoscopy for those with positive results. To maximize the benefits of screening, a positive FOBT result requires prompt follow-up with colonoscopy. Delaying colonoscopy significantly undermines the benefits of CRC screening, which include decreased morbidity and mortality, life-years saved, and lower net costs of screening. In spite of this, a large proportion of individuals with a positive FOBT do not continue with follow-up. 1 –4
Barriers to follow-up after a positive FOBT have been identified. 5 –10 Patient barriers to obtaining follow-up colonoscopy after a positive FOBT include stress and anxiety that can affect responsiveness to further investigation. 11,12 Some patients have refused to perform an invasive colonoscopy examination despite a positive blood result and only agreed to follow-up via a noninvasive virtual colonoscopy. 13 It was also found that if people in the immediate social environment (family, friends, and co-workers) undergo the test, the person is more likely to, as well. 14
Health literacy is increasingly recognized as a critical factor affecting communication across the continuum of treatment. It is the degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions. The definition of health literacy was extended to more comprehensive aspects including the knowledge, motivation, and competencies to access, understand, appraise, and apply information in order to make decisions in everyday life concerning health care, disease prevention, and health promotion. 15 According to the National Adult Literacy Survey, “about one in five American adults may lack the necessary literacy skills to function adequately in our society”. 16 As patients, such individuals are at a disadvantage in their ability to process and understand cancer-related information and to obtain the services needed to make appropriate health-care decisions. Patients with poor health literacy have a complex array of difficulties that may limit their understanding of cancer screening and health status. In addition, these barriers impair communication and discussion about the risks and benefits of treatment options. Low health literacy appears to affect compliance with cancer screening and is associated with less knowledge of cancer prevention and greater misunderstanding regarding susceptibility to cancer, the benefits of early detection, and its prognosis. 16,17 Low literacy may also influence the source and accuracy of the information received. 18 All of these factors may, in turn, influence participation in cancer screening. 19,20 Specifically, patients with low health literacy will adhere to CRC screening less than those with high literacy skills would. 17 –24
This study was conducted in Israel, a country with high immigration rates. Approximately 20% of the population was not born in Israel and 150 000 immigrants arrived from 2013 through 2017. 25 According to the OECD, 36% of adult Israelis have a relatively low level of literacy and numeracy, and these are strongly correlated with reported health status. 26 In a study of the association between health literacy, health behavior, socio-economic indicators and self-assessed health, researchers found that 31% of respondents to a survey in Israel had problematic health literacy. 27 Studies have demonstrated an association between immigration and lower CRC screening rates, but these evaluated the initial screening procedure, and not follow-up after a positive result. 28,29
In addition to immigration, 26% of the Israeli population speaks Arabic as a first language, with varying levels of literacy in Hebrew. Azaiza and Cohen 30 demonstrated CRC screening rates were higher among the Jewish population than among the Arab population, due to several factors, including differences in risk perception, benefit perception, physician recommendation and locus of control. Significant predictors of FOBT included higher education, older age, a first-degree relative with CRC, higher belief in benefits to be gained from the test, and receiving a recommendation to perform the test.
All Israeli citizens are insured under the National Health Insurance Law, which mandates community health and hospitalization coverage for the public sector. Israelis can purchase extended insurance coverage from their health-care provider and private health insurance. Meuhedet Healthcare Services is one of four health maintenance organizations in Israel. It insures and provides care for 1.2 million members. The current rate of CRC screening (annual FIT (fecal immunochemical test) or colonoscopy in the previous 10 years) among 180 000 members, ages 50 to 75 is 60%, similar to national rates. The rate of follow-up colonoscopy after a positive FIT in Meuhedet was 41%. In order to improve follow-up rates, we conducted a study 31 in 2016 assessing the usefulness of sending a short message service (SMS) regarding colonoscopy follow-up after a positive FIT. We found that 17% of patients who had completed an FOBT did not remember having the test and were not aware of the test results.
The aim of the current study was to examine the association between patient comprehension of medical information and adherence to colonoscopy follow-up among patients who had a positive FIT. To the best of our knowledge, this is the first time that a patient’s ability to comprehend test results and their implications were examined in relation to adherence to follow-up recommendations after positive screening FIT results.
Methods
The study was approved by the Meuhedet Institutional Review Board (trial reference number: 02-20-05-15). As this was a telephone survey, response to the survey served as informed consent.
Study Population
A total of 762 patients from Meuhedet who had a positive FIT between March 2016 and September 2016 participated in this study. Exclusion criteria were personal or family history of CRC, colonoscopy 2 years before the positive FIT, or diagnosis with any type of cancer during the study period. A total of 240 (31.5%) patients were excluded, 46 (6%) because of family history of CRC, 2 (0.2%) died during the study, 63 (8.2%) had an oncology diagnosis, 26 (3.4%) had a colonoscopy prior to the positive FIT, and 103 (13.5%) refused to participate in the survey.
The final study population consisted of 522 participants; all patients who met the inclusion criteria and agreed to complete the telephone survey during the study period.
Study participants were asked to complete a telephone survey 120 days (± 7 days) after the positive FIT (whether the patient performed colonoscopy or not). The survey included questions regarding health status, understanding the screening results, and interactions with health-care providers. The survey was conducted in Hebrew, Arabic, Russian or English, as needed.
Study Variables
The dependent variable for this study was completion of a colonoscopy up to 120 days following a positive FIT. A preliminary study found that the median follow-up in Israel was 112 days.
The variable of interest in this study is health comprehension. As previously presented, there is a strong association between health literacy and health behavior, and health literacy includes message comprehension. As a measure of health comprehension, each participant was asked three questions about their FIT result: (1) “Have you had any tests over the past year to check for occult blood in the stool?”; (2) “Did you receive the fecal occult blood test results?”; (3) “Was the fecal occult blood test result positive?”. A participant who answered “no” to any one of the three questions was classified as having a “low comprehension” level, and participants who answered “yes” to all 3 questions were classified as “high comprehension”.
When FIT results are positive an automated computer alerts the physician who is notified via the patient’s EMR. The alert to the physicians is automatically generated the moment the lab releases the positive result. All study participants were advised either by telephone or face-to-face of test results by their physician and this interaction was documented in the EMR. A validation process was conducted to ensure that all participants who stated that they had not been notified of the test results, had been notified, and did not remember and/or did not understand the results. We ascertained that there was documentation in the electronic medical record (EMR) that the physician had notified the patient of the results, as required.
Additional dependent variables that we included in our analyses were: socio-economic status (SES), insurance level and demographic variables (gender, geographic district, age, education level, marital status, country of birth, ethnicity, and religion). The SES is derived from the member’s home address and based on the Israeli Census Bureau locality definitions. The SES levels range from 1 to 20; 20 is the highest. For the purpose of this study, SES levels were grouped into three levels: 1 to 8 low, 9 to 13 medium, and 14 to 20 high, as this is an accepted method of categorizing the population. Insurance level was defined as basic, additional, and private insurance.
As stated above, this study stemmed from a previous study 31 that examined the effect of a text message on adherence to follow-up. Therefore, participants in the current study had been randomized into an intervention group, who received an SMS alert regarding their test results, and a control group, who did not.
Data sources
The FIT results were obtained from the Meuhedet Central Laboratory database. Colonoscopy follow-up and demographic and clinical characteristics were obtained from the patients’ EMR.
Data Analysis
Data were analyzed using IBM SPSS statistics software (version 24.0, for Windows). P < .05 was considered to be significant for all analyses.
The χ2 test was used to explore possible associations between socio-demographic variables and rate of adherence to colonoscopy and to assess the association between health comprehension and adherence. Logistic regression was used to calculate odds ratios (ORs) and 95% confidence intervals (CIs) for performing colonoscopy within 120 days, adjusting for potential confounders significantly related to adherence in univariate analysis.
Results
The final sample included 522 respondents, 88 (16.8%) in the “low comprehension” group and 434 (83.2%) in the “high comprehension” group. The groups were similar in age and gender. There were significantly more Jewish than non-Jewish people in the “high health literacy” group (P < .001), as well as a higher proportion of those with over 12 years of education (56.5% vs 38.6%, P < .001). There were significantly more patients who agreed to receive SMS from the provider in the high comprehension group (P < .001), as well as a higher proportion of those with additional insurance and private insurance (P < .001). There were twice as many participants in the lower SES level (35.2% vs 17.1%, P < .0001) among those with “low comprehension”. In our questionnaire responses most of the patients stated they had received an explanation regarding the test, but the proportion was significantly higher in the high comprehension group (89.2% vs 71.6%, P = .00). Participant characteristics are presented in Table 1.
Patient Characteristics.

Abbreviations: FOBT, fecal occult blood test; SES, socio-economic status; SD, standard deviation; SMS, short message service.
Of 522 respondents, there were 272 (52.1%) men with a mean age of 62.6 ± 6.5 years and 250 (47.9%) women with a mean age of 62.1 ± 6.7 years. Among them, 326 (62.5%) patients adhered to colonoscopy within 120 days of the positive FIT.
Adherence was not associated with gender, age, or religion. Adherence rates were significantly higher among patients who had over 12 years of education versus patients with up to 12 years of education (66.7% vs 57.6%; P = .033), and among patients with higher SES, levels 14 to 20 (67.6%) and levels 9 to 13 (64.5%) versus patients with SES levels 1 to 8 (51.6%), (P = .045). Adherence rates were also higher among patients in the intervention group (70.3%) versus the control group (56.2%; P = .001), among patients who have additional insurance from their health-care provider (66.7%) versus patients who do not have additional insurance (36.1%; P = .000), and among patients who have private insurance in addition to the Healthcare organisation (HCO) insurance (66.8%) versus patients who do not have private insurance (58.6%; P = .054). Participants who answered that they had a FIT were asked whether they received an explanation regarding the test. Adherence rates were significantly higher among patients who stated that they had received an explanation about the FIT versus those who did not (67.5% vs 51.2%; P = .004).
A total of 38 (7.3%) patients answered “no” to the first question “Have you had any tests over the past year to check for occult blood in the stool?”, 20 (4.14%) answered “no” to the second question “Did you receive the fecal occult blood test results?” and 30 (4.31%) patients answered “no” to the third question “Was the fecal occult blood test result positive?”. Overall 88 (16.9%) patients were considered as having “low comprehension”.
Table 2 illustrates the association between adherence to follow-up colonoscopy and the 3 questions on which the health comprehension measure was based. Adherence rates were significantly higher among patients who responded that they had a FIT over the past year (64.7%) versus patients who claimed not to have carried out the screening test (34.2%; P = .000), and among patients who reported they received the FIT result (65.8%) versus patients who did not (40%; P =.018). Adherence rates were also significantly higher among patients who stated they received an explanation about the purpose of the test versus those who did not receive an explanation (65.8% vs 40.0%), (P = .018). Adherence rates were significantly higher among patients that stated that the FIT result was positive versus those who thought it was negative (66.8% vs 46.7%; P = .000). The adherence rate was twice as high among those with high versus low comprehension levels – defined as those who answered “no” to any of the above questions (P < .0001).
Response to Health Comprehension Questions and Rate of Adherence to Colonoscopy 120 Days After Positive FIT.
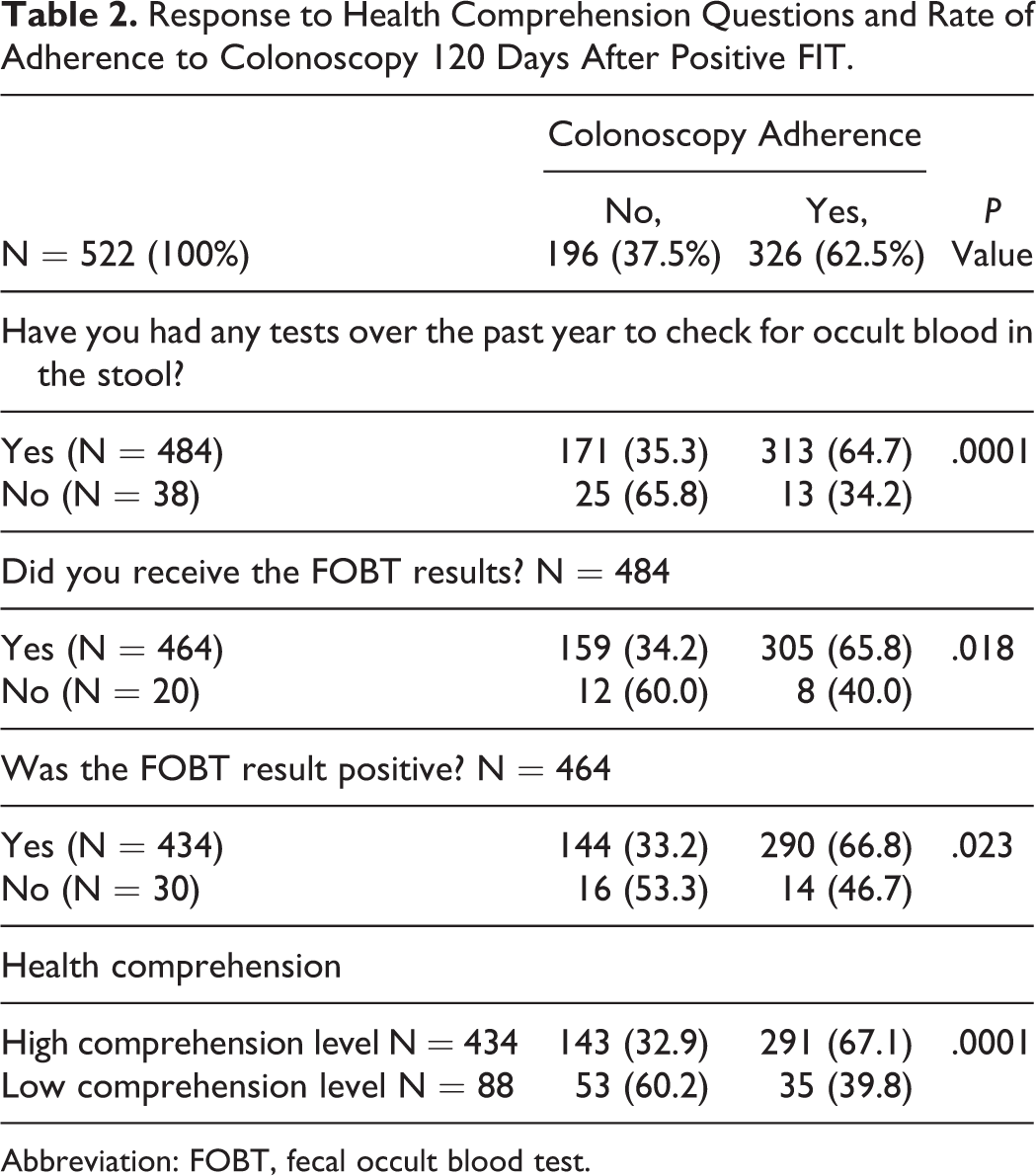
Abbreviation: FOBT, fecal occult blood test.
A low level of health comprehension was significantly less frequent among patients with over 12 years of education (12.2%) versus patients with up to 12 years of education (22.2%), (P = .002), and among patients with higher SES (27.5% in the 1-8 group, 14.1% in the 9-13 group, and 9.0% in the 14-20 group; P = .001).
Logistic regression was performed to determine whether the colonoscopy rate was different between the 2 health comprehension groups, when adjusted for other variables: The odds ratio for colonoscopy was significantly higher in the high health comprehension group as compared with the low health comprehension group, after adjusting for age, gender, education, intervention versus control group, agreed to receive SMS from the provider and receiving an explanation about the FOBT test (OR = 2.095, 95% CI: 1.129-3.890; P = .019; Table 3).
Odds Ratios for Colonoscopy up to 120 days for Study Variables.
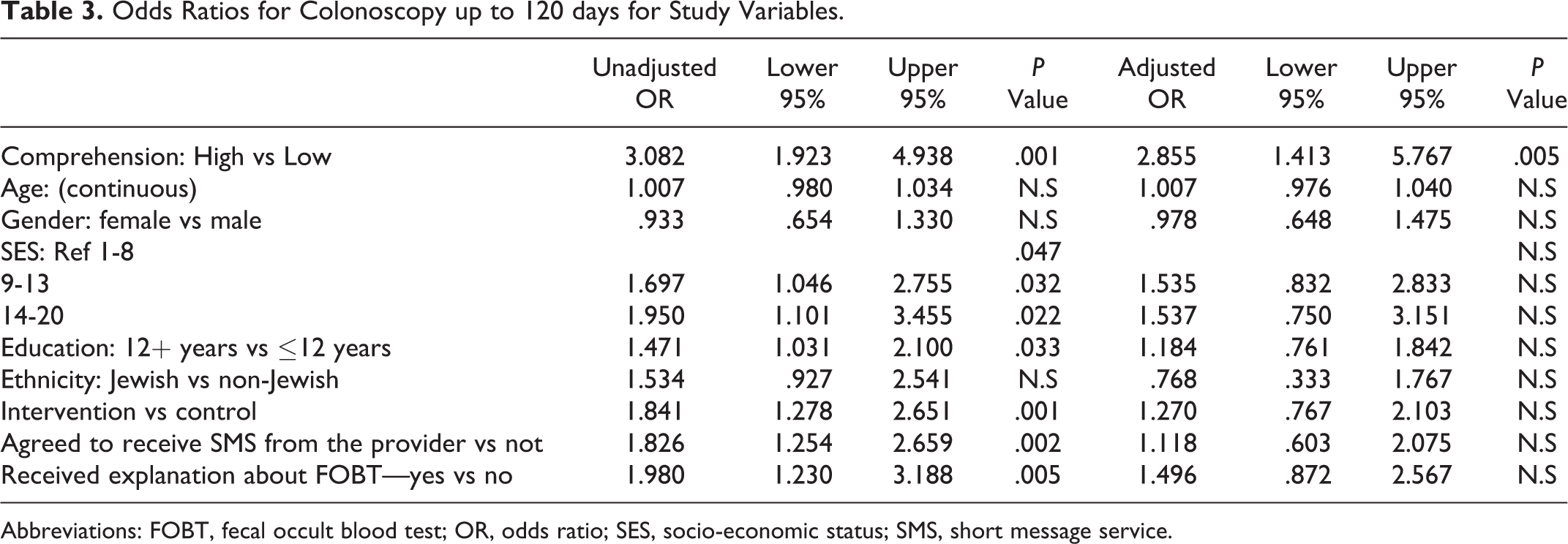
Abbreviations: FOBT, fecal occult blood test; OR, odds ratio; SES, socio-economic status; SMS, short message service.
No association was found between the profession of the caregiver who recommended the test or provided the kit and health comprehension or adherence.
Discussion
This study examined the association between patient understanding of medical information and completion of follow-up after a positive fecal occult blood screening test. We decided to investigate this issue following a survey that was part of a larger study investigating barriers to follow-up among these patients. The survey showed that 17% of people who had a positive FOBT result did not understand having the test, the test results, or its implications.
The findings of the current study demonstrate that after adjusting for education, and ethnicity and receiving an explanation about the test (all associated with both health literacy and follow-up), patients who comprehended the terminology of FOBT test results were twice as likely to complete follow-up.
In univariate analysis, the proportion of people defined as having high health comprehension according to the study questionnaire was greater among those who adhered to colonoscopy as opposed to those who did not (67.1% vs 32.9%, respectively; P < .001). Health literacy is a critical factor affecting communication across the continuum of treatment. 17,21 Limited health literacy appears to have a multifaceted effect on adherence to cancer screening recommendations. Low health literacy is associated with less knowledge of cancer prevention and greater misunderstanding about susceptibility to cancer, the benefits of early detection, and prognosis. 16,17 Low literacy can influence the source and accuracy of the information received, as people with low health literacy are less able to identify and access accurate and reliable sources of health information. 18 All these factors might influence participation in cancer screening in general and CRC screening in particular. Specifically, patients with limited health literacy adhere less than those with high health literacy skills do. Our findings support this association as comprehension of test results are closely related to health literacy. In addition, we found that even after a positive screening test, patients defined in our study as having low health comprehension have a lower rate of follow-up, which therefore places them at-risk.
Age, gender, education, receiving an explanation about the test, and ethnicity were associated with our health comprehension measure. A study conducted in Israel showed that years of education and income were significantly associated with health literacy. Health literacy, along with age, was the strongest independent variable associated with self-assessed health. 27 The current study also found a significant association between health comprehension, education and SES: 61.4% of those with less than 12 years of education had low health comprehension, compared with 38.6% of those with 12+ years (P = .002). Among patients with low SES, 35.2% had low health comprehension, compared with 14.1% in the high SES level (P = .01).
Non-Jewish ethnicity (primarily the Arab population and immigrants in Israel) can indicate a language barrier and therefore, may lead to limited understanding of the purpose of the FIT and the meaning of a positive or negative result. It may also be related to the level of cultural acceptance of the process required for follow-up. In this study, Arab ethnicity was associated with lower adherence to follow-up – 53.5% vs 63.9% (P = .095) and with lower health comprehension – 31.8% of Arab patients had low health comprehension, as compared with 9.9% of Jewish patients (P < .0001). These findings agree with those of a previous CRC screening study conducted in Israel, 30 where significant predictors of FOBT included higher education, older age, a first-degree relative with CRC, higher belief in benefits to be gained from the test, and receiving a recommendation to perform the test.
An interesting, albeit not surprising, finding in our study is that patients who remembered receiving an explanation about the test were more likely to adhere to follow-up, and more likely to have high health comprehension. This is important for 2 reasons. The first- people with lower comprehension still remember having an explanation. Second- those who remember having an explanation are more likely to adhere. Therefore, by incorporating a process of explaining and documenting the reason for the test and its consequences, it is possible to increase adherence and reduce disparities.
This study had several limitations. The first is that a validated measure of health literacy was not used. We used a surrogate measure of patients’ responses to three questions: Did you complete the test? Did you get the test result? Was the result positive? We assumed that if patients completed the test, and had been notified of the positive results, and answered “no” to any of these questions, it meant that they had trouble understanding medical information, or, in other words, had low health comprehension. It is possible that direct measurement of health literacy would have led to different findings, but this is unlikely. It is also possible that patients understood the significance of the test and its results, but did not remember them, as the calls were made 4 months later. It is almost impossible to differentiate between recall and comprehension as they are closely interrelated, but one can assume that if the information is understood and perceived as important, patients would remember it 4 months later. It is also possible that measuring patient comprehension regarding the test results is measuring physician communication skills, but this is unlikely, as no association was found between individual physicians and adherence. Another limitation of this study is that SES was not measured directly – it was obtained from the SES of the participants’ home address area based on postal codes. However, this methodology is common in research conducted as part of the Community Quality Indicator program in the Israeli Ministry of Health. 32 Another possible weakness is that we decided to limit time to colonoscopy to 120 days after the positive FIT result. It is possible that patients underwent colonoscopy 1 or 2 years after the initial FIT, but it would be difficult to relate this to the initial test. In addition, the Israeli Ministry of Health standards are 120 days, and previous studies have shown that very few patients have colonoscopies after this period has elapsed.
Conclusions
This is the first study to show an association between comprehension of test results and colonoscopy follow-up among CRC screening program participants with a positive FIT result. These findings are important and promising, as they suggest that improving patient understanding might lead to greater adherence regardless of other demographic and socio-economic measures. The work identified a gap in CRC screening and identified health comprehension as a determining factor. We recommend that when patients undergo screening tests, they receive a clear explanation of the need for follow-up if the test is positive, thus reducing health disparities associated with literacy.
An important finding of this study is that health comprehension was a stronger predictor of follow-up than were all other demographic variables, including age, gender, education, SES and ethnicity. A possible implication is that patient education regarding the reason for screening tests and the implications of the result, is essential regardless of subjective or objective attitudes related to the demographic variables.
The study results contribute to understanding the role of health comprehension in health disparities and identifying action areas for health promotion.
Footnotes
Authors’ Note
The study was approved by the Meuhedet Institutional Review Board (trial reference number: 02-20-5-15).
Acknowledgments
This study was performed by Revital Azulay as part of the requirements for a PhD degree at Bar Ilan University, Public Health and Health Systems Management Program, Department of Management, under the direction of Racheli Magnezi, Prof, MHA. The study was approved on May 20, 2015.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.