
Abstract
Purpose
This study aimed to provide a clear comparable figure of the trends in incidence and mortality rates of esophageal cancer (EC) in Huai’an District, Huai’an City, Jiangsu Province, China, a high-risk area for EC.
Methods
The data for age- and sex-specific incidence rates between 1998 and 2016, the mortality rates in 1990-2016 and the number of EC patients were obtained from Huai’an District Cancer Registry. Crude rates, Age-standardized rates (ASRs) by world standard population and truncated age-standardized rates of EC incidence and mortality were calculated. The joinpoint regression analysis was used to calculate the annual percent changes (APC), average annual percent changes (AAPC), and their 95% confidence intervals (CIs).
Results
Overall, 20,892 new EC cases and 20,806 EC deaths were registered in Huai’an District. ASR of EC incidence from 1998 to 2016 and mortality from 1990 to 2016 were 73.32/100,000 and 60.03/100,000, respectively. The ASR illustrated that the incidence of EC had significant downward trends in total, male and female (AAPC = −4.65, −4.90, and −5.51, respectively, p <.01). The age-specific incidence and mortality rates of EC increased dramatically in people over the age of 40, and peaked in people between the ages 70-74. In the subdivisions of Huai’an District, geographical diversities in the crude incidence and mortality rates of EC were found.
Conclusion
In summary, the incidence and mortality rates of EC showed downward trends in Huai’an District. However, the burden of EC still remained serious in this high-risk area. Cost-effective methods of intervention and health education should be enhanced for improving EC prevention.
Introduction
The global cancer statistics 2020 estimated that esophageal cancer (EC) was the seventh most common type of cancer and the sixth leading cause of cancer deaths worldwide. 1 It is aggressive in nature and often diagnosed in late stages, leading to a low survival rate. The prevalence of EC is highest in Eastern Asia, followed by Southern and Eastern Africa. Approximately 80% of the cases worldwide occur in less developed regions. 1 Huai’an District, an inland low socio-economic rural area located in the Northern Jiangsu Province of China, is a high-risk area for EC and has been reported to have a distinct epidemiological pattern.2-8 Environmental and dietary factors play the most significant roles in the development of EC as the local residents are highly exposed to N-nitrosamines, mycotoxins, and other carcinogens from drinking water, pickled food, fried food, hot food, and stored grains.3,4,6,9-11 From 2008 to 2012, the crude incidence and mortality rates of EC in the Huai’an District were 96.15/100,000 and 63.25/100,000 respectively, ranked at the first position among all types of cancer, and esophageal squamous cell carcinoma (ESCC) has always been the predominant histological subtype. 3 Huai’an District is the highest risk area for EC in Huai’an City (when comparing to other districts), with an extremely high incidence of EC and the highest number of cases. Therefore, it was selected as a pilot rural area for the Early Diagnosis and Early Treatment Project of Esophageal Cancer (EDETPEC) supported by the government and Cancer Foundation of China since 2010, in order to improve the prevention of EC in high-risk areas.3,12
Over the past several decades, with socio-economic development, lifestyle changes, and the intervention of EDETPEC, declining age-adjusted incidence and mortality rates of EC were observed in the data provided by National Central Cancer Registry in China,13,14 particularly in some high-risk areas such as Linzhou and Cixian.15,16 However, although many EC studies have been conducted in Huai’an District, detailed EC statistics and the trend of incidence of the district have never been reported in previous studies.3,6,17-19 Therefore, this study aimed to provide a detailed report of EC statistics and a clear comparable figure of the trends in incidence and mortality rates of EC in Huai’an District, Huai’an City, Jiangsu Province, China between 1998-2016. This was based on the cancer registry report provided by Huai’an District Center for Disease Control and Prevention (CDC).
Materials and Methods
Source of Data
Huai’an District Division of Cancer Prevention and Control was established by Huai’an District CDC in 1987, and Huai’an District Cancer Registry was initiated in 1988, with a complete tumor registration and reporting system. The cancer registry has been included in Cancer Incidence in 5 Continents, and the computer administration system was introduced in 1998. However, the collected data was paper-based prior to 1998, and the incidence rate data from 1990 to 1997 was missing. Therefore, age- and sex-specific incidence rates between 1998-2016, mortality rates between 1990-2016 and the number of cases for EC patients were obtained from statistical office of Huai’an District Cancer Registry after verification of the data. The code for EC was C15 according to the International Classification of Diseases, 10th Revision (ICD-10). The demographic data was obtained from the Huai’an District Bureau of statistics of Huai’an City. Data used in this study does not contain personal information, thus ethical approval was not required. The participating registry has given their consent. The study was performed in accordance with the Declaration of Helsinki.
Quality Control
Quality of registration data was evaluated according to the criteria of “Guideline for Chinese Cancer Registration” 20 The mortality to incidence ratio (M/I), the proportion of morphological verification (MV%), and the percentage of cancer cases identified with death certification only (DCO%) were used to assess the completeness, validity, reliability and comparability of the data. 21 In Huai’an District, the overall indicators of M/I ratio, MV and DCO% were .69, 63.6, and .43%, respectively. Additionally, a full reconciliation with mortality data has been done for each year, thus the cancer cases died for other causes have been excluded.
Statistical Analysis
Crude incidence and mortality rates were provided. Age-standardized rates (ASRs) of EC were calculated and standardized using Segi’s World Standard population. Truncated age-standardized incidence and mortality rates (Segi’s World Standard population) between 35 and 64 years old were calculated, as the diagnosis data of these working-age populations typically have relatively higher completeness and reliability. To assess the trends in the epidemiology of EC, joinpoint regression was used to evaluate the annual percent changes (APC), average annual percent changes (AAPC), and their 95% confidence intervals (CIs). A minimum of zero joinpoints (1 line segment) and a maximum of 5 joinpoints (6 line segments) were allowed for each model. The program started with the minimum number of joinpoints and tested whether more joinpoints were statistically significant and must be added to the model (up to the maximum number). The number of new cases and deaths were evaluated using the 5 year age-specific incidence/mortality rates and the corresponding populations. Chi-square (χ2) test was performed to assess the differences in incidence and mortality rates among different regions in Huai’an District. Microsoft Excel 2016 (Microsoft Inc., Redmond, WA, USA), IBM SPSS Statistics version 23.0 (SPSS Inc., Chicago, IL, USA) and Joinpoint Regression Software version 4.6.0.0 (National Cancer Institute, Bethesda, MD, USA) were used in statistical analysis. Statistical significance was considered as p < .05 (two-tailed).
Results
Demographic Structure
Population structure by sex and year in Huai’an District during 1990-2016.

Population structure by age in Huai’an District during 1990-2016.


Population pyramid of Huai’an District in 1990-2016.
Incidence of Esophageal Cancer
Detailed information and trend in incidence of esophageal cancer by sex in Huai’an District during 1998-2016.
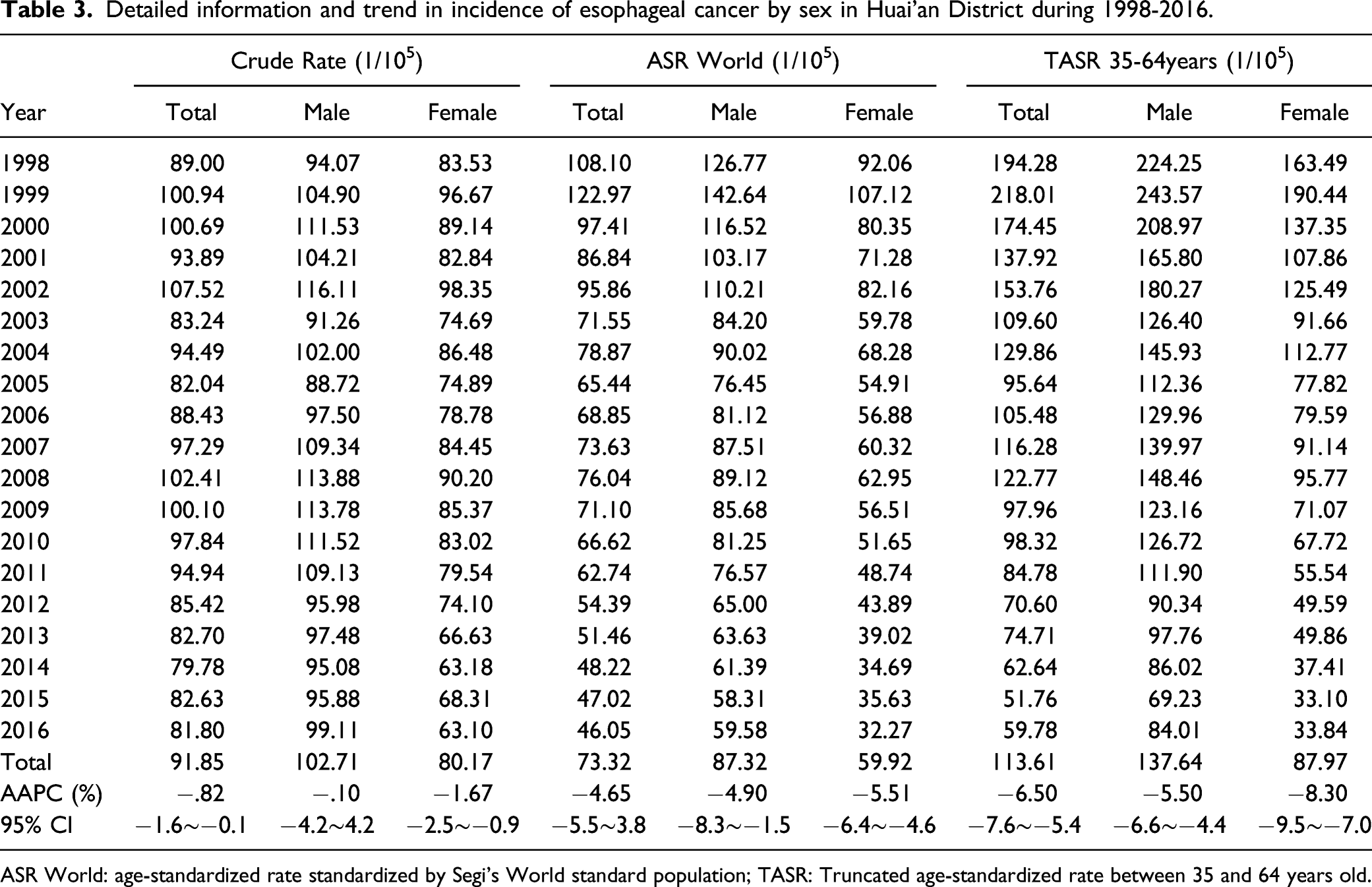
ASR World: age-standardized rate standardized by Segi’s World standard population; TASR: Truncated age-standardized rate between 35 and 64 years old.

The trend in incidence of esophageal cancer by sex in Huai’an District during 1998-2016. (A): Trend in crude incidence rate of esophageal cancer in total; (B): Trend in age-standardized incidence rate of esophageal cancer by world standard population in total; (C): Trend in crude incidence rate of esophageal cancer in males; (D): Trend in age-standardized incidence rate of esophageal cancer by world standard population in males; (E): Trend in crude incidence rate of esophageal cancer by in females; (F): Trend in age-standardized incidence rate of esophageal cancer by world standard population in females. *Indicates that the APC has statistical significance, p < .05.
Mortality of Esophageal Cancer
Detailed information and trend in mortality of esophageal cancer by sex in Huai’an District during 1990-2016.

ASR World: age-standardized rate standardized by Segi’s World standard population; TASR: Truncated age-standardized rate between 35 and 64 years old.
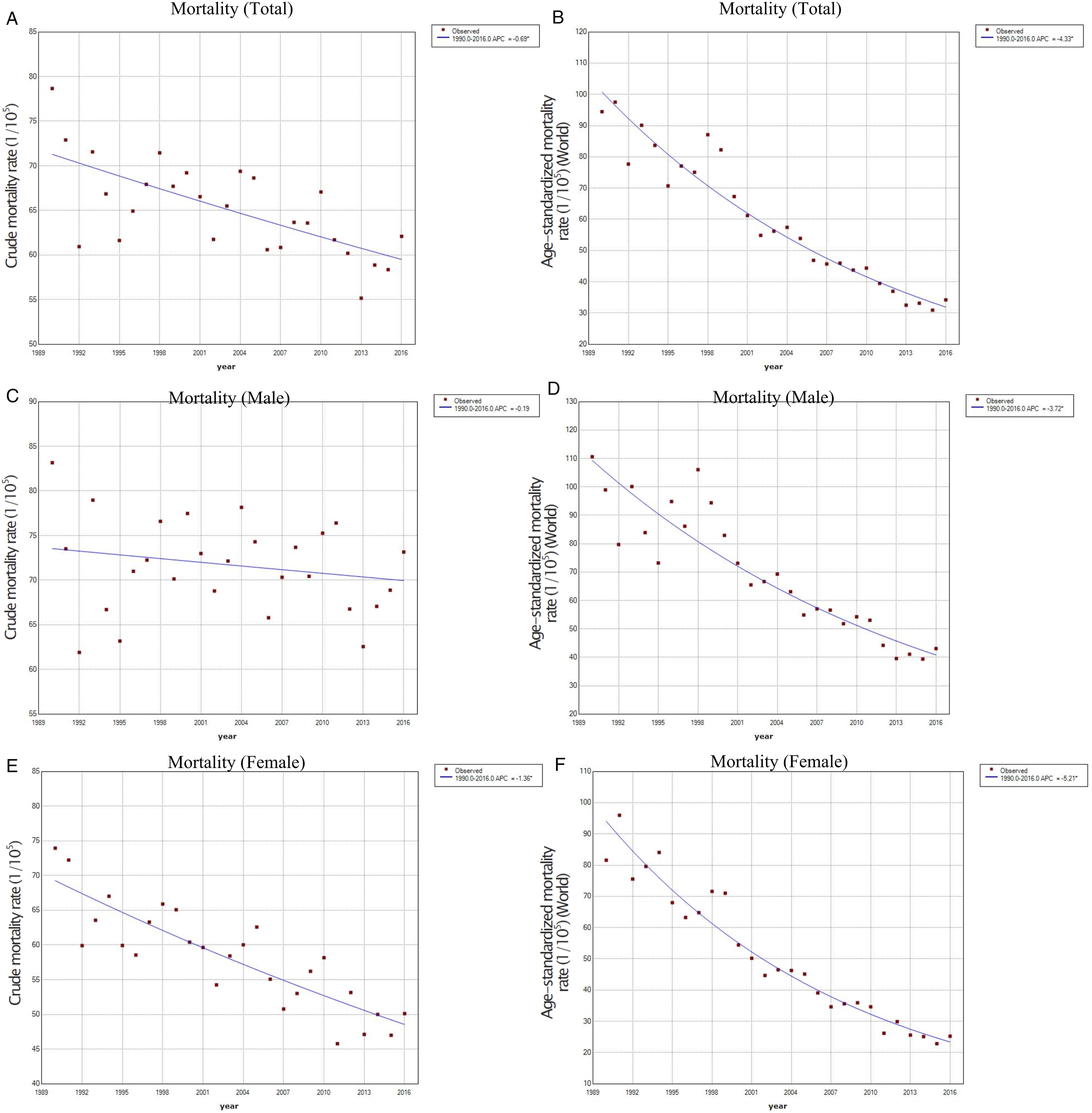
The trend in mortality of esophageal cancer by sex in Huai’an District during 1990-2016. (A): Trend in crude mortality rate of esophageal cancer in total; (B): Trend in age-standardized mortality rate of esophageal cancer by world standard population in total; (C): Trend in crude mortality rate of esophageal cancer in males; (D): Trend in age-standardized mortality rate of esophageal cancer by world standard population in males; (E): Trend in crude mortality rate of esophageal cancer by in females; (F): Trend in age-standardized mortality rate of esophageal cancer by world standard population in females. *Indicates that the APC has statistical significance, p < .05.
Age-specific Incidence and Mortality Rates of Esophageal Cancer
As shown in Figure 4, the age-specific incidence and mortality rates of EC were relatively low in both genders under 40 years of age, whereas the rates increase dramatically for those aged over 40. The peak appeared in the age group 70-74 years with the incidence of 775.16/100,000 in males, 560.52/100,000 in females. The mortality rates were 641.72/100,000 in males and 475.82/100,000 in females. The rates decreased dramatically for those aged 75 and over. Rates in males were generally higher than those in females. (A): Age-specific incidence of esophageal cancer in Huai’an District by sex, 1998-2016; (B): Age-specific mortality of esophageal cancer in Huai’an District by sex, 1990-2016.
Crude Incidence and Mortality Rates of Esophageal Cancer in Different Regions of Huai’an District
Crude incidence and mortality rates of esophageal cancer in different regions of Huai’an District during 2010-2016.
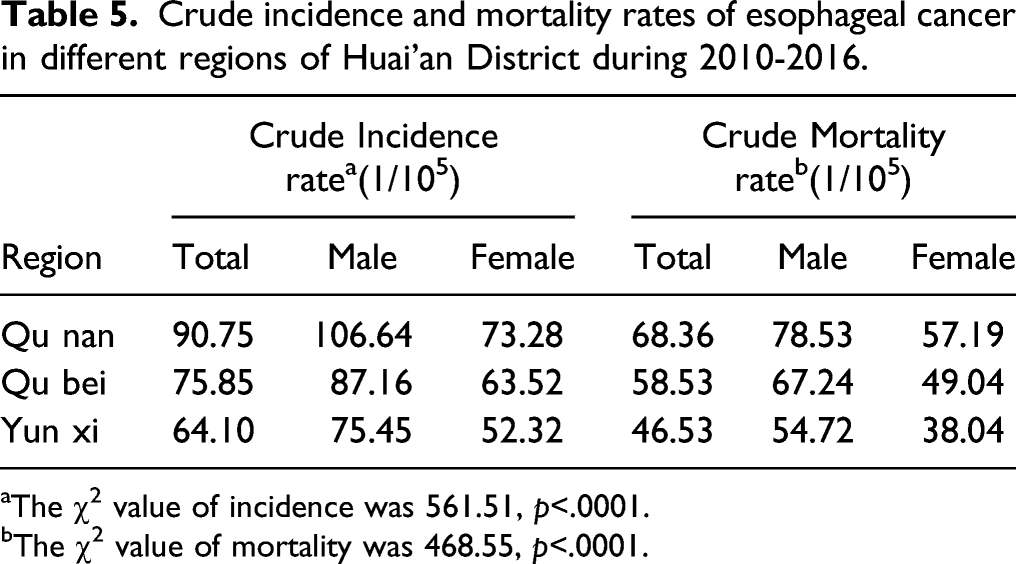
aThe χ2 value of incidence was 561.51, p<.0001.
bThe χ2 value of mortality was 468.55, p<.0001.
Discussion
In this study, we presented the 19 year trend in incidence and 27 year trend in mortality of EC in Huai’an District, a high-risk area for EC in the Northern Jiangsu Province of China. The overall quality indicators of M/I ratio was between .6 and .8, DCO% was less than 15%, which met the criterion, 20 whereas the MV% was lower than 66%. To some extent, MV% reflects the levels of medical diagnosis, medical technology development and economic development. Compared with developed countries, MV% of China cancer registration data can be relatively lower in the reports, especially in the early years. 22 As a whole, the ASRs of incidence and mortality of EC showed downward trends during the observed period of time. However, compared with the worldwide ASRs of EC incidence reported by Globocan 2020 report (9.3/100,000 in males and 3.6/100,000 in females) and the national ASRs of EC incidence reported by China 2015 report (16.75/100,000 in males and 5.94/100,000 in females), the ASRs of EC incidence in Huai’an District still remained fairly high.1,23 However, the crude rates of incidence and mortality in male group did not show statistical significance during the total observed period of time, but the potential reason is still unclear and requires further investigation. In addition, the result of the crude EC incidence for male group shows that only the period of 2008-2016 had significant downward trend, which may be partly explained by the implementation of EDETPEC during this period. Elderly populations are at a higher risk of developing EC, which may be associated with prolonged exposure to carcinogens. The incidence and mortality rates of EC dramatically increased for those aged 40 and older, and generally peaked in the 70-74 age group for both genders, suggesting that cancer screening should be focused on those aged over 40 years for both genders.
In Huai’an District, the incidence rate of EC was only 1.46-fold more common in men than in women. While EC is 2 to 8 times more common in men than in women in most other areas of the world, tobacco smoking and alcohol drinking are the dominant risk factors that cause this trend. 24 Our previous study reported a distinct epidemiological pattern of precancerous lesions of ESCC in Huai’an District, and the influencing factors for esophageal precancerous lesions may be similar to those previously identified as influencing factors for ESCC. 3 Like some other previous studies conducted in high-risk areas in China,25-29 the use of alcohol and tobacco may play a minor role in the development of EC, whereas environmental and dietary factors (which may influence both genders equally) were found to play dominant roles in the Huai’an District. 3 The reason is that in low-risk areas, people are not likely to be exposed to so many risk factors, thus the use of tobacco and alcohol may take the main responsibility for cancer development, resulting in a greater number of cases in men than in women. However, in high-risk areas, exposure to the chronic irritation of many carcinogens may make tobacco and alcohol seem to contribute little to EC incidence. 30 For example, 72.4% of ESCC cases were attributed to alcohol in the US while only 10.9% of cases were attributable in China.31,32 Previous studies conducted in Huai’an District indicated that factors influencing the risk of ESCC and its precancerous lesions included the source of drinking water, nutritional status, consumption of vegetables, fruits, corn, corn flour, pickled food, fried food, and hot food.3-6,8,9,18 For instance, consuming shallow well water and surface water was found to be associated with carcinogenesis of esophagus, 3 which was highly related to the contamination of nitrosamine and microcystin in the source of water in this region.9,33-35 Contamination of aflatoxin B1 and fumonisin B1 in food, especially in corn and corn flour, was also reported in this region.6,10,11 Additionally, many residents in Huai’an have been used to frequently consume pickled food (e.g., pickled radish, pickled root mustard, salted meat, and salted fish) and hot foods such as their staple food hot porridge made of corn flour, 3 while the N-nitrosamine precursors in pickled food may form highly toxic and carcinogenic N-nitrosamines, 4 and high temperature of 65°C and over may cause a carcinogenic effect because of the direct contact with esophageal mucosa, particularly the upper esophagus.36,37 Additionally, genetic factors such as genetic polymorphism, DNA methylation, and gene-nutrition interaction were also found to be significantly associated with the risk of EC.2,5,18
Similarly, with the city-town-village tertiary cancer prevention and treatment network established in Yangzhong County, 21 the local residents aged between 35-75 from 27 towns in Huai’an District were covered and eligible for a free routine endoscopy examination in EDETPEC, and the rate of compliance reached approximately 80% in total. Therefore, over the past several decades, with socio-economic development, lifestyle changes, the popularization of health education, and the intervention of EDETPEC, the living and nutritional conditions of the local residents have been greatly improved, and the esophageal precancerous lesions or EC can be detected at early stages. The incidence and mortality rates of EC thereafter have declined dramatically.
We found geographical diversities in the crude incidence and mortality rates of EC in the subdivisions of Huai’an District. These geographical patterns almost match those of stomach cancer, suggesting (at least some) common risk factors for these 2 cancers in Huai’an District. 38 These factors include the source of drinking water, high pickled food intake, and high fried food intake, which have been identified as important risk factors for both types of cancer in this area.3,39-41 In a report published in 1993, the highest crude mortality rate for EC was in Yun Xi (110.31/100,000), followed by Qu Nan (93.50/100,000) and Qu Bei (78.65/100,000). 42 In the present study, the highest rates for EC was in Qu Nan, followed by Qu Bei and Yun Xi. One reason for the change may be that the socio-economic development of Qu Nan was retarded compared to others, and the drinking water source may be contaminated by N-nitrosamines and algal toxins more heavily found in this region.9,33,34,43 Therefore, in 2020, Huai’an District Government planned to effectively govern the water source protection area of the Grand Canal Baimahu water plant for Qu Nan in the next 2 years. Currently, 22 freight yards and wharves have been renovated, 10 ferries have been banned, all gas stations, wharves, 224 houses, and 17 companies inside the first- and second-grade protection zones have been relocated or demolished.
This study has some strengths. The EC data of Huai’an District provided in this study are the most up-to-date and comprehensive since the Huai’an District Cancer Registry was initiated. Joinpoint regression was used to effectively disentangle the separate effects on secular trends. This study also has some limitations. First, the data of incidence rate from 1990 to 1997 were missing because the collected data were paper-based before 1998. Thus, to keep the completeness, validity, reliability, and comparability of the data, incidence rate in 1998-2016 and mortality rate in 1990-2016 for EC were analyzed after the verification of data. Second, the dramatic decrease in EC incidence after age 75 years old could be an indicator of incomplete registration among the elderly. Third, the results of the quality indicators including M/I ratio, MV%, DCO% were not constant over time, thus the overall indicators during the period of time were used. In addition, like previous analyses of cancer,21,44,45 this study analyzed the incidence and mortality of EC without distinguishing histological types. In the raw data, the information of morphological verification for some cases was not provided, the code of ICD-10 of many cases was C15.9 (malignant neoplasm of esophagus, unspecified), which means the location of neoplasm was unspecified, thus the accurate histological information for these cases were not likely to be provided. Internationally, divergent trends are usually observed between different histological subtypes of EC (squamous cell carcinoma vs adenocarcinoma) due to different risk factors and pathogenesis. 46 Esophageal adenocarcinoma (EAC) has become increasingly common in more highly developed world, and its carcinogenesis is initiated by the acid exposure of the esophageal mucosa from stomach, while ESCC has always been the predominant histological subtype of EC in developing countries, especially in the low socio-economic regions, and its carcinogenesis is associated with the chronic irritation of carcinogens. 46 The incidence of ESCC is decreasing in many countries, probably due to improved living conditions and nutritional status. 30 In China, ESCC accounts for more than 90% of EC cases, 47 and also is the predominant subtype of EC in Huai’an District. 3 Hence, to a great extent, the present study may reflect incidence trend of ESCC in the studied region. Further studies are needed to present a clear comparable figure of the incidence and mortality trends of EAC in the region in the future.
Conclusion
In conclusion, this study presented a 19 year trend in incidence and 27 year trend in mortality of EC in Huai’an District, a high-risk area for EC. The incidence and mortality rates of EC showed downward trends during the period of time. Elderly populations are at a higher risk of developing EC, and geographical diversities in the crude incidence and mortality rates of EC in the subdivisions of Huai’an District were found. The intervention of early diagnosis and treatment, the socio-economic development and the popularization of health education are important for improving prevention of EC.
Supplemental Material
sj-pdf-1-ccx-10.1177_10732748221076824 – Supplemental Material for Trends in Incidence and Mortality of Esophageal Cancer in Huai’an District, a High-Risk Area in Northern Jiangsu Province, China
Supplemental Material, sj-pdf-1-ccx-10.1177_10732748221076824 for Trends in Incidence and Mortality of Esophageal Cancer in Huai’an District, a High-Risk Area in Northern Jiangsu Province, China by Shaokang Wang, Da Pan, Zitong Chen, Guang Song, Renqiang Han, Guiju Sun, Ming Su, in Cancer Control
Footnotes
Acknowledgments
We thank all the participants, researchers and collaborators who were involved in the study for their efforts and contribution. Thanks also to Mr Rob Unwin for proofreading. This work was supported by the National Natural Science Foundation of China (No. 81673147) and the Danone Dietary Nutrition Research and Education Foundation (DIC2020-08).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China and Danone Dietary Nutrition Research and Education Foundation.
Authorship
Conceptualization: Shaokang Wang and Guiju Sun; Data curation: Ming Su, Guang Song and Renqiang Han; Formal analysis: Da Pan and Zitong Chen; Funding acquisition: Shaokang Wang; Investigation: Ming Su, Guang Song and Renqiang Han; Methodology: Da Pan and Zitong Chen; Project administration: Shaokang Wang and Ming Su; Resources: Shaokang Wang, Guiju Sun and Ming Su; Software: Da Pan and Zitong Chen; Supervision: Guiju Sun and Ming Su; Validation: Shaokang Wang and Da Pan; Visualization: Da Pan; Roles/Writing - original draft: Da Pan; Writing - review and editing: Da Pan and Shaokang Wang.
Data Availability Statement
All data generated or analyzed during this study are included.
Ethics Approval Statement
Data used in this study does not contain personal information, thus ethical approval was not required. The participating registry has given their consent. The study was performed in accordance with the Declaration of Helsinki.
Abbreviations
AAPC, average annual percent changes; APC, annual percent changes; ASR, age-standardized rate; CI, confidence interval; CDC, Center for Disease Control and Prevention; DCO%, the percentage of cancer cases identified with death certification only; EAC, esophageal adenocarcinoma; EC, esophageal cancer; ESCC, esophageal squamous cell carcinoma; EDETPEC, Early Diagnosis and Early Treatment Project of Esophageal Cancer; M/I, mortality to incidence ratio; MV%, the proportion of morphological verification
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.