
Abstract
Background:
The incidence of pancreatic neuroendocrine tumors (PNETs) has increased significantly. The purpose of this study was to analyze the clinical characteristics and prognosis of patients under 50 years old.
Methods:
Patients with PNETs recorded in the Surveillance, Epidemiology, and End Results (SEER) database from 2004 to 2015 were analyzed. The clinical characteristics were analyzed by Chi-square test. The Kaplan-Meier method was used to estimate overall survival (OS). Multivariate Cox proportional risk regression analysis was used to determine independent prognostic factors.
Results:
2,303 patients included, of which 547 (23.8%) patients were younger than 50 years old. The number of younger patients has increased steadily, while the proportion in total PNETs decreased recently. Compared with older group, the proportion of the Black, grade I/II, and surgery were higher in early-onset PNETs. Liver was the most frequent metastatic site. There was no significant difference in the incidence of different metastatic sites between younger and older PNETs patients, while younger patients had better OS (P < 0.05). Grade, N stage, M stage, and surgery were independent prognostic factors for OS in early-onset PNETs.
Conclusions:
Younger patients have unique clinicopathological characteristics compared with older patients in PNETs. Better OS was observed in younger patients which might due to the higher proportion of well-differentiated tumor and surgery than older patients.
Introduction
Although more than 90% of pancreatic cancer is ductal adenocarcinoma, the incidence rate of pancreatic neuroendocrine tumors (PNETs) is increasing. 1 From 2004 to 2012, the incidence of PNETs increased from less than 0.4 per 100,000 to over 0.8 per 100,000 in United States. 2 The 5-year overall survival rate for PNETs in early stages are 61.9%, and the 5-year survival rate for advanced cancers is less than 20%. 3
Previous studies have found that there are differences in clinical characteristics and prognosis between young and old in cancer patients including lung cancer, 4 colorectal cancer, 5 and so on. PNETs is a kind of highly heterogeneous tumor, however, the clinical characteristics and prognosis of young patients with PNETs had not been well studied. Patients with pancreatic cancer younger than 50 years old were considered to be early-onset individuals in recent studies. 6,7 Therefore, it is necessary to compare the clinical characteristics and survival rates of young PNETs patients with those of elderly patients through a large multicenter data set. In our study, the data of PNETs patients from 2004 to 2015 were collected by SEER database in order to study the clinical characteristics and prognosis of younger patients.
Materials and Methods
Patient Selection
Our study screened PNETs patients from 2004 to 2015 through the SEER database. Selection criteria: a. The pathological diagnosis was clear; b. Active follow-up; c. Single primary cancer. Exclusion criteria: a. The age, race, T stage, N stage, M stage and surgery status were unknown; b. Pathological reports come from autopsies or death reports. For this study, we signed the SEER research data agreement to access SEER information with the username10067-Nov2018. The SEER database is publicly available, so the approval and informed consent of the institutional review committee were not required in this study.
Variable Classification
Variables include age at diagnosis, race, sex, grade, primary site of tumor, T stage, N stage, M stage, surgery, chemotherapy, survival time and survival status. Finally, the whole study cohort was divided into 2 groups: <50 years old and ≥50 years old at the time of diagnosis. Race was divided into 3 groups as described in SEER database: white, black and other. Sex was classified as male and female. The grade was divided into 5 groups as described in SEER database: grade I (well differentiated), grade II (moderately differentiated), grade III (poorly differentiated), grade IV (undifferentiated) and unknown. 8 The TNM stage was according to the 6th edition of AJCC stage, which adapted to patients in the SEER database with a diagnosis time of 2004-2015 as previous studies described. 9 -11 The International Classification of Diseases for Oncology, Third Edition (ICD-0-3) codes was used to identify PNETs patients (8150-8153, 8155, 8240, 8241, 8246). 3 Primary site of tumor was classified into 4 groups: head, body, tail and others (including pancreatic duct, islets of Langerhans, other specified parts of pancreas, overlapping lesion of pancreas and pancreas, NOS). T stage was divided as T1, T2, T3 and T4. N stage was divided as N0 and N1. M stage was divided as M0 and M1. Status of surgery was classified as No and Yes. Chemotherapy was classified as No/ Unknown and Yes in SEER database. There was no record of detailed metastasis of distant organs in the SEER database before 2010. The definition and classification of distant organ metastasis were as described previously. 12 OS referred to the duration from diagnosis to any original death or last follow-up.
Statistical Analysis
We use SEER*Stat 8.3.5 to get the data, and use SPSS25 to analysis data. The difference of baseline data between the 2 groups was compared using Chi-square test. The overall survival rate was evaluated using Kaplan-Meier method, and was compared by log-rank test. Multivariate COX proportional regression risk model was used to determine independent prognostic factors, risk ratio and corresponding 95% confidence interval. There was significant difference between the 2 sides (p < 0.05).
Results
Clinical Characteristics
As shown in Figure 1, from 2004 to 2015, the number of younger patients had increased steadily, while the proportion in total PNETs decreased recently.

Trends in number and percentage of younger patients in the whole PNETs cohort during 2004-2015 in SEER database.
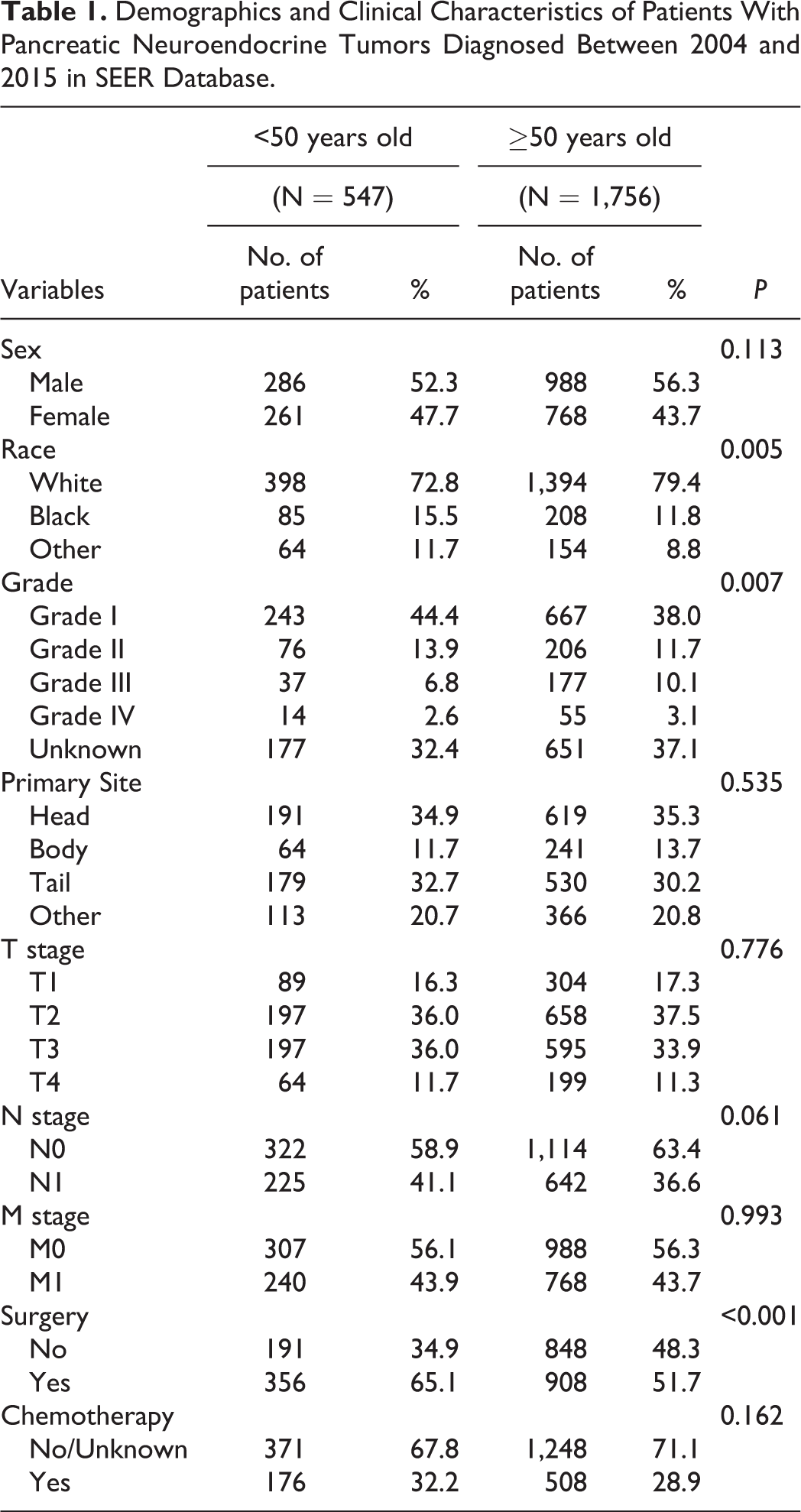
Finally, a total of 2,303 patients met the inclusion criteria, with 547 (23.8%) patients in the early-onset group. In terms of demographic characteristics, the proportion of Blacks in younger group was higher than that in older patients (15.5% vs 11.8%). There were no statistically significant differences in distribution by sex between early-onset and older groups (P = 0.113). In terms of tumor pathological characteristics, the proportion of well and moderately differentiated tumors was higher in younger group (58.3% vs. 49.7%). No significant differences were present in primary site, T stage, N stage and M stage between younger and older group. In terms of treatment, compared with the older group, the younger group was more likely to receive surgery (65.1% vs. 51.7%), however, there was no statistical difference between the 2 groups in chemotherapy (P = 0.162). More details were shown in Table 1.
Demographics and Clinical Characteristics of Patients With Pancreatic Neuroendocrine Tumors Diagnosed Between 2004 and 2015 in SEER Database.
Comparison of Metastasis Pattern and Prognosis Between Younger and Older Patients With PNETs
As shown in Table 2, in the young group with PNETs, single liver metastasis was the most common metastasis site, accounting for 32.4%. In addition, single organ metastasis had the highest incidence among different metastasis patterns (32.9%). More importantly, there was no significant differences in all metastasis patterns between young and elderly PNETs patients (P > 0.05).
Comparison of Organ Metastasis Patterns Between <50 and ≥50 Years Old Patients With Pancreatic Neuroendocrine Tumors Diagnosed Between 2010 and 2015 in SEER Database.

*: Fisher’s exact test.
**: Pearson chi-squared test.
***: Chi-squared test of continuity correction.
In patients with PNETs, the prognosis of younger patients was better than that of older patients as presented in Figure 2A (P < 0.001). In subgroup analyses, younger group without metastasis also had a significantly higher overall survival rate compared with older group (Figure 2B), as well as in patients with metastasis (Figure 2C) or with liver metastasis (Figure 2D) (P < 0.001).

Comparison of overall survival rates between the younger and older group of PNETs patients. A. The whole patients (P < 0.001); B. Patients without metastasis (P = 0.006); C. Patients with metastasis (P < 0.001); D. Patients with single liver metastasis (P < 0.001).
Prognostic Factors for Overall Survival Rate in Patients With PNETs
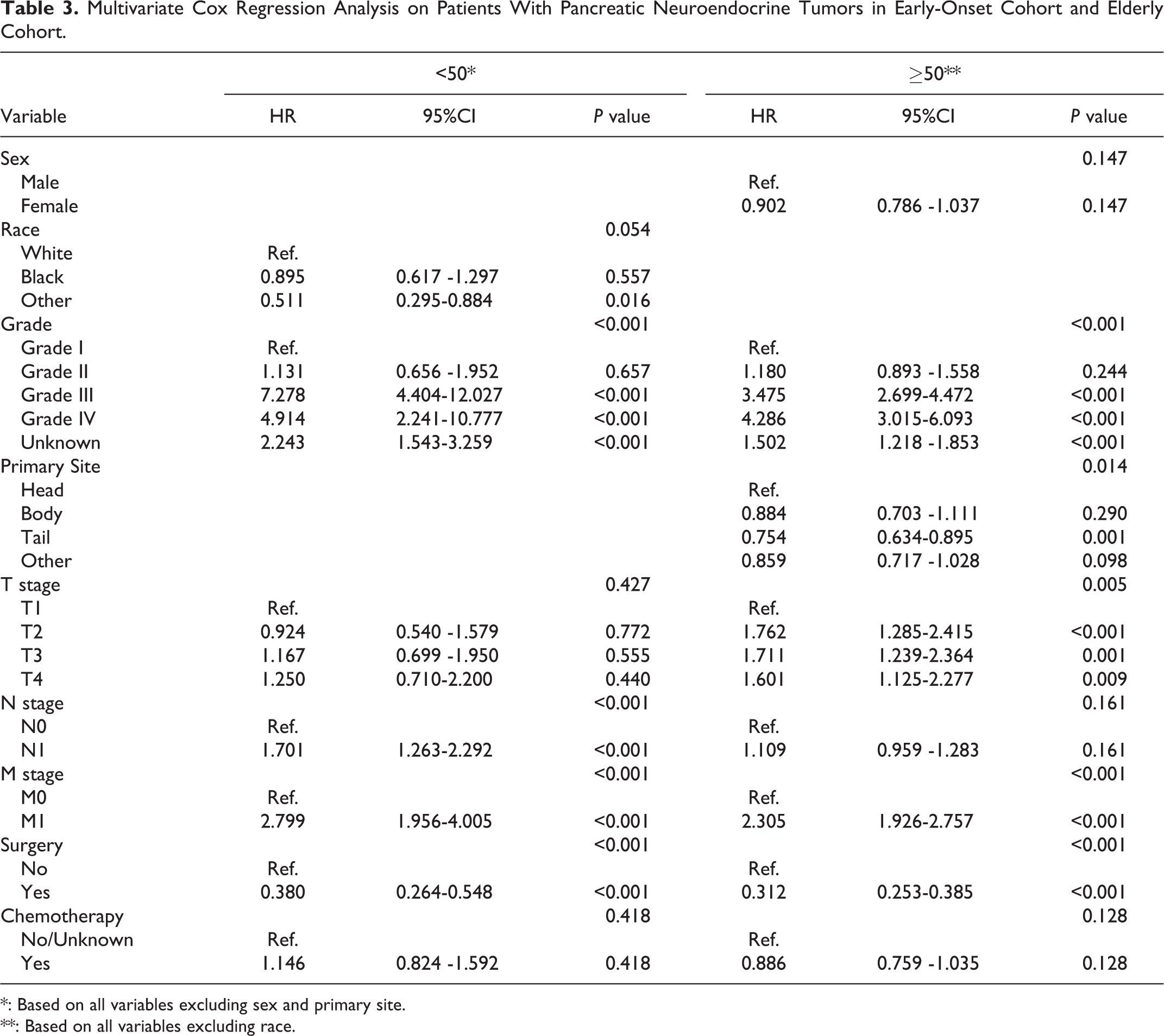
As shown in Table 3, grade, N stage, M stage, surgery were independent prognostic factors for OS in early-onset PNETs patients. The survival curves of these variables were presented in Figure 3. In details, patients with grade III/IV tumors had worse OS compared with patients with grade I/II tumors (HR:7.278, 95%CI:4.404-12.027, P < 0.001; HR:4.914, 95%CI:2.241-10.777, P < 0.001). The risk of death in patients with lymph node metastasis tended to be higher compared with those in lymph node-negative patients (HR:1.701, 95%CI:1.1.263-2.292, P < 0.001). Compared with early stage patients, patients with distant metastasis had worse OS (HR:2.799, 95%CI:1.956-4.005, P < 0.001). In addition, patients who underwent surgery had better OS than those with no-surgery (HR:0.380, 95%CI:0.264-0.548, P < 0.001).
Multivariate Cox Regression Analysis on Patients With Pancreatic Neuroendocrine Tumors in Early-Onset Cohort and Elderly Cohort.
*: Based on all variables excluding sex and primary site.
**: Based on all variables excluding race.

Overall survival rates curves for younger PNETs patients by (A) grade (P < 0.001); (B) N stage (P < 0.001); (C) M stage (P < 0.001); (D) surgery (P < 0.001).
In older group, multivariate analysis showed that grade, primary site, T stage, M stage, and surgery were independent factors for the prognosis. Detailly, patients with grade III/IV (HR:3.475, 95%CI:2.699-4.472, P < 0.001; HR:4.286, 95%CI:3.015-6.093, P < 0.001), larger tumor size (HR:1.601, 95%CI:1.125-2.277, P = 0.009), distant metastasis (HR:2.305, 95%CI:1.926-2.757, P < 0.001) had poor outcomes. In contrast, patients with pancreatic tail tumor (HR:0.754, 95%CI:0.634-0.895, P = 0.001) or received surgery (HR:0.312, 95%CI:0.253-0.385, P < 0.001) had better prognosis.
Discussion
Through the analysis of SEER database, our study found that younger patients had unique clinicopathological characteristics in PNETs patients. Younger patients, with or without distant metastasis, had better survival outcome than those older patients with PNETs. In addition, multivariate analysis was carried out to determine the independent factors affecting the prognosis of early-onset patients with PNETs.
The incidence of PNETs was increasing in recent years. 13 On the one hand, it might be related with the easy access to diagnostic tests like endoscopy, computed tomography, and magnetic resonance imaging. One the other hand, the current American Cancer Society (ACS) cancer screening guidelines might also contribute to this phenomenon. In this study, we found that the absolute number of PNETs patients with age younger than 50 years old had increased, which was broadly consistent with one published study based the National Cancer Database. 14 However, the proportion of younger patients in all PNETs was decreased in the past decade. Previous studies found that compared with patients younger than 50 years old, the older patients with neuroendocrine tumors demonstrated the highest absolute incidence rate and the rate of incidence was increasing faster. 15,16 Additionally, PNETs was more frequently occur in a younger group than pancreatic ductal adenocarcinoma as reported in other literatures. 17,18 Thus, although neuroendocrine carcinoma is a rare tumor, its high incidence rate in young patients must be emphasized in clinical practice.
Generally, different age of the patients resulted in clinical heterogeneity. In early-onset patients with PNETs, the rate of blacks was higher than that in older patients. Others who conducted similar research made similar findings. Suleyman et.al found that patients with early-onset PNETs were more likely to be blacks compared with the old (15% vs 11%). 14 Early-onset PNETs were prone to be well-differentiated. In contrast, younger patients were predominantly poorly differentiated in locally advanced cervical cancer 19 and triple-negative cancer. 20 The differences about the impact of age on tumor differentiation require further exploration. As far as we know, this was the first detailed comparison of metastasis patterns between younger and older patients with PNETs. We found that single liver metastasis had the highest incidence in both younger and older PNETs patients, which may be related to anatomical structure. Wang et.al also reported that liver was the most common metastatic site for PNETs. 21 There was no difference in incidence of different metastasis pattern between young PNETs patients and elderly patients, but the prognosis of younger patients with advanced tumor was better than that of elderly patients. This might be associated with the fact that younger PNETs patients were more likely to undergo surgery as we reported in this study. It has been confirmed that primary site surgery can reduce the risk of death of metastatic PNETs by 50%. 22 Although comorbidity status was not recorded in SEER database, prior work demonstrated that the Charlson age comorbidity index was higher in older patients than that in younger patients (70 years old vs 57 years old). 23 Comorbid conditions frequently impact cancer treatment decisions and are associated with OS and increased treatment-related toxicity and adverse events.
Multivariate analysis showed that the independent factors affecting the older cohort were not necessarily the same in younger patients, such as primary site, T stage and N stage. The reason for this difference is not clear, it might be that there were potential differences in molecular characteristics or immune-tumor pathway among different age groups, thus affecting the prognosis. 24 Poorly-differentiated tumors predict for a worse prognosis. The same finding has been reported in various tumors. 25 -27 In general, tumors with low differentiation grow faster than tumors with high differentiation. From the metabolic concept of tumor biology, poorly differentiated tumors had a higher SUV max of glucose uptake than moderately and well-differentiated tumors. 28 Lymph node and distant metastasis in early-onset patients with PNETs indicates a significantly poor prognosis, which was in agreement with several prior studies. 29,30 The 5-years overall survival rate for localized, regional and distant PNETs tumor were 94%, 76%, 31%, respectively. No differences were found in older patients between lymph node-positive and node-negative groups. Another study based on PNETs patients older than 75 years in SEER database obtained the similar coclusion. 31 However, different conclusion exits as well. In patients with PNETs who underwent surgery, positive nodal status represented poorer OS (HR: 1.41). 14
Surgery vastly improved prognosis of PNETs patients. In our study, surgery reduced the risk of deaths by over 60% both in younger and older PNETs patients. Previous study even reported that the 5-year survival reached 100% in localized small size PNETs after resected. 32 For advanced tumor, surgery was still recommended if greater than 90% of the tumor burden can be resected. 33 The landscape of treatment for advanced cancer is rapidly evolving, such as somatostatin analogs, 34 targeted therapies (everolimus), 35 peptide receptor radionuclide therapy. 36 However, novel therapies are not recorded in the SEER database, this is one limitation for our study.
Our study has some other limitations. The retrospective character of our study is indeed a limitation. No data on the clinical presentation or laboratory values in the SEER database which are applied to identify functional or nonfunctional tumors. PNETs in different countries may have different histologic types, and different ethnic backgrounds may have different environmental or genetic factors, and these results may not be applicable to countries other than the United States.
Conclusion
In a word, patients under 50 years old accounted for 23.8% of PNETs and had unique clinicopathological characteristics compared with older patients. In generally, younger patients with PNETs had a better overall survival rate, thanks to the fact that they received aggressive surgery and had well differentiated tumor. Patients with advanced tumor still had poor prognosis. Further exploration of advanced diagnosis and treatment approaches for PNETs is required.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.