
Abstract
Background
Precancerous cervical lesion is an abnormality in the cells of the cervix that could eventually develop into cervical cancer. Cervical cancer is a public health problem that contributes to the death of women worldwide. In line with the high burden of the issue, the Ethiopian government had attempted to expand cervical cancer screening centers and recommendation of services to age-eligible as well as high-risk groups of women. Therefore, the study aimed to assess the prevalence of precancerous lesions of cervix cancer among women aged 30-49 years and associated factors in West Wollega.
Method
Facility-based analytic cross-sectional study design was conducted in selected hospitals of West Wollega from January 1- February 20, 2022, among 339 women. A face-to-face interview was conducted and the presence or absence of precancerous cervical lesion was tested by visual inspection with acetic acid. Data were analyzed by SPSS version 25. Variable with P-value <.25 in the bi-variable analysis were entered into multivariable logistic regression. Results with a P-value ≤ .05 at 95% confidence level were considered for statistical significance.
Result
The prevalence of precancerous cervical lesions was 27.4% (95% CI: 22.7%32.1%). The mean standard deviation of participants was 35.22 +6.32 years. More than half (63.4%) and 67.6% of them were regarded as having good knowledge and a favorable attitude towards precancerous cervical lesions respectively. History of menstrual irregularity had two folds higher odds of being diagnosed with the precancerous cervical lesion when compared with counterparts at, [AOR = 2.29(95% CI:1.29-4.04]. Women with a history of STI had 3.5 times higher odds of developing precancerous cervical lesion compared to women with no history of STI [AOR)=3.46(95% CI:1.94-6.18)], history of bleeding after sexual intercourse was 2.88 times more likely to have precancerous cervical lesion compared to those without it at [AOR=2.88(95% CI:1.43-5.78)]. Parity greater than or equal to five had 2.4 times higher odds of developing precancerous cervical lesions compared to women with parity less than five at [AOR=2.41(95% CI: 1.23-4.75)]. History of steroid use had 3.5 times higher odds of developing precancerous cervical lesion compared with opponents at [AOR=3.5(95% CI: 1.32-9.34) and women with an Unfavorable attitude towards screening for Cervical cancer screening, prevention, and control methods had 2.2 times higher odds of developing precancerous cervical lesion compared their counterpart at [AOR=2.15(95% CI: 1.21-3.83)].
Conclusion
The precancerous cervical lesions continue to be a significant public health concern in Ethiopia. It will remain a significant cause of death of women unless effective screening methods like VIA and vaccination against HPV are scaled up. Furthermore, having a history of menstrual irregularities, STI, bleeding after coitus, parity greater than ≥5, steroid use, and having an unfavorable attitude towards screening factors are significantly associated with the occurrence of the precancerous lesion. Therefore, effective prevention approaches have to consider these factors for the control of cervical cancer in the early phase of the lesion.
Introduction
A precancerous cervical lesion, which is also called an intraepithelial lesion, is an abnormality in the cells of the cervix that could eventually develop into cervical cancer. 1 Cervical cancer is a crucial point of action for any cancer control program because of the burden of the disease, and the possibilities for effective prevention via screening. 2 It is historically classified as adenocarcinoma and squamous cell carcinoma in 99% of women with squamous cervical carcinoma caused by Humans Papillomavirus (HPV) infection. 3
Cervical cancer is the leading cause of death in women. Worldwide, cervical cancer is the fourth leading cause of death in women. 4 By 2020, an estimated 604000 women have been diagnosed with cervical cancer worldwide and an estimated 342,000 women have died of the disease. 3 Globally, cervical cancer has an occurrence rate of 371,000 cases and a death rate of 190,000 with 80% of the cancer of the cervix death occurring in resource-limited countries. The maximum rates are found in Central and South America, East Africa, South, and South-East Asia, and the Western Pacific. The problem is mainly worse in sub-Saharan Africa. 1 In Africa, 80,400 women were diagnosed with cervical cancer each year and it is the second most common cancer in the region. Furthermore, 50,300 women die each year from the disease and it is the leading cause of death from cancer. In sub-Saharan Africa, cervical cancer accounts for 22.5% of all women with cancer, and the majority of women with cervical cancer live in rural areas.5,6 Ethiopia ranked 14th led by Malawi among the East African Countries. In Ethiopia, about 7095 new cervical cancer cases are diagnosed annually which makes it the 2nd leading cause of female cancer and the 2nd most common female cancer in women aged 15-44 years according to an estimate 2012.7,8
According to World Health Organization (WHO) estimates, cervical cancer is expected to kill more than 443,000 women by 2030, with a high rate (over 98% of deaths) believed to occur in developing countries (especially in Sub-Saharan Africa (SSA). 9 Non-communicable diseases such as cervical cancer cause devastating effects in developing countries. 5 Cervical cancer is the most common cancer in 23 countries and is the leading cause of death in 36 countries. Most of these countries are in sub-Saharan Africa, Melanesia, South America, and Southeast Asia. 10 Precancerous lesions can be progressed to cervical cancer and the risk for the development of cervical cancer if there is missed the chance of early identification of the precancerous lesion and its risk factor. 11 It can be prevented, unlike other reproductive cancers through effective screening programs. 12 According to an estimate in 2012, there were about 4732 cervical cancer deaths which occurred annually making cervical cancer the 2nd leading cause of female cancer deaths in Ethiopia. As well as being the 2nd leading cause of cancer mortality in women aged 15-44 years. This implies there will excessive life loss due to the disease unless prompt intervention like screening and vaccination is undertaken. 8 Early screening and vaccination are some prevention strategies for cervical cancer. However, the risk of death from complications related to cancer of the cervix may be mainly affiliated to health problems over the course of a woman’s life in low income countries. 13 Vaccination can be viewed as primary prevention, with screening as secondary prevention. 12
Even though the cause for many cancers remains unknown, established cancer causes include external factors like lifestyle, such as tobacco use and excess body weight, and non-modifiable judged as internal factors, including inherited genetic mutations, hormones, and immune conditions are contributors. 14 The peak age of incidence was between 40 and 49 years. Most of the cases were found in Addis Ababa, where the hospital is situated. An increase in the trend of cervical cancer cases was observed. 2 In addition, in Ethiopia, early sexual activity, high HIV prevalence, and low socioeconomic status may place women at risk for cervical cancer. 15
It is estimated that about 1-2% of women have CIN2 + each year. This rate is reported to be higher for HIV-positive women, at 10%.1-5,16 In high-income countries, regular Pap smear tests have been shown to reduce the risk of developing cervical cancer, by detecting malignant mutations. 17 As the problem is escalating in low and mid-income countries, interventions like using visual inspection with acetic acid has been revealed to be effective for screening in precancerous lesion low resource settings. 18
Cervical cancer is preventable, however many women in low-income countries do not have access to effective screening programs. Ethiopia has no standard policy or protocol for cervical cancer screening, rather it is patchy or inconsistent. Ethiopian women typically present for cancer care at a late stage in the disease, where treatment is likely ineffective. 19 There are no specific symptoms and no clinical features indicating the presence of a CIN. Many of these lesions, however, may become white when 3-5% acetic acid is added and possibly iodine-negative in the use of Lugol’s iodine solution, as the CIN epithelium contains little or no glycogen. 20 Like that of colorectal cancer screening, this procedure can help to prevent cervical cancers by giving opportunity for early identification and removal of precancerous lesions. It also provides the chance to identify as early as possible, when treatment is less extensive and more likely to be successful. Furthermore, screening is known to contribute in decrement of death from cancers including cervical cancer. 14 However, lack of funding for diagnostic services, low awareness of testing, and lack of trained health professionals are also major challenges in diagnosing and treating cervical cancer. 21
Reducing the magnitude and tackling the factors related with precancerous lesion is very important. As it is very crucial to produce significant decreases in incidence and mortality from precancerous lesion, barriers should be identified. Therefore, this study is aimed at determining the magnitude of this lesion within the study area and factors contributing to the problem. 22 Every woman has the right to be screened for cervical cancer at least once in her lifetime. However, in resource-poor settings, 30–49-year-old women comprise the target audience because cervical cancer is rare in women under 30 and most common in women over 40 years. Screening younger women will detect many lesions that will never develop into cancer, will lead to considerable overtreatment, and is not cost-effective.1,23 In the same manner, the World Health Organization set priority to be given to screening women aged 30-49 years in the general population of women. 23 In Ethiopia according to the population census of 2013 EFY/2020/21 G.C projected estimate of women aged 30-49 years comprises approximately 19.2% of the total population. 1 To the best of author’s knowledge, prevalence, and factors for precancerous cervical lesions, have not been studied yet in study area. Therefore, this study will serve for clinicians, policy makers, and program planner’s designers as a resource for the design of appropriate interventions to decrease cervical cancer in areas like vaccination, early screening, and awareness creation. Further, the results of the study may serve as baseline information for future research.
Method and Materials
Study Area, Population, Source, Design
This study was conducted in selected hospitals of West Wollega, which is found in Oromia National Regional State, located at a distance of 441 km from Addis Aba. It has a total population of 1,951,933 (Urban %13 Rural 87%). Five government hospitals, two NGO hospitals, 67 health centers, and 560 public health facilities are currently functional. Data were collected from January 1-February 20/2022. The participants were selected from all women of age 30-49 years’ living in the West Wollega zone, while all selected women of age between 30 and 49 years attending pre-cervical cancer screening at West Wollega Hospitals and selected health centers were studied by institutional-based prospective analytic cross-sectional study design was employed.
Sample Size Determination and Sampling Procedure
The sample size was calculated using a single population proportion formula; considering 27.7% as the prevalence of pre-cervical cancer among clients screened in Southern Ethiopia, 3 5% margin of error, and a 10% estimated non–response rate.Where, n = the sample size required.N= Number of householdsP = 27.7% prevalence of pre-cervical cancer among clients screened in Southern Ethiopiad = margin of sampling error tolerated Zα/2 = the standard normal variable at (α-1) or 95% confident level = 1.96
Since the total population is >10,000 no need for a correction formula:
The sample size was found to be 308. By adding a 10% non-response rate the final sample size is 339.Hospitals and health centers providing routine cervical cancer screening and treatment using VIA and cryotherapy services were purposively selected

Data Collection Instruments and Procedure
Data were collected through face-to-face interviews with a structured questionnaire that was initially adapted from previous studies. 4 The questionnaire was prepared in English, translated to Afan Oromo, and then back to English to check the consistency. Ten BSc nurses and five supervisors were assigned for data collection and supervision.
Data Quality Control
One-day orientation was given for data collectors and supervisors to ensure the quality of the field operation by principal investigators. Supervisors supervised the data collection process on daily bases and check the quality of collected data. The data collection tool was pre-tested on 5% of the sample at Arjo health center. Based on the findings and feedback obtained from the pre-testing process, a modification was made to the questionnaire.
Data Processing and Analysis
The data were entered into Epi-data version 3.2 and analyzed by SPSS version 25.0 for further analysis and interpretation. Descriptive analysis was carried out for each of the variables to check frequency, distribution, and missing values. Variable with a p-value of <.25 on bi-variable analysis were entered into a multivariable logistic regression to identify predictors of pre-cancerous lesion of the cervix. The odds ratio at 95% confidence intervals was used to quantify the degrees of association. Results with a p-value ≤.05 were considered as being statistically significant
Operational Definition and Definition of Terms
Ethical Consideration
Ethical Clearence letter was obtained from the West Wollega Zonal Health Department research, ethics review committee with reference number 199/WEFGL/13, Date-12/12/13, and then a formal letter was written to all Hospitals and health centers included within the study before data collection. All study participants were provided information about the study purpose and confidentiality of information. The participants were informed to withdraw participation at any point if they felt discomfort. Written informed consent was obtained from each study participant.
Results
Socio-Demographic Characteristics of the Study Participants
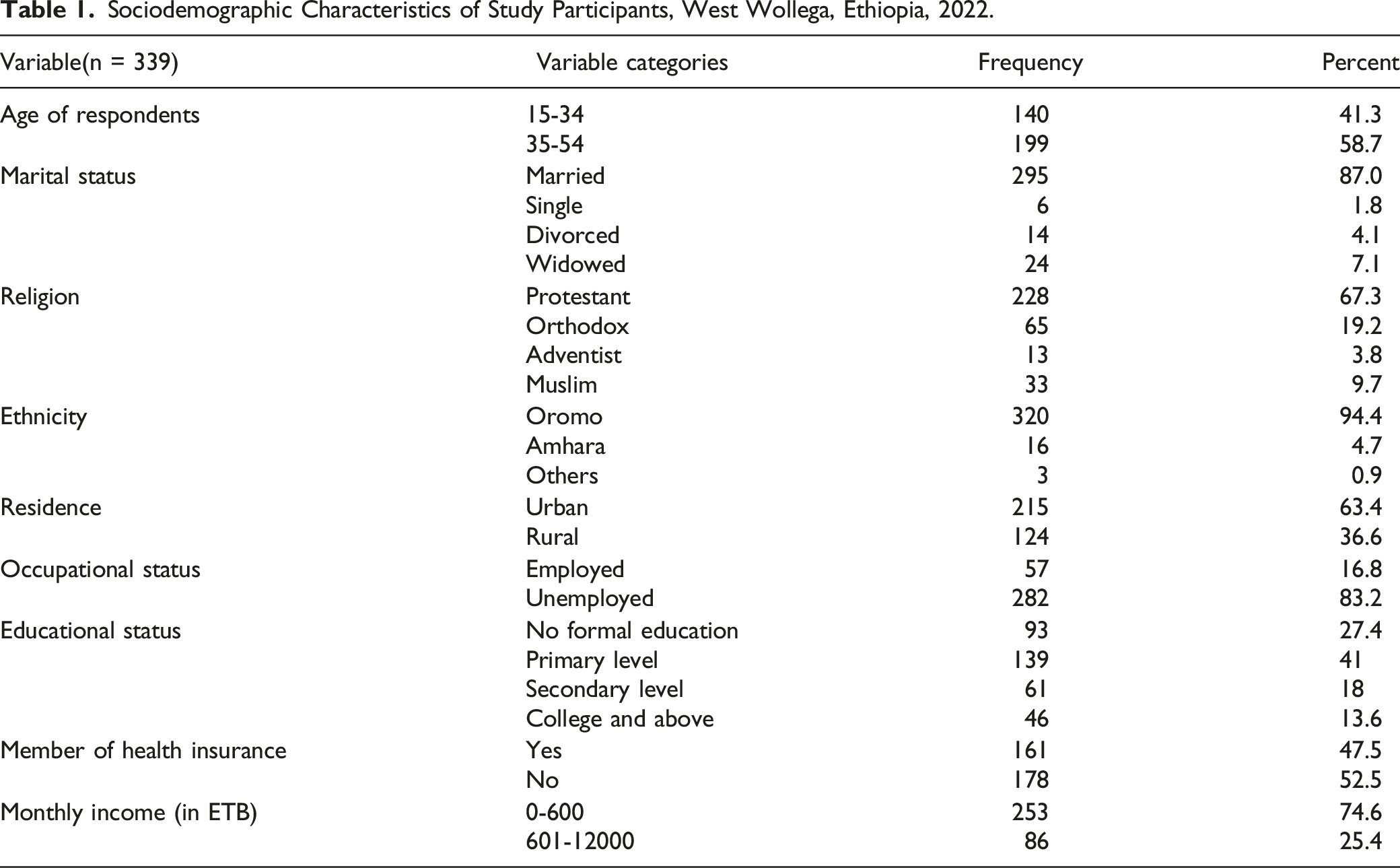
Sociodemographic Characteristics of Study Participants, West Wollega, Ethiopia, 2022.
Obstetrics and Gynecological History
Obstetrics and Gynecological Related History of Study Participants, West Wollega, Oromia, Ethiopia, 2022.

Knowledge of Precancerous Cervical Lesion Risks, Signs, Prevention, and Consequence
Knowledge Status of Respondents Regarding Precancerous Cervical Lesion, West Wollega, 2022.

Level of Attitude
Attitude Level of the Study Participants, West Wollega, 2022.

Prevalence of Precancerous Cervical Lesion Among Study Participants
Crude and Adjusted Odds Ratios of Factors Associated with the Precancerous Cervical Lesion, West Wollega, Ethiopia, 2022.

1=Reference
aStatically significant
Factors associated with precancerous cervical lesion
In multivariable analysis, participants with a diagnosis of menstrual irregularity had a two folds higher odds of being diagnosed with the precancerous cervical lesion when compared with counterpart at, [AOR=2.29(95%CI:1.29-4.04]. Women with history of STI had 3.5 times higher odds of developing precancerous cervical lesion compared to women with no history of STI [AOR)=3.46(95%CI:1.94-6.18)]., Women having bleeding after sexual intercourse were 2.88 times more likely to have precancerous cervical lesion compared to those without it at [AOR=2.88(95%CI:1.43-5.78)]. Women with parity greater than or equal to five had 2.4 times higher odds of developing precancerous cervical lesions compared to women with parity less than five at [AOR=2.41(95%CI:1.23-4.75)]. Participants who had a history of steroid use had 3.5 times higher odds of developing precancerous cervical lesion compared to participants with no history of steroids use at [AOR=3.5(95%CI:1.32-9.34) and women with an unfavorable attitude towards screening for cervical cancer screening, prevention, and control methods had 2.2 times higher odds of developing precancerous cervical lesion compared to women with favorable attitude towards screening, prevention, and control methods [AOR=2.15(95%CI:1.21-3.83)] (Table 5).
Discussion
The findings of this study are in line with the results of a study from the city of Arba Minch and the Zuria region (27.7%) and are higher than those reported in Easter Ethiopia, Harar (18.5%), three referral hospitals of Amhara region 20.2%, and Jimma (12.9%).3,5,10,13 Furthermore, the findings were significantly higher than systematic reviews conducted in Ethiopia, 24 Southern Ethiopia 22%,25-26 Dessie 6.9%, Waldia and Dessie 9.9%, 27 Almeda textile factory in North Ethiopia 6.7% 28 and Rwanda. 18 This reveals that the findings recommend raising of a screening strategy for cervical intraepithelial neoplasia for all women. 13
In this study, 63.4% of study participants were well-informed about cervical cancer. The findings were higher than the study results in Butajira and Wolita of Ethiopia. On the other hand, the study also revealed that 67.6% of women interviewed had a positive attitude toward cervical smear screening under the results reported in Bishoftu town.16,17,29
Participants with a diagnosis of menstrual irregularity had a statistically significant higher odds of association [AOR=2.29(95%CI: 1.29-4.04] for being diagnosed with a precancerous cervical lesion of the cervix, which is in line with research done in Debre -Berhan University. 22 This might be a reason of other causes of abnormal menstruation including uterine cancer or cervical cancer. 20 As well, sometimes cervical cancer mimics menstrual bleeding. The patient may notice a longer or heavier menstrual cycle than usual or spotting or bleeding between periods 24
Women having STI had 3.5 times higher odds of developing precancerous cervical lesions compared to women with no history of STI [AOR) = 3.46(95%CI:1.94-6.18)], which is similar to research conducted in the Debre Markos town, 30 Southern Ethiopia, 25 and three referral hospital in Amhara region. 5 This association might be due to that the fact that cervical cancer occurs in the cervix, which is the entrance to the uterus. More than 90% of cervical cancers develop due to persistent infection of the human papillomavirus (HPV), which is most often transmitted through sexual intercourse. 21 It is clear that STI are a result of having sexual partners. In another way, having multiple sexual partners escalates the risk of getting HPV, and in turn, can lead to the development of cervical pre-cancer lesions. 13 As well, it is clear that nearly all cases of cervical cancer result from infection with HPV, and the prevention of cervical cancer includes screening and vaccination. 12
Women having a history of bleeding after sexual intercourse were more likely to have precancerous cervical lesions [AOR=2.88(95%CI: 1.43-5.78)] compared to their counterparts. This is in line with a study in Beijing. 31 Bleeding during or after sex can be alarming, especially if the mothers were not menstruating. 32 The most likely causes include a sexually transmitted infection, benign polyps, cervical ectropion, atrophic vaginitis, endometriosis, trauma, and cancer. 33 The results suggest that to prevent precancerous cervical lesions one must consider changes of lifestyle and sexual behavior. 34
Women with parity greater than or equal to five had 2.4 times higher odds of developing precancerous cervical lesion compared to women with parity less than five [AOR=2.41(95%CI: 1.23-4.75)], which is in line with Johannesburg South Africa, 35 this might be due to that high parity increases the risk of squamous-cell carcinoma of the cervix among HPV-positive women. A general decline in parity might therefore partly explain the reduction in cervical cancer recently seen in most countries. 36
Women with an unfavorable attitude had 2.2 times higher odds of developing precancerous cervical lesions compared to women with a favorable attitude [AOR=2.15(95%CI:1.21-3.83)]. This is in line with research done in Hawassa town
36
and an overall score of attitudes was 67.6%. This finding was lower than research conducted among Adama Science and Technology University Female Students which was (71.7
Conclusions and Recommendations
Precancerous cervical lesions continue to be a significant public health concern in Ethiopia. It will remain a cause of death of women unless effective screening methods like VIA and vaccination to HPV are scaled up. Furthermore, having history of menstrual irregularities, STI, bleeding after coitus, parity greater ≥5, steroid use, and having unfavorable attitude towards screening factors are significantly associated with occurrence of precancerous lesion. This implies that clinicians can play a pivotal role in the prevention of advancement of the lesion to cancer as majority of the factors can be identified during early. Therefore, effective prevention approaches have to consider these factors for the control of cervical cancer in early phase of lesions.
List of Abbreviations/Acronyms
ASIR-Age-Standardized Incidence Rate, CIN 2 and CIN 3_Cervical Intraepithelial Neoplasia, CC- Cervical Cancer, DNA –Deoxyribose Nucleic Acid, DALYs -Disability-Adjusted Life-Years, WHO-World Health Organization, HIV- Human Immune-Virus, LSES-Low Socioeconomic Status, OR-Odd Ratio, SSA-Sub-Saharan Africa, STI-Sexually Transmitted Infection, STD-Sexually Transmitted Diseases, NGO- Non-Governmental Organization, HPV-Human Papilloma Virus, VIA- Visual Inspection with Acetic acid
Footnotes
Acknowledgments
We thank the data collectors and study participants.
Author’s contributions
KE and GF have been involved in the conception, writing the study protocol, formulating of the study design, and have provided training for data collectors, data entry, analysis, and interpretation of data. KE, MT, and LM participated in the design, interpretation of data, reviewing of intellectual content; supervising the overall process of the process, and manuscript preparation and they have provided important comments to supervise the overall process and review the manuscript. All authors have reviewed and approved this article’s final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the West Wollega Zone Health Office funded this studys data collection However the funder’s have no role designing study, analyzing and publishing this work.
Ethical Approval
Ethical Clarence letter was obtained from the West Wollega Zonal Health Department research, ethics review committee with reference number 199/WEFGL/13, Date-12/12/13, and then a formal letter was written to all Hospitals and health centers included within the study before data collection. All study participants were convinced a bout study purpose and confidentiality of information. The participants were informed to withdraw participation at any point they feel discomfort. Written informed consent was obtained from each study participants.
Data Availability
All the data and materials are available with the authors.