
Abstract
Introduction
Quantifying disease burden plays a critical role in informing prevention strategies and optimizing health resource allocation. While existing studies have separately described the global epidemiological landscapes of chronic obstructive pulmonary disease (COPD) and tracheal, bronchus, and lung cancer (LC), there is a notable absence of comprehensive analysis on the combined burden of LC-COPD. Addressing this gap is essential for improving disease management and policy development.
Methods
Data on age-standardized incidence, death, prevalence, and disability-adjusted life year (DALY) rates (ASIR, ASDR, ASPR, and ASDALYR per 100 000) from 1990 to 2021, in global, regional, and national/territorial hierarchy, were retrieved from the 2021 Global Burden of Disease Study (GBD 2021). COPD to LC ratios of ASRs (C/L–ASRs) were calculated to describe the relative burden of LC-COPD. With Joinpoint regression, the average annual percentage changes were generated to study epidemiological trends. ASDALYR attributable to four shared risks, were systematically studied.
Results
In 2021, global ASRs for both COPD and LC declined, yet their combined disease burden remained substantial. Notably, five regions exhibited synchronous increases. Low SDI regions showed severe imbalance—described by a C/L–ASIR of 3.53 in 2021. Age stratification further revealed COPD-dominated mortality in aged ≥ 75 years, particularly among females. Despite a 60.1% global decline since 1990, smoking was still the leading contributor. Household air pollution from solid fuels posed a greater burden than smoking in South Asia and Sub-Saharan Africa. Ambient particulate matter pollution increased LC-related ASDALYRs in almost all regions.
Conclusion
Although the overall burden of LC-COPD is declining, the comorbid population remains large and continues to face healthcare access barriers. This study calls for shifting focus to the shared comorbidity burden, prioritizing the prevention of common risk factors, early identification of comorbidities, and implementing integrated care to optimize resource utilization under constrained conditions.
Plain Language Summary
Despite declines in the overall burden of chronic obstructive pulmonary disease (COPD) and tracheal, bronchus, and lung cancer (LC), the comorbid population remains substantial and persistently underserved. By shifting the lens from single diseases to their shared burden, our findings call for coordinated clinical and policy actions that prioritize prevention of shared risk factors, early identification of comorbidities, and integrated care to maximize benefits under constrained resources.
Keywords
Introduction
Tracheal, bronchus, and lung cancer (LC) is currently the most commonly diagnosed malignancy and the leading cause of cancer-related mortality worldwide.1,2 According to the International Agency for Research on Cancer (IARC), there are nearly 2.5 million new cases and more than 1.8 million deaths globally, accounting for 12.4% of all cancer diagnoses and 18.7% of cancer deaths. 3 Among all cancers, LC imposes the greatest economic burden, estimated at USD 3.9 trillion. 4
This burden substantially contributes to the global burden of disease and undermines population health. Curative-intent treatments for LC include surgical resection and radiotherapy, both of which require adequate baseline pulmonary function. 5 Moreover, treatment of LC is frequently accompanied by declines in pulmonary function. 6 Prior evidence indicates that decreases in pulmonary function are unavoidable regardless of treatment modality. 7
Chronic obstructive pulmonary disease (COPD) is the most common cause of chronic impairment of lung function and the third leading cause of death globally. 8 Its prevalence is projected to approach 600 million cases worldwide by 2050, which represents a relative growth of 23% in the number of individuals with COPD compared with 2020. The greatest growth will occur among females and in middle- and low-income countries and regions. 9
COPD not only appears to increase the risk of developing lung cancer, 10 but LC-COPD is also associated with poorer outcomes, including worse overall survival (OS) and progression-free survival (PFS) after treatment and a threefold increase in cardiopulmonary complications.11-13
Despite substantial research on each disease separately,14,15 prior studies have not comprehensively quantified the burden of LC-COPD, nor systematically examined temporal changes in their shared risk factors. To address this gap, we assessed the joint burden across global, regional, and national levels via Global Burden of Disease (GBD) 2021 estimates in 1990-2021.
We calculated age-standardized incidence, death, and prevalence rates (ASIR, ASDR, ASPR per 100 000) and quantified temporal trends via average annual percentage change (AAPC). We further constructed COPD to LC ratios of age-standardized rates (C/L–ASIR, C/L–ASDR and C/L–ASPR) and evaluated age-standardized disability-adjusted life years rates (ASDALYR) attributable to shared risk factors: smoking, ambient particulate matter pollution, household air pollution from solid fuels, and second-hand smoke. Analyses were stratified by socio-demographic index (SDI) quintile, sex, and age.
Methods
Data Sources and Software
This study collected and analyzed data from the GBD 2021 results, which were publicly available through the Global Health Data Exchange 2021 (GHDx 2021, https://vizhub.healthdata.org/gbd-results/, last accessed on December 30, 2024). 16 GBD 2021 estimated the burden of 288 causes, 371 diseases and injuries, and 88 risk factors in 204 countries and territories from 1990 to 2021. Data on the incidence, mortality, prevalence and DALYs due to COPD and LC from 1990 to 2021, categorized by sex, age, location, and risk factors, were obtained from GHDx 2021. Additional information on GBD 2021 is provided in Supplemental Note S1. Descriptive analyses and visualizations were performed using Graph-Pad Prism 10.1.0, MATLAB R2024a and Origin Pro 9.9.5.
Selection of Regions
In general, regions were classified according to their geographical location and sociodemographic characteristics. The world is divided into 21 major regions based primarily on geographic location and other demographic characteristics (details provided in Supplemental Note S1).
SDI Values
The socio-demographic characteristics of regions were reflected by SDI values, which serve as a comprehensive metric delineating the developmental spectrum of geographic locations. Ranging from 0 to 1, the SDI represents an amalgamation of rankings based on per capita income, average educational attainment, and fertility rates across all regions in the GBD study. In GBD 2021, locations are segmented into SDI quintiles: low (0 < SDI ≤ 0.570), low-middle (0.570 < SDI ≤ 0.670), middle (0.670 < SDI ≤ 0.812), high-middle (0.812 < SDI ≤ 0.858), and high (0.858 < SDI ≤ 1) categories. 17
COPD to LC Ratios of Age-Standardized Rates (C/L-ASRs)
We obtained the ASRs for LC and COPD. The ratio of ASR COPD to ASR LC was computed and then natural-log transformed to normalize the distribution of the ratio for subsequent analysis. This composite metric, denoted as C/L–ASRs, is calculated as

To assess the uncertainty of the estimates, we applied the Monte Carlo simulation method. For each estimate, we performed random sampling with replacement and simulated 1000 iterations. This allowed us to generate the distribution of the C/L–ASRs and compute the corresponding confidence intervals. The Monte Carlo method effectively captured the variability inherent in the data, offering a comprehensive uncertainty analysis.
In the uncertainty analysis, we considered data variability, model errors, and sampling errors. Data variability reflects differences in data quality across regions and time periods; model errors, introduced by the log transformation, were accounted for in the Monte Carlo simulations; and sampling errors were assessed through random sampling. However, systematic bias and uncertainties from model assumptions were not fully controlled, particularly regarding reporting and sampling biases in low-resource regions.
Joinpoint Regression Analysis
The Joinpoint regression model, also known as piecewise or multi-phase regression, divides a long-term trend line into several linear segments. It does not require a predefined trend in the data, making it particularly effective for analysing long-term disease data with multiple trends. The model’s strength lies in its ability to compute the Average Annual Percent Change (AAPC), a summary measure over a specified interval. When defining

Attributable Risk Factors
A comparative risk assessment framework was used to evaluate the disease burden attributable to 84 health risk factors categorized as behavioural, environmental/occupational, and metabolic risks. 17 Exposures, attributable DALYs of COPD and LC were estimated for four shared risk factors.
GATHER Checklist
The reporting of this study conforms to the GATHER guidelines. 18
Results
ASRs of Global and Regional COPD and LC Burdens
The Age–Standardized Burden Metrics (ASIR, ASDR, and ASPR), and Their Male/Female Ratios for COPD at Global Level, in SDI Quintiles and GBD Regions in 2021, and Their Changing Trends in 1990-2021

Abbreviations: COPD, chronic obstructive pulmonary disease; PC, percentages of change; M/F, male-to-female ratios; SDI, socio-demographic indexes; GBD, Global Burden of Disease; ASIR, age-standardized incidence rate; ASDR, age-standardized death rate; ASPR, age-standardized prevalence rate.
The Age–Standardized Burden Metrics (ASIR, ASDR, and ASPR), and Their Male/Female Ratios for LC at Global Level, in SDI Quintiles and GBD Regions in 2021, and Their Changing Trends in 1990-2021

Abbreviations: LC, tracheal, bronchus, and lung cancer; PC, percentages of change; M/F, male-to-female ratios; SDI, socio-demographic indexes; GBD, Global Burden of Disease; ASIR, age-standardized incidence rate; ASDR, age-standardized death rate; ASPR, age-standardized prevalence rate.
Five (24%) regions showed simultaneous increases in the ASIR of COPD and lung cancer—Andean Latin America (COPD 14.3%, LC 1.0%), Central Asia (COPD 0.3%, LC 60.2%), Central Latin America (COPD 12.1%, LC 69.8%), Central Sub-Saharan Africa (COPD 6.2%, LC 218.9%), and Western Sub-Saharan Africa (COPD 12.5%, LC 450.3%)—whereas eight (38%) regions exhibited concurrent declines (Figure 1A). ASDR decreased for both conditions in 13 (62%) regions, with Eastern Europe leading (COPD −67.2%, LC −40.6%) and Central Asia showing the largest LC decline (COPD −51.6%, LC −51.6%). In East Asia (COPD −68.0%, LC 12.1%), Western Sub-Saharan Africa (COPD −22.6%, LC 18.1%), and South Asia (COPD −11.3%, LC 11.3%), LC ASDR still increased by more than 10% (Figure 1B). For ASPR, only four (19%) regions showed simultaneous decreases: Central Asia (COPD −1.9%, LC −53.8%), Eastern Europe (COPD −11.4%, LC −31.9%), Southern Latin America (COPD −4.7%, LC −27.4%), and Tropical Latin America (COPD −0.8%, LC −3.8%) (Figure 1C). The ASRs (per 100 000 population) of COPD and LC incidence (A), death (B), and prevalence (C) in 2021 worldwide. The ASIPR of worldwide and across 21 GBD regions (D). Abbreviations: COPD = chronic obstructive pulmonary disease, LC = tracheal, bronchus, and lung cancer, GBD = Global Burden of Disease, ASIR = age-standardized incidence rate, ASDR = age-standardized death rate, ASPR = age-standardized prevalence rate, ASIPR = ASIRLC/ASPRCOPD
Between 1990 and 2021, most regions followed a three-phase pattern in ASIPR—a steady rise during the 1990s, a peak in the 2000s, and a slight plateau or moderate decline thereafter. Globally, ASIPR showed only a modest reduction. High-income regions consistently recorded the highest ratios (around 0.02), indicating a greater propensity for lung cancer comorbidity among individuals with COPD. East Asia and Australasia exhibited notable fluctuations and overall increases, suggesting a relative rise in lung cancer incidence within the COPD population since 1990. In High-income Asia Pacific, ASIPR rose mildly at first but later declined sharply and persistently. Most Sub-Saharan African subregions maintained low levels near 0.005, while Central Sub-Saharan Africa, Western Sub-Saharan Africa, and South Asia—though beginning from low baselines—showed steady increases. In contrast, Europe, Central Latin America, and Central Asia demonstrated overall declines during the same period (Figure 1D).
C/L–ASRs of COPD and LC Burdens Among Global and Regional
The Log-Transformed Ratio of COPD to LC Age-Standardized Rates (C/L–ASRs), and Their Changing Trends at Global Level, in SDI Quintiles and GBD Regions in 1990-2021

Abbreviations: COPD, chronic obstructive pulmonary disease; LC, tracheal, bronchus, and lung cancer; PC, percentages of change; SDI, socio-demographic indexes; GBD, Global Burden of Disease; ASIR, age-standardized incidence rate; ASDR, age-standardized death rate; ASPR, age-standardized prevalence rate; C/L–ASRs, ln(ASRCOPD) - ln(ASRLC).
C/L–ASRs of COPD and LC Burdens Among Countries and Territories
With the exception of Pacific Island countries (population of Cook Islands, Nauru, Niue, Palau, Tokelau and Tuvalu < 20 000), Nigeria, Nepal, Bhutan and Bangladesh in 2021 had C/L–ASIR of 4.45 [4.21, 4.70], 4.05 [3.79, 4.37], 3.90 [3.58, 4.31] and 3.81 [3.51, 4.17], respectively. They also ranked among the highest for C/L–ASDR, Nepal 3.21 [2.79, 3.62], India 2.85 [2.65, 3.08], Bhutan 2.76 [2.32, 3.29], Nigeria 2.51 [2.25, 2.80] and Malawi 2.43 [2.07, 2.81]. For C/L–ASPR, the leaders were Nigeria 7.21 [6.97, 7.49], Kenya 6.19 [5.94, 6.49], Bhutan 6.30 [5.95, 6.82], Malawi 6.47 [6.16, 6.83] and India 6.19 [6.01, 6.39] (Table S4).
The vast majority of nations that experienced significant increases in C/L–ASIR between 1990 and 2021 are located in the Northern Hemisphere, such as Kazakhstan (212.2%), Qatar (133.3%), Kuwait (133.3%), Tajikistan (132.7%) and Mexico (109.4%). Among 204 countries, 136 (66.7%) experienced ASIR increases: seven (3.4%) rose by 100-200%, 21 (10.3%) rose by 50-100%, 57 (27.9%) rose by 20-50% and 51 (25.0%) rose by 0-20%. Conversely, 62 (30.4%) showed decreases: 43 (21.1%) decreased by 0-20%, and 19 (9.3%) decreased by 20-50% (Table S5).
Mitigation trends show clear geography. Five largest reductions occurred in Lesotho (−46.4%), Egypt (−44.4%), China (−40.2%), Cabo Verde (−34.2%) and Kenya (−32.9%). Between 1990 and 2021, China experienced substantial declines in C/L–ASIR, with the decline of C/L–ASIR -40.2%, C/L–ASDR -71.8% and C/L–ASPR -47.3% (Table S5).
For C/L–ASDR, the top five increases were in Kazakhstan (178.7%), Norway (104.9%), the United States (103.4%), Saint Vincent and the Grenadines (93.7%) and Antigua and Barbuda (63.0%). Overall, 54 countries (26.5%) reported that the C/L–ASDR increased: three (1.5%) exceeded 100%, four (2.0%) rose by 50-100%, 25 (12.3%) rose by 20-50% and 22 (10.8%) rose by 0-20%. The remaining 150 (73.5%) declined (Table S5).
With respect to the C/L–ASPR, 108 countries (52.9%) recorded increases between 1990 and 2021: six (2.9%) rose by 100-200%, twelve (5.9%) rose by 50-100%, 48 (23.5%) rose by 20-50% and 42 (20.6%) rose by 0-20%. Declines occurred in 96 nations (47.1%). Kazakhstan (200.1%), Tajikistan (121.9%), Kyrgyzstan (120.0%), Kuwait (111.6%) and Uzbekistan (111.2%) experienced the largest ASPR increases (Table S5).
Trends of Global COPD and LC Burden Metrices
The current status and mitigation trends of the COPD and LC burdens in 204 GBD countries and territories exhibit significant inequalities. Figure 2 displays the results of AAPC derived from Joinpoint regression analysis of ASPR across 204 countries from 1990 to 2021. Presented through fitted curves and scatter density plots, it highlights the average temporal trends in ASPR of COPD and LC burden over 32 years and their associations with SDI levels. Globally, AAPC for LC demonstrates significant spatial variability, ranging from sharp declines to alarming increases. In contrast, the AAPC for COPD generally tends to remain more stable, with most values clustering near 0 (Figure 2A and B). Global burdens in 204 countries and territories. The AAPC of LC prevalence (A). The AAPC of COPD prevalence (B). The relationship between the AAPC in COPD and LC across different countries. The X-axis represents the AAPC value for COPD, while the Y-axis represents the AAPC value for LC. Each point represents a country, and the colour reflects the SDI (C). Abbreviations: COPD = chronic obstructive pulmonary disease, LC = tracheal, bronchus, and lung cancer, SDI = socio-demographic indexes, AAPC = average annual percentage change
This variability is exemplified by several key nations. Egypt exhibits among the highest AAPCs for both COPD and LC, representing a region where the burden of respiratory diseases is accelerating rapidly. Similarly, the Democratic People’s Republic of Korea also shows high AAPC for both conditions. Conversely, France presents a unique case with a relatively high AAPC for COPD yet an AAPC for LC that approaches 0, indicating a stabilization of its trend—a pattern often observed in high-income countries with mature tobacco control policies.Singapore is a standout performer, reporting one of the lowest AAPCs for LC, though future strategies should focus more on addressing its relatively higher burden of COPD. The range of extremes is further illustrated by countries leading in opposite directions. Morocco and Saudi Arabia are noted for having some of the highest AAPCs for LC. Kyrgyzstan and Kazakhstan report the lowest AAPCs for COPD, highlighting the success of respiratory health initiatives in parts of Central Asia (Figure 2C).
This global analysis underscores a divergent landscape: many high-income countries and territories are witnessing stabilizing or declining trends, particularly for LC, while numerous countries in low-income are experiencing a rising burden of both diseases (Table S6).
Distribution of COPD and LC Burdens by Sex and Age Group
Log-transformed C/L-ASR are presented to illustrate overall temporal patterns, whereas age- and sex-specific trends were depicted using the original, untransformed rates.
In the analysis of the C/L–ASIR, the ratio reached 1 in the 75-79 age group and exceeded 1 only after 80 years. Among adults aged ≥ 60 years, a higher ratio was more frequently observed in females. For men, the ratio increased sharply during midlife, peaking at 64% in the 35-39 age group, and remained positive until turning negative after age 80. For females, it rose modestly (29% at 35-39 years) and declined steadily from −11% in the 60-64 years age group to −39% in the ≥ 90 group. Regarding the C/L–ASDR, it exceeded those from COPD between 30 and 60 years of age, with a ratio maintained below 1. Beyond 65 years, COPD resulted in a ratio greater than 1. Females consistently exhibited higher ratios across all age groups. Both sexes demonstrated age-related declines in the ratio: moderate in males (ranging from −10% to −36%) and substantially steeper in females (from −30% to −54%). In the C/L–ASPR, the ratio exceeded 1 only after age 75, with nearly identical values between males and females. For males, the ratio rose to 49% at 40-44 years, plateaued, returned to 0% by 65-69 years, and became negative thereafter. For females, it hovered near 0 in early adulthood, increased slightly to 4% at 40-44 years, and decreased steadily to between −30% and −50% from age 55 onward (Figure 3). The C/L–ASRs in different sexes and age–groups. Incidence ratio (A), prevalence ratio (B), death ratio (C) and their percentages of change during 1990-2021 (D–F). Abbreviations: COPD = chronic obstructive pulmonary disease, LC = tracheal, bronchus, and lung cancer, SDI = socio-demographic indexes, C/L–ASRs = COPD/LC ratios of age-standardized burden metrics
Attributable Risks and Their Trends during 1990-2021
The profile of COPD and LC comorbidity burden attributable to four shared GBD risk factors, smoking, ambient particulate matter pollution, household air pollution from solid fuels, and second-hand smoke. Among the GBD super-regions, smoking was the predominant risk factor with the exception of South Asia and Sub-Saharan Africa. Compared to 1990, most regions exhibited a decline in ASDALYR attributable to smoking. In Central Europe, Eastern Europe, and Central Asia and the High-income super-regions, the ASDALYR for LC significantly exceeded that of COPD. Conversely, the ASDALYR for LC and COPD were comparable in Latin America and Caribbean, North Africa and Middle East, and Southeast Asia, East Asia, and Oceania. In contrast, South Asia and Sub-Saharan Africa saw a much higher burden of ASDALYR from COPD than from LC (Figure 4). The shared risk factors for COPD and LC burdens in seven GBD super regions. Changes in ASDALYR attributed to four risk factors between 1990 and 2021 in Central Europe, Eastern Europe, and Central Asia (A), Latin America and the Caribbean (B), Southeast Asia, East Asia, and Oceania (C), Sub-Saharan Africa (D), High–income regions (E), North Africa and the Middle East (F), and South Asia (G). Abbreviations: COPD = chronic obstructive pulmonary disease, LC = tracheal, bronchus, and lung cancer, GBD = Global Burden of Disease, SDI = socio-demographic indexes, ASDALYR = age-standardized disability-adjusted life years rates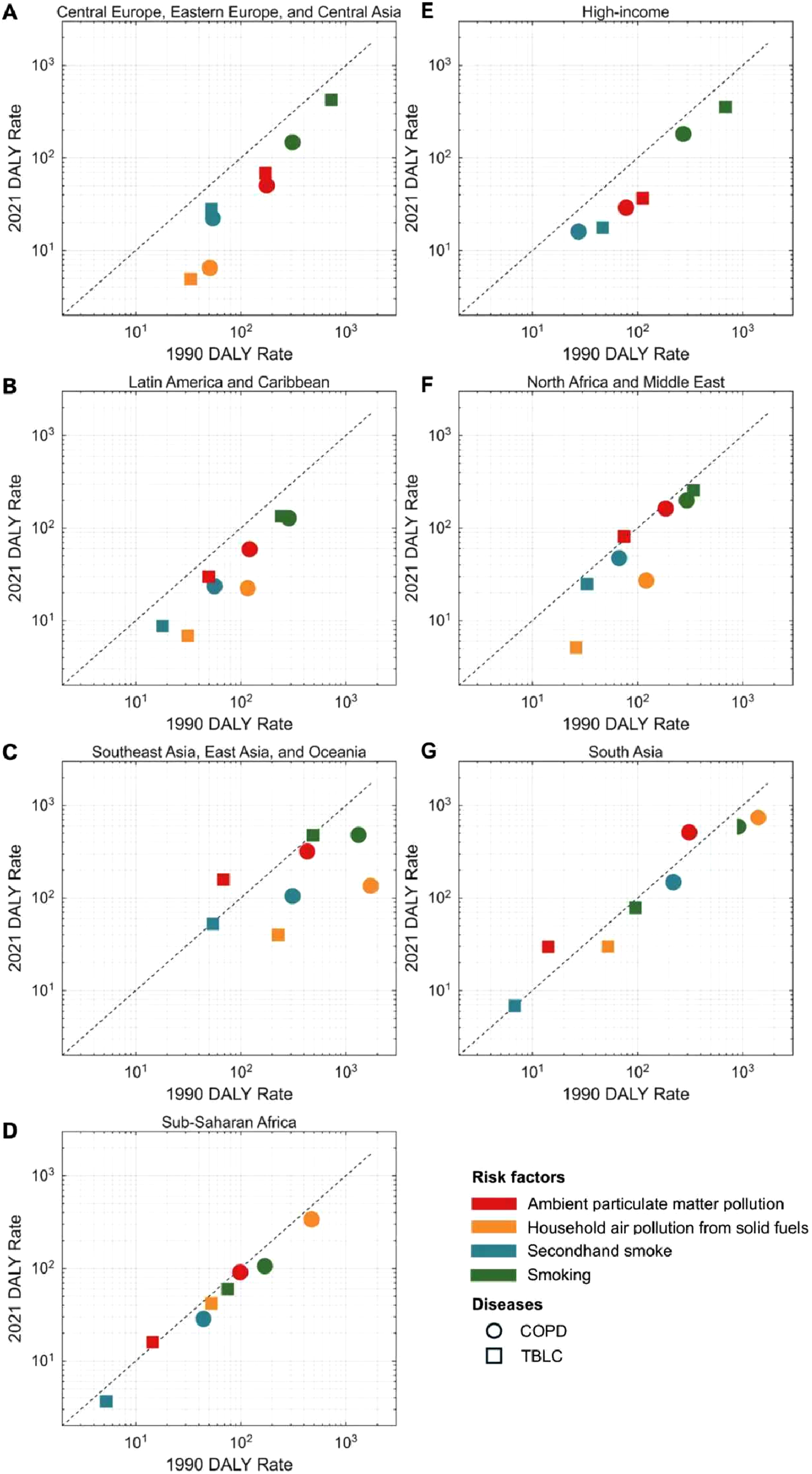
We can see the trends in ASDALYR for COPD and LC attributable to 4 shared risk factors, by SDI regions, from 1990 to 2021. In Global and all SDI regions, overall ASDALYRs for both LC and COPD showed a decline over this period. The most substantial reductions were observed for smoking, which decreased by up to 60.1%. For LC, ambient particulate matter pollution increased in all SDI regions except high-SDI regions. The other three risk factors demonstrated favorable declining trends. In the case of COPD, increases in ASDALYRs were confined to low-middle and low SDI regions (rising by 58.1% and 17.4%, respectively), while the other three risk factors exhibited declines to varying degrees across all SDI regions. When examining the ≥ 70 years age group, the total attributable ASDALYRs for LC showed a slight increase in high-middle and middle SDI regions, contrasting with the age-standardized population trend. Within this age group, ambient particulate matter pollution contributed to increased ASDALYRs of LC globally and in high-middle, middle, low-middle, and low SDI regions. Furthermore, second-hand smoke exposure was associated with increased ASDALYRs in high-middle and middle SDI regions, though it declined elsewhere. Among individuals aged ≥ 70 years, ambient particulate matter pollution was associated with elevated ASDALYRs for COPD globally and in middle, low-middle, and low SDI regions, although decreases were observed in other regions (Figure 5). ASDALYR changes (1990-2021) attributable to four shared risk factors (smoking, second–hand smoke, ambient particulate matter pollution, and household air pollution from solid fuels) for COPD and LC, at global level and in SDI quintiles. (A) LC age-standardized, (B) COPD age-standardized, (C) ≥ 70 years age-group in LC, (D) ≥ 70 years age-group in COPD. Abbreviations: COPD = chronic obstructive pulmonary disease, LC = tracheal, bronchus, and lung cancer, SDI = socio-demographic indexes, ASDALYR = age-standardized disability-adjusted life years rates
Discussion
In this study, we characterized the burden of LC-COPD across temporal, geographic, and demographic dimensions at the global, regional, and national levels and quantified the temporal dynamics of comorbidities via the C/L–ASRs. We also conducted region-, age-, and sex-stratified analyses of the four categories of shared risk factors. In routine clinical practice, the comorbidity of COPD and LC poses challenges that exceed the burden of either condition alone, this phenomenon has important implications for epidemiologic prevention and control and complicates many clinical scenarios.
To clarify the shifting link between COPD and lung cancer, we introduce ASIPR. It tells you how many new lung cancers appear each year per unit of COPD burden. When ASIPR rises, fresh lung cancer risk is climbing within the COPD pool because diagnosis is sharper, exposures are getting worse, or people with COPD are living longer. When ASIPR is low or falling, it may signal missed cancers in a high-risk group or that COPD is expanding faster than cancer. Regional patterns speak volumes. In High-income regions, ASIPR runs high: low-dose CT (LDCT) screening is common, populations are older, and a legacy of heavy smoking still lingers, which pushes more cancers to the surface among people with COPD. In Sub-Saharan Africa, low ASIPR likely reflects scarce diagnostics and health systems focused on infectious disease, its steady uptick is a warning that real cases are finally being found. In high-income Asia Pacific, ASIPR is drifting down, helped by tough tobacco control,such as smoke-free public spaces, steep taxes.
In terms of incidence, the persistently increasing C/L–ASIR across most regions, such as Western Europe, Southern Sub-Saharan Africa and Oceania, suggests a non-negligible proportion at elevated joint risk of both conditions. Compared with individuals without COPD, those with COPD have a two to seven-fold greater risk of developing lung cancer, independent of smoking history. 19 This warrants particular vigilance, as we observed increasing trends in LC in regions with high COPD burdens over the past two decades, such as Andean Latin America, Central Asia, Central Latin America, Central Sub-Saharan Africa and Western Sub-Saharan Africa.
Both conditions show parallel increasing trends in regions with high smoking prevalence, substantial high ambient PM2.5 exposure, and accelerating population ageing. Mechanistically, COPD and LC share a pathophysiological cascade: smoking and particulate matter trigger inflammation and excessive production of reactive oxygen and nitrogen species (ROS/RNS), leading to DNA damage and strand breaks due to impaired repair capacity. This ultimately fosters a pro–tumorigenic microenvironment through transforming growth factor-β (TGF-β)-mediated tissue remodelling.20-22
In recent years, the multimodal treatment paradigm for LC has improved outcomes in patients, however, LC-COPD complicates the deployment and on-treatment management of immunotherapy, targeted therapy, and radiotherapy.23-26 Although a systematic review indicated that patients with LC and COPD may derive greater benefit from immune checkpoint inhibitors (ICIs), the concomitant increase in immune-related adverse events (irAEs) increases treatment risk. 24 Similarly, radiotherapy demonstrates reduced efficacy and increased risk of radiation pneumonitis in this patient population. The benefits of targeted therapy can likewise be attenuated by underlying airway disease. For example, Wu et al. reported poorer survival in patients with LC-COPD receiving EGFR tyrosine kinase inhibitors (EGFR-TKIs). 27 Pulmonary function metrics are pivotal for assessing surgical candidacy and determining the maximal extent of resection, 28 compared with patients without COPD, those with LC-COPD have markedly worse clinical and perioperative outcomes, emphasizing the urgent need to improve LC screening and early therapeutic options in patients with COPD. Moreover, Lee et al demonstrated a clear association between forced expiratory volume in one second (FEV1) and postoperative survival. 29
In the C/L–ASIR, LC incidence remains higher than that of COPD up to the aged ≥ 80 years. This pattern reflects not only the widespread adoption of LDCT, which increases early lung cancer detection 30 but also the reliance on pulmonary function testing (PFT) for COPD ascertainment. 31 Spirometry is more labour intensive than CT is, limiting its utility as a screening tool and failing to promptly detect small airways disease. Consequently, patients with small airway pathology but without PFT abnormalities may derive less clinical benefit and remain underrecognized. 32 In 2011, the GOLD report acknowledged that grading severity by FEV1 alone is overly reductionist, as FEV1 correlates poorly with symptom burden, health–status impairment, and exacerbation risk. 33 Zhang et al. proposed a deep learning model that diagnoses COPD and other functional small airway diseases from a single inspiratory CT scan, enabling detection earlier than PFT. 34
The C/L–ASDR indicates that ASDR of LC predominates in the age group of 30-60 years (C/L–ASDR < 1), whereas COPD overtakes in the ≥ 65 years age group (C/L–ASDR > 1), reflecting that current COPD care is oriented toward symptom control and disease slowing, 35 in late stages, cardiovascular and other complications limit mortality reduction. 36 Targeted agents directed at pathways associated with lung cancer are under development to improve outcomes in patients with LC-COPD. 37 The C/L–ASPR exceeds 1 only in the ≥ 75 years age group, likely owing to the chronic, long-term nature of the disease, which increases in prevalence with age. Nonetheless, the rapidly growing comorbid population has not received commensurate attention in clinical management, COPD shapes patients’ needs and the uptake of palliative care. Among those with stage I–III disease, palliative care coverage remains low despite substantial symptom burden. 38
Controlling attributable risk factors is crucial for reducing disease mortality. In comorbid conditions, targeting shared risk factors can simultaneously alleviate the burden of both diseases. The screening identified four common exposures: ambient particulate matter pollution, smoking, household air pollution from solid fuels, and second-hand smoke. Accumulating evidence suggests that COPD exerts a substantial indirect influence on the associations between these exposures and lung cancer risk. COPD mediated 12.0% of the effect of smoking on lung cancer risk, 9.9% of the effect of annual consumption exceeding 20 packs, 3.8% of the effect of passive smoking, and 6.1% of the effect of biomass combustion. 39 These findings imply that smokers, heavier annual consumers, and biomass fuel users tend to develop COPD first, which subsequently increases their lung cancer susceptibility. In our attribution analysis stratified at 70 years, smoking dominated in nearly all regions.
The WHO Framework Convention on Tobacco Control (FCTC), adopted in 2005, is an international treaty that supports minimum standards for tobacco control (such as curbing advertising and taxing tobacco). By 2023, it had ratified by 183 parties. 40 Ambient particulate pollution impacts most regions worldwide to varying degrees, with middle income and less developed regions bearing a disproportionate burden. These regions, often driven by the practical demands of industrial growth, typically have limited investment in or technological capabilities for pollution control, exacerbating their pollution challenges. Nevertheless, all regions have now implemented proactive policies to enhance air quality monitoring and regulation. A 2024 air quality report indicated that over 90% of countries and territories failed to meet guideline levels, 80% of which were low- and middle-income countries (such as China and India), contributing to rising ambient particulate matter pollution–attributable burdens of COPD and LC. The environmental Kuznets curve provides a plausible explanation: air pollution peaks in the middle-income phase because of manufacturing-intensive growth. 41
China’s remarkable 40.2 % decline in C/L-ASIR stands out as a model of evidence-driven, policy-supported chronic respiratory disease control. Over the past decade, several long-term national programs have converged to build a comprehensive prevention and early detection framework. First, the Healthy China Action (2019-2030) 42 expanded spirometry screening and smoking-cessation services from large hospitals to community clinic. This led to a clear increase in early detection of COPD. 43 Second, the 14th Five-Year Cancer Control Plan (2021-2025) 44 promoted low-dose CT screening for high-risk groups. Over three million people have been screened, and pilot cities report much higher rates of early-stage lung cancer detection. 45 Third, the Blue Sky Defense War 46 launched in 2013 has cut national PM2.5 levels by nearly 60 %, improving air quality and reducing exposure to harmful pollutants.47,48
Beyond policy execution, China’s success has also been underpinned by domestic research on the effectiveness and cost-efficiency of screening approaches, which informed region-specific implementation guidelines and enabled resource-sensitive deployment. Emerging tools, such as artificial-intelligence-assisted imaging, real-time air-pollution monitoring, and integrated electronic health records, are poised to enhance the precision and scalability of these interventions. This multi-sectoral, evidence-anchored model illustrates that sustained coordination among clinical, environmental, and policy stakeholders is essential for lasting population-level gains, offering replicable lessons for other middle-income nations.
These findings indicate substantial potential to alleviate the global burden of COPD and LC through air quality improvements. This necessitates targeted policies that decouple economic growth from pollution intensity and accelerate transitions to cleaner energy sources. In Sub-Saharan Africa and South Asia, household air pollution from solid fuels contributes the largest share of DALYs over than smoking—with particularly pronounced impacts among females. This likely reflects widespread reliance on solid fuels (such as wood and coal), exposure to cooking fumes, and gendered roles in indoor food preparation. 49 Accordingly, improving access to clean household energy in these regions, especially for females, is critical to mitigating the growing burden of COPD and LC.
This study has several limitations. First, the availability and quality of primary data constrain estimates of COPD and LC burden and risk attribution. Disease registries were particularly imperfect 30 years ago, especially in low and middle-income countries. Moreover, several countries with small population included in the GBD lack empirical data, estimates for these settings rely on predictive covariates and spatial borrowing from neighbouring regions, which may further reduce accuracy. Second, LC is heterogeneous in terms of aetiology, pathology (encompassing subtypes such as squamous cell carcinoma and adenocarcinoma), and temporal trends. Similarly, COPD is a complex and heterogeneous disease with diverse mechanisms and clinical phenotypes. Owing to GBD constraints, we could not disaggregate analyses by histologic subtype, endotype, or phenotype. Third, although the composite linked C/L–ASRs are innovative, they do not directly measure individual-level comorbidities. Limitations inherent to the GBD data precluded the estimation of the proportion of patients with concurrent disease or the temporal ordering of disease onset. Furthermore, a related methodological limitation arises from the independent modelling of each risk–disease pair in the GBD framework. While a joint attribution method mitigates overlap when multiple risks act on a single disease, attributable burdens for COPD and LC are estimated separately for a shared risk factor like smoking. Consequently, the cumulative burden for the two diseases may reflect overlapping attribution. The GBD data do not provide parameters to allow for the redistribution of these shared risks across diseases, preventing correction for this potential overestimation. Future individual-level studies are therefore needed to provide complementary insights into both comorbid patterns and the precise burden attributable to shared risk factors.
Conclusion
Although the overall burden of LC-COPD is declining, the comorbid population remains substantial and persistently underserved. This study calls for a shift in focus to the shared comorbidity burden of these diseases, urging the prioritization of prevention for common risk factors, early identification of comorbidities, and the implementation of integrated care to maximize the benefits of available resources under constrained conditions.
Supplemental Material
Supplemental Material - Global and National Burden of Chronic Obstructive Pulmonary Disease and Tracheal, Bronchus, and Lung Cancer From 1990 to 2021: Comorbidity Burden Analysis Based on the Global Burden of Disease Study 2021
Supplemental Material for Global and National Burden of Chronic Obstructive Pulmonary Disease and Tracheal, Bronchus, and Lung Cancer From 1990 to 2021: Comorbidity Burden Analysis Based on the Global Burden of Disease Study 2021 by Hao Zhou, Zhiheng Dong, Xiaodan Ye in Cancer Control
Footnotes
Ethical Considerations
This study collected and re–analyzed the data from the GBD 2021 study, which was approved by the institutional review board of the University of Washington School of Medicine.
Consent to Participate
As a secondary analysis, no additional human participant research ethics review or informed consent was required for this study.
Authors’ contributions
H Zhou: Investigation, Methodology, Resources, Visualization, Writing–Original Draft, Z Dong: Formal Analysis, Investigation, Methodology, Software, Visualization, Writing–Original Draft, X Ye: Conceptualization, Funding Acquisition, Supervision, Writing–Review and Editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by National Science Foundation of China under grant numbers 82471977, 82271989, 82071990, 81571629, and Project of Shanghai Science and Technology Commission under the grant number 20Y11911900, 19411965200, 124119a0100. Shanghai STC innovation Project under the grant number 24F1904002.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.