
Abstract
Introduction
Pancreatic neuroendocrine tumors (PanNETs) have shown an increasing incidence, yet population-based studies examining the clinical characteristics and cancer-specific survival (CSS) specifically in adolescents and young adults (AYA) (aged 13-39 years) remain scarce.
Methods
This population-based, retrospective cohort study identified all patients diagnosed with PanNETs through the Surveillance, Epidemiology, and End Results (SEER) database. Propensity score matching (PSM) was adopted to reduce selection bias. Kaplan-Meier analyses and Cox proportional hazards models were used to evaluate the impact of demographic and clinical variables on CSS. Temporal trends in incidence by age group were also assessed over the study period.
Results
A total of 4408 patients were included, with 338 in the AYA group and 4,070 in the older adult (OA) group (aged ≥ 40 years). Compared to the OA group, the AYA group had more female patients, earlier clinical staging, lower distant metastasis rates, and higher surgical treatment rates (P < 0.05). The AYA group exhibited better CSS (P=0.005). After PSM, the AYA group and the OA group had comparable CSS (P=0.261). Multivariate Cox regression analysis identified N stage and surgery as independent risk factors for CSS in the AYA group.
Conclusions
In this study, distinct clinical characteristics of AYA patients with PanNETs were identified compared with older adults. In this observational analysis, after PSM, CSS rates were similar between the two age groups, despite baseline differences before matching. The rising incidence of PanNETs in AYA individuals suggests a need for continued surveillance and personalized management in this young population.
Keywords
Introduction
Pancreatic neuroendocrine tumors (PanNETs), originating from the neuroendocrine system, represent a distinct category of pluripotent stem cell tumors that constitute approximately 3%-5% of all pancreatic neoplasms.1-3 Depending on their cellular lineage, PanNETs can be categorized as carcinoid tumors, insulinomas, APUD tumors, gastrinomas, vasoactive intestinal peptide tumors, glucagonomas, and others.4,5 Furthermore, based on their clinical manifestations, these tumors can be classified as either functional or non-functional.6,7 Recent advancements in diagnostic methods and heightened awareness of endocrine tumors have led to an increase in the identified cases of PanNETs, particularly among the younger demographic. According to the National Cancer Institute’s registry, the United States witnesses an estimated 1,000 new cases of PanNETs annually. 8
Although previous investigations have delved into the clinicopathological attributes and prognostic outcomes of PanNETs,9-12 substantial disparities exist between the elderly and young patient cohorts concerning physiological functions, disease incidence, mortality rates, clinicopathological features, psychological well-being, treatment responses, and overall prognosis. Notably, research exclusively focused on the younger patient population is still lacking. The definition of adolescents and young adults (AYA) varies across studies; however, it is commonly defined as individuals aged 13-39 years in population-based cancer research.13,14 Recently, there has been a notable surge in cancer research specifically targeting the AYA population.15-17 Nonetheless, studies pertaining to PanNETs in this age group are conspicuously absent. To bridge this knowledge gap, our study leverages the extensive data from the Surveillance, Epidemiology, and End Results (SEER) database. Unlike prior studies that either focused on older populations or examined overall survival without accounting for selection bias, we provide the first large-scale, population-based analysis of clinical characteristics and cancer-specific survival (CSS) specifically in AYA patients with PanNETs. Notably, this study is the first to apply propensity score matching (PSM) to compare CSS between AYA and older adult groups, thereby minimizing confounding and yielding more reliable comparisons. We aimed to provide clinicians with valuable insights into treating a distinct patient population by conducting a comprehensive analysis of the clinical characteristics and CSS rates of AYA patients specifically diagnosed with PanNETs in the United States. In this study, we hypothesized that AYAs diagnosed with PanNETs may present with distinct clinical characteristics and may have better CSS compared to older adults. Furthermore, we sought to identify independent prognostic factors specific to this understudied population. A preprint version of this study is available at https://doi.org/10.21203/rs.3.rs-4242353/v1.
Methods
Patient Selection
This population-based, retrospective cohort study centered on patients with pancreatic neuroendocrine neoplasms diagnosed between 2000 and 2020, using data from the SEER database (accessible at https://seer.cancer.gov). These patients were identified based on the International Classification of Diseases for Oncology, 3rd Edition (ICD-O-3) histology code 8240/3 (carcinoid tumor, NOS) and primary site codes corresponding to the pancreas, ensuring that only pancreatic primaries were included. The exclusion criteria consisted of: (1) unknown pathological histological diagnosis; (2) unknown survival information; (3) patient aged less than 13 years; (4) diagnosis other than PanNETs. Figure 1 depicts a flowchart outlining the study protocol. The analyzed variables encompassed age, race, sex, American Joint Committee on Cancer (AJCC) staging, TNM stage, tumor size, marital status, surgical intervention, radiation, chemotherapy administration, follow-up duration, and vital status. Participants were divided into two age groups: AYA (aged between 13 and 39) and older adults (OA) (40 and above). Racial categories included white, black, and an “other” category combining American Indian, Alaska Native, Asian, and Pacific Islander. Marital status was categorized as either married or unmarried, with the latter encompassing those who were divorced, separated, single, or widowed. The primary objective was to evaluate CSS rates among patients with PanNETs. These rates were calculated from the time of diagnosis to cancer-related death, or the most recent follow-up. Given that the SEER database consists of de-identified, publicly accessible information, this research did not involve human subjects, and all patient data have been anonymized. Thus, institutional review board (IRB) approval and informed consent were not necessary. This study was conducted in accordance with the Helsinki Declaration of 1975, as revised in 2024. The reporting of studies conducted using observational routinely-collected health data (RECORD) statement was followed.
18
Patients were selected from the SEER database according to the specified histological and temporal criteria, constituting a population-based cohort rather than a consecutive, random, or selectively enrolled sample. Flowchart of patient selection. A total of 4,408 patients diagnosed with pancreatic neuroendocrine tumors (PanNETs) between 2000 and 2020 were included. After 1:6 propensity score matching (PSM), the adolescent and young adult (AYA) group (aged 13-39 years, n=338) and the older adult (OA) group (aged ≥ 40 years, n=2,028) were well-balanced for baseline characteristics
Multiple Imputation
To address missing data in various variables, such as race (0.8% of cases), AJCC stage (8.3% of cases), T stage (5.6% of cases), N stage (5.3% of cases), M stage (5.3% of cases), tumor size (7.6% of cases), marital status (5.4% of cases), and surgery (0.4% of cases), the random forest method was employed using the R software (version 4.1.0) for multiple imputation (MI).
Statistical Analysis
Categorical variables were presented as frequencies and percentages, with comparisons between groups conducted using the Chi-square test. For continuous variables that did not conform to a normal distribution, the median and interquartile range (IQR) were used as descriptors, and comparisons between groups were facilitated by the Mann-Whitney U test. To minimize selection bias and balance baseline characteristics between the AYA and OA groups, we performed PSM using a 1:6 nearest-neighbor matching algorithm without replacement. The propensity score was estimated using a logistic regression model that included the following covariates: age, race, sex, marital status, AJCC stage, T stage, N stage, M stage, tumor size, surgery, radiation, and chemotherapy. A caliper width of 0.01 was applied to ensure adequate matching quality. Standardized mean differences (SMDs) were calculated for all covariates before and after matching, with an SMD < 0.1 considered indicative of adequate balance. The Kaplan-Meier method was adopted to evaluate CSS, and comparisons between groups were aided by the log-rank test. Hazard ratios (HRs) and 95% confidence intervals (CIs) were obtained from both univariate and multivariate Cox proportional hazard models. Variables deemed significant (P < 0.05) in the univariate Cox regression analysis were subsequently incorporated into the multivariate analysis. Temporal trends in incidence rates were assessed using Joinpoint regression analysis. All statistical computations were executed using R software (version 4.0). A P-value of less than 0.05 was deemed statistically significant in determining disparities between groups.
Results
Patient Characteristics
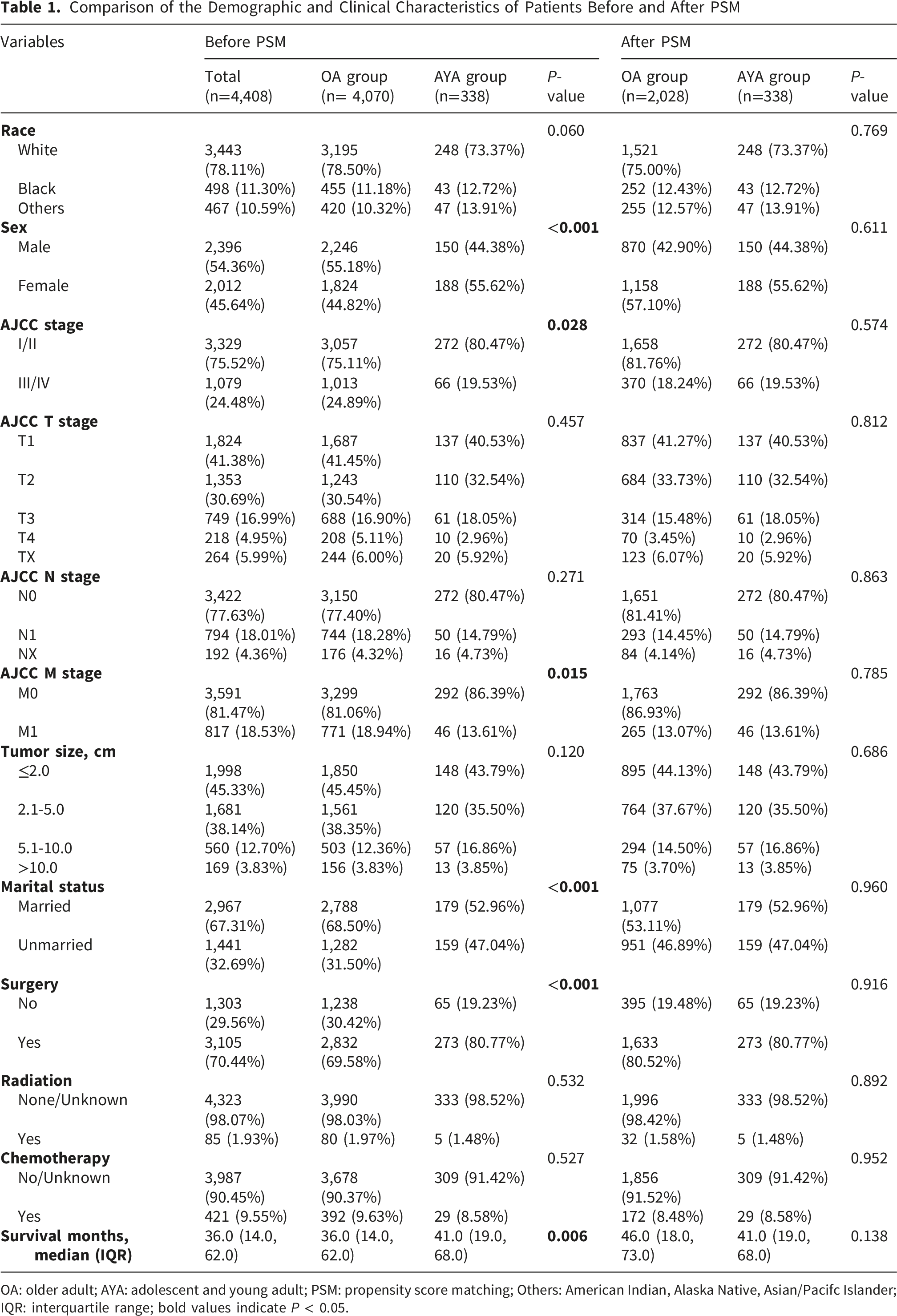
A total of 4408 patients were included in the study, with 338 in the AYA group and 4,070 in the OA group. Throughout the 21-year timeframe spanning from 2000 to 2020, the age-adjusted incidence rate of PanNETs among AYA patients showed a significant upward trend (P for trend < 0.05), increasing from 0.004 per 100,000 in 2000–2002 to 0.136 per 100,000 in 2018–2020 (Figure 2). Throughout the 21-year timeframe spanning from 2000 to 2020, AYA patients diagnosed with PanNETs were categorized into seven 3-year periods, revealing a noticeable increase in the incidence rate (Figure 2). Before PSM, notable disparities existed between the two groups in regard to sex, AJCC stage, M stage, marital status, and surgery (P < 0.05). After 1:6 PSM, there were 338 patients in the AYA group and 2028 patients in the OA group. There was no statistically significant difference in baseline data comparison (P > 0.05) (Table 1). Table 1 presents a comprehensive overview of the patients’ demographic and clinical information, whereas Supplementary Table 1 gives a thorough comparison of these features between the two groups before MI. Age-adjusted incidence rates of pancreatic neuroendocrine tumors (PanNETs) among adolescents and young adults (AYA) from 2000 to 2020. Incidence rates are presented per 100,000 population across seven 3-year intervals. A significant increasing trend was observed over the study period (P for trend < 0.05) Comparison of the Demographic and Clinical Characteristics of Patients Before and After PSM OA: older adult; AYA: adolescent and young adult; PSM: propensity score matching; Others: American Indian, Alaska Native, Asian/Pacifc Islander; IQR: interquartile range; bold values indicate P < 0.05.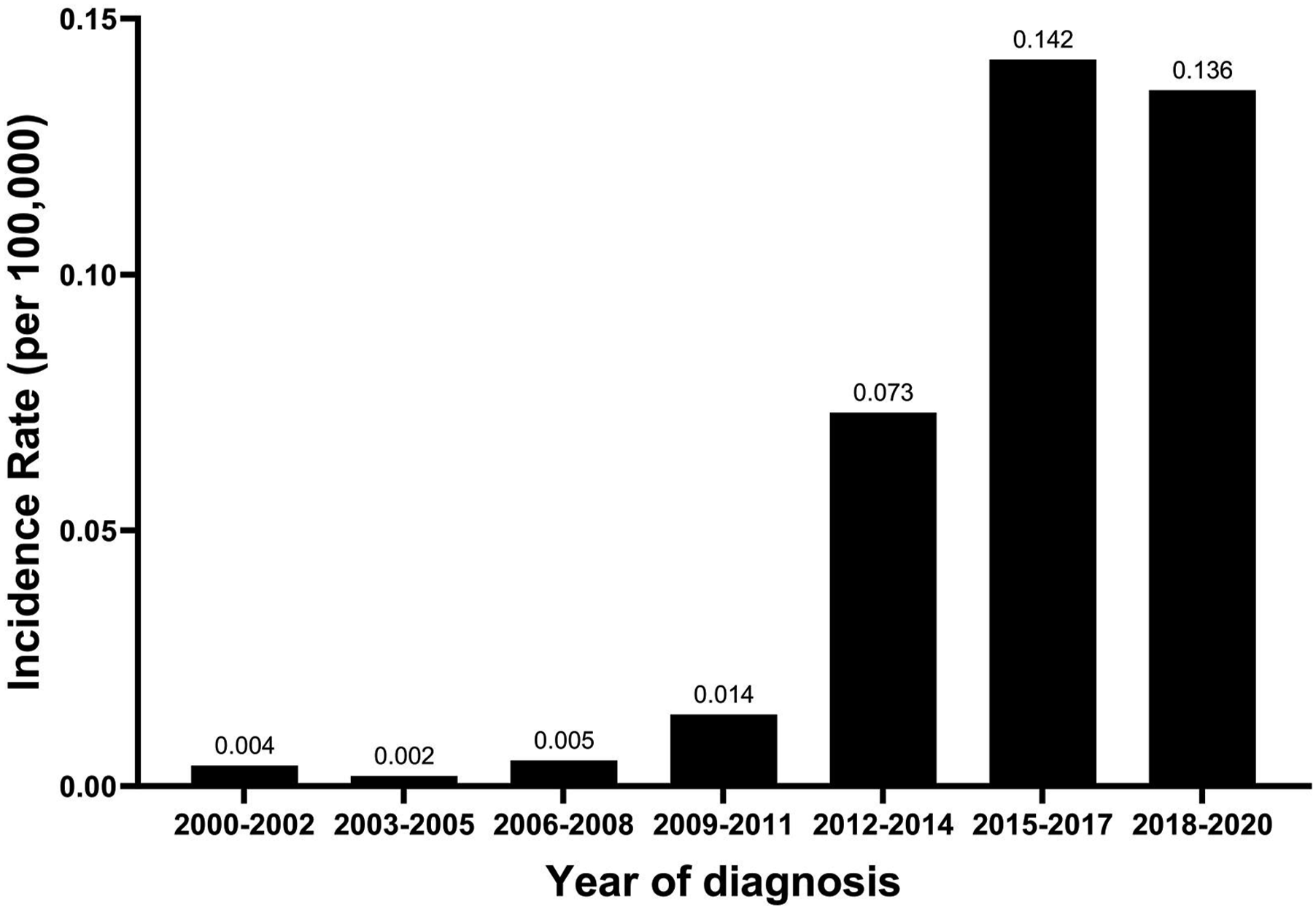
Survival Analysis of Patients With Pancreatic Neuroendocrine Tumors
Survival Rate of Patients With Pancreatic Neuroendocrine Tumors in the OA Group and AYA Group

OA: older adult; AYA: adolescent and young adult; PSM: propensity score matching; bold values indicate P < 0.05.

Cancer-specific survival (CSS) curves for adolescent and young adult (AYA) and older adult (OA) patients with pancreatic neuroendocrine tumors (PanNETs). (A) Before propensity score matching (PSM), the AYA group demonstrated significantly better CSS than the OA group (HR = 0.57, 95% CI: 0.38–0.85, P = 0.005). (B) After PSM, no significant difference in CSS was observed between the two groups (HR = 0.79, 95% CI: 0.52–1.19, P = 0.261)
Univariate and Multivariate Cox Regression
Univariate and Multivariate Cox Regression to Analyze the Cancer Specific Survival of Patients With Pancreatic Neuroendocrine Tumors in the AYA Group

AYA: adolescent and young adult; Others: American Indian, Alaska Native, Asian/Pacifc Islander; HR: hazard ratios; CI: confidence interval; bold values indicate P < 0.05.
Subgroup Analysis
Before PSM, the CSS of the AYA group was superior to that of the OA group, particularly within specific subgroups such as Caucasians, females, those in AJCC stages I/II, patients in the N0M0 category, married individuals, and those who were not subjected to radiotherapy or chemotherapy (P<0.05) (Figure 4). However, after PSM, the CSS of the AYA group was comparable to that of the OA group (P>0.05), except in the AJCC stages I/II and N0 stage subgroups where the CSS of the AYA group was superior to the OA group (P<0.05) (Figure 5). Subgroup analysis of cancer-specific survival (CSS) between adolescent and young adult (AYA) and older adult (OA) patients with pancreatic neuroendocrine tumors (PanNETs) before propensity score matching. Hazard ratios (HRs) and 95% confidence intervals (CIs) are shown for each subgroup. The AYA group showed superior CSS in several subgroups, including white patients, females, AJCC stage I/II, N0, M0, married individuals, and those not receiving radiotherapy or chemotherapy (P < 0.05) Subgroup analysis of cancer-specific survival (CSS) between adolescent and young adult (AYA) and older adult (OA) patients with pancreatic neuroendocrine tumors (PanNETs) after propensity score matching. Hazard ratios (HRs) and 95% confidence intervals (CIs) are presented. The AYA group maintained a CSS advantage only in the AJCC stage I/II and N0 subgroups (P < 0.05), while overall CSS was comparable between the two groups

Discussion
In this population-based study, we leveraged the SEER database to characterize the clinical presentation and cancer-specific survival of AYAs with PanNETs—a demographic that remains understudied in the neuroendocrine tumor literature. The observation that AYA patients presented with earlier-stage disease and lower rates of distant metastasis suggests that younger age may be associated with a more favorable disease phenotype at diagnosis. This could reflect either inherent biological differences in tumor behavior or differences in healthcare-seeking behavior and diagnostic intensity. Additionally, the higher rate of surgical intervention in the AYA group may indicate a more aggressive treatment approach in younger patients, which may independently contribute to outcomes. These findings underscore the importance of considering age-related clinical patterns in risk stratification and treatment planning. These observations suggest that AYA patients with PanNETs tend to present with less advanced disease and have improved access to surgical procedures. This may be attributed to early disease detection or a more proactive therapeutic approach adopted for this age group. Our findings align with previous studies by Mei et al. 19 and Shi et al., 20 which also reported a higher proportion of surgical treatments in the young group compared to the elderly. Shi et al. 20 and Goksu et al. 21 found in their studies that the proportion of black patients with PanNETs was higher among young patients than among elderly patients. However, our study found that the proportion of patients from different ethnic groups in the AYA group was similar to that in the OA group (P>0.05). Such disparities could potentially be attributed to variations in sample sizes and the duration of the studies. To our knowledge, this study represents the largest and most comprehensive population-based analysis of PanNETs in the AYA population to date. Its key novelties include: (1) a focused examination of CSS rather than overall survival, which more accurately reflects cancer-specific outcomes; (2) the use of PSM to reduce selection bias in survival comparisons; and (3) the identification of rising incidence trends and unique prognostic factors specific to AYAs. These findings fill a critical gap in the literature and have important implications for risk stratification and clinical management in this age group.
Additionally, we observed a significant upward trend in the incidence rate of PanNETs among AYA patients over the study period. Similar trends have been reported by Goksu et al. 21 and Yadav et al., 22 indicating a rising incidence of PanNETs among younger individuals. This observed increase is likely multifactorial. First, advances in diagnostic imaging—including endoscopic ultrasonography, computed tomography (CT), and magnetic resonance imaging (MRI)—have substantially improved the detection of small, previously occult PanNETs. 8 Second, the increasing use of cross-sectional abdominal imaging for unrelated indications has led to a rise in incidental diagnoses, particularly among younger patients who undergo imaging for other clinical reasons. Third, growing awareness of neuroendocrine tumors among clinicians and more accurate pathological classification over time may have contributed to increased case ascertainment. Additionally, changes in disease coding practices and the widespread adoption of standardized diagnostic criteria during the study period may have further influenced incidence estimates. While lifestyle factors and environmental exposures cannot be ruled out, the contribution of such factors remains speculative and requires further epidemiological investigation. Taken together, at least part of the observed increase likely reflects improved detection and diagnostic intensity rather than a true rise in disease burden.
Previous studies have consistently demonstrated that age plays a crucial role in determining the prognosis of patients with NETs, with younger patients exhibiting a more favorable prognosis.23-25 Nevertheless, there are limitations in the existing research. For instance, Han et al’s 25 study, while focusing exclusively on PanNETs’ overall survival (OS), encompassed only 104 patients, raising concerns about the generalizability of its findings. Similarly, despite a larger sample size, Halfdanarson et al’s 23 study was also confined to PanNETs’ OS analysis. In contrast, Caldarella et al. 24 provided a broader perspective by examining all NETs, but this comprehensive approach lacked specific insights into PanNETs. Compared to studying OS, studying CSS provides greater specificity in assessing the efficacy of cancer treatments. Meanwhile, CSS more precisely reflects the clinical benefits in specific disease contexts. Furthermore, improvements in CSS can directly inform clinicians’ treatment decisions specifically for cancer patients. Therefore, we analyzed the CSS of patients with PanNETs. Initially, we found that the AYA group had significantly better CSS outcomes compared to the OA group (HR 0.57, 95% CI 0.38-0.85, P=0.005) (Figure 3A). However, after PSM, the CSS of the AYA group became comparable to that of the OA group (HR 0.79, 95% CI 0.52-1.19, P=0.261) (Figure 3B). The comparable CSS between the two groups after PSM may be attributed to the similar biological behavior of PanNETs across different age groups, which results in comparable tumor growth rates and aggressiveness. Additionally, the widespread use of mature treatment modalities such as surgery, radiotherapy, and chemotherapy may have contributed to the significant improvement in the CSS of patients, regardless of age group.
Previous research has indicated that PanNETs are predominantly found in males in France, the United States, and Norway. 26 In this study, there were 2,396 male patients (54.4%) and 2,012 female patients (45.6%), similarly showing a higher proportion of male patients. However, we found that among the AYA population, the proportion of female PanNETs was higher than that of male patients (55.6% vs. 44.4%). The higher incidence of PanNETs in young female patients compared to males may be attributed to a combination of factors. Specifically, women’s physiological characteristics and genetic predispositions may make them more susceptible to this disease. Moreover, the lifestyle choices, dietary habits, and potential environmental exposures specific to modern young women might also increase their risk. Furthermore, the mental stress faced by women, coupled with their tendency to prioritize health management and actively participate in early screening compared to men, might contribute to the higher reported incidence of PanNETs among women in statistical data. However, further clinical research and epidemiological studies are needed to validate these hypotheses.
In this study, we found that the risk of death in AYA patients with lymph node metastasis (LNM) was more than six times higher than that in patients without LNM (Table 3). Studies by Krampitz et al. 27 and Curran et al. 28 also showed that patients with PanNETs and LNM had a poorer prognosis. The poor prognosis of patients with PanNETs and LNM is primarily due to the fact that LNM signifies the spread of the tumor, indicating disease progression and deterioration. Simultaneously, it affects the normal immune function of the lymphatic system, reducing the body’s resistance and making the tumor more prone to spread throughout the body. Furthermore, LNM implies that the tumor may have stronger invasive and metastatic capabilities, which not only increases the likelihood of metastasis to other organs but also limits treatment options and increases the difficulty of treatment. These factors combined contribute to the poor prognosis of patients with PanNETs and LNM. Surgery is the preferred treatment for PanNETs, especially for early-detected tumors. The type of surgery depends on the location and size of the tumor. Depending on the specific situation, options such as tumor resection, distal pancreatectomy, and pancreaticoduodenectomy can be chosen. Surgical treatment can improve the prognosis of patients with PanNETs.2,29,30 In this study, we also found that surgical treatment can improve the prognosis of AYA patients with PanNETs.
These findings carry several clinical implications. First, the observation that AYA patients present with earlier-stage disease and higher surgical resection rates suggests that this population may benefit from timely and aggressive surgical intervention. Second, the identification of lymph node metastasis as a strong independent predictor of CSS highlights the need for thorough nodal staging and consideration of lymphadenectomy during surgical resection in AYA patients. Third, the comparable CSS between AYA and OA groups after PSM implies that age alone should not dictate treatment intensity; instead, management decisions should be guided by tumor biology and stage. Collectively, these insights support the development of age-informed, stage-adapted clinical pathways for AYA patients with PanNETs.
The limitations of this study include several aspects. Firstly, the study population primarily represents the United States, limiting the generalizability of the findings to other global regions. Secondly, as with any registry-based study, several inherent biases should be acknowledged. Selection bias may arise from the retrospective, non-randomized design. Information bias is possible due to missing or miscoded data inherent to large administrative databases. Detection bias may be present given the increasing use of advanced imaging modalities over the study period (2000–2020), which could lead to higher diagnosis rates in later years. Referral bias should also be considered, as SEER data predominantly reflect the U.S. healthcare system. Thirdly, the SEER database lacks detailed pathological information, including tumor grade, Ki-67 proliferation index, and molecular markers, which are recognized prognostic factors for PanNETs. The absence of these variables may introduce unmeasured confounding and limit the granularity of our survival analyses. Fourthly, the study mentioned the impact of surgery on prognosis, but did not delve into the differences in effectiveness between various surgical methods, which may affect the accuracy of prognosis evaluation for patients. Fifth, the surgery variable was limited to whether surgical resection was performed, without detailed information on the type, extent, or radicality of surgery. This lack of granularity may affect the precision of treatment effect estimates and represents an inherent limitation of registry-based analyses. However, to our knowledge, this is the first large-sample, long-follow-up study on CSS of PanNETs in the AYA population.
Conclusion
In this population-based observational study using the SEER database, AYA patients with PanNETs display unique clinical features. After balancing baseline characteristics with PSM, CSS was comparable between AYA and older adult groups. AYA patients tend to present at earlier stages with lower metastatic burden and receive surgical treatment more frequently. Lymph node stage and surgery were independently associated with CSS in AYA patients, supporting the potential prognostic benefit of complete surgical resection with adequate nodal evaluation. These observational findings highlight the importance of early detection, stage-directed surgical intervention, and individualized management rather than age-based decisions alone. Sustained monitoring of the increasing incidence trend in this young population is warranted to facilitate early and appropriate intervention.
Supplemental Material
Supplemental Material - Clinical Characteristics and Cancer-Specific Survival of Adolescents and Young Adults With Pancreatic Neuroendocrine Tumors: A SEER-Based Study
Supplemental Material for Clinical Characteristics and Cancer-Specific Survival of Adolescents and Young Adults With Pancreatic Neuroendocrine Tumors: A SEER-Based Study by Lijun Huang, Fuli Gao, Jian Chen, Xiaodan Xu and Luojie Liu in Cancer Control.
Footnotes
Ethical Considerations
This study utilized de-identified data from the publicly available SEER database. As the research did not involve direct interaction with human subjects or the use of identifiable private information, ethical approval and informed consent were not required. The study was conducted in accordance with the Declaration of Helsinki and its subsequent amendments.
Author Contributions
Conception and design: Xiaodan Xu, Luojie Liu. Administrative support: Xiaodan Xu. Provision of study materials or patients: Lijun Huang, Fuli Gao, and Jian Chen. Collection and assembly of data: Luojie Liu. Data analysis and interpretation: Luojie Liu and Jian Chen. Manuscript writing: All authors. Final approval of manuscript: All authors.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Changshu Science and Technology Program (CY202339), the Suzhou Youth Science and Technology Project for the Advancement of Science, Education, and Health (KJXW2023067), Specialized Project for Clinical Key Disease Diagnosis and Treatment Technology in Suzhou (LCZX202334), and the Suzhou 23rd Batch of Science and Technology Development Plan (Clinical Trial Institution Capability Enhancement) Project (SLT 2023006).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.