
Abstract
Purpose
The purpose of this study was to assess the association of comorbidity burden with overall survival, accounting for racial/ethnic and socioeconomic differences in patients with cancer.
Methods
In this retrospective cohort study, patients newly diagnosed with cancer between 2010 and 2018 were identified from a large health plan in southern California. Cancer registry data were linked with electronic health records (EHR). Comorbidity burden was defined by the Elixhauser comorbidity index (ECI). Patients were followed through December 2019 to assess all-cause mortality. Association of comorbidity burden with all-cause mortality was evaluated using Cox proportional hazards model. Crude and adjusted hazard ratio (HR, 95%CI) were determined.
Results
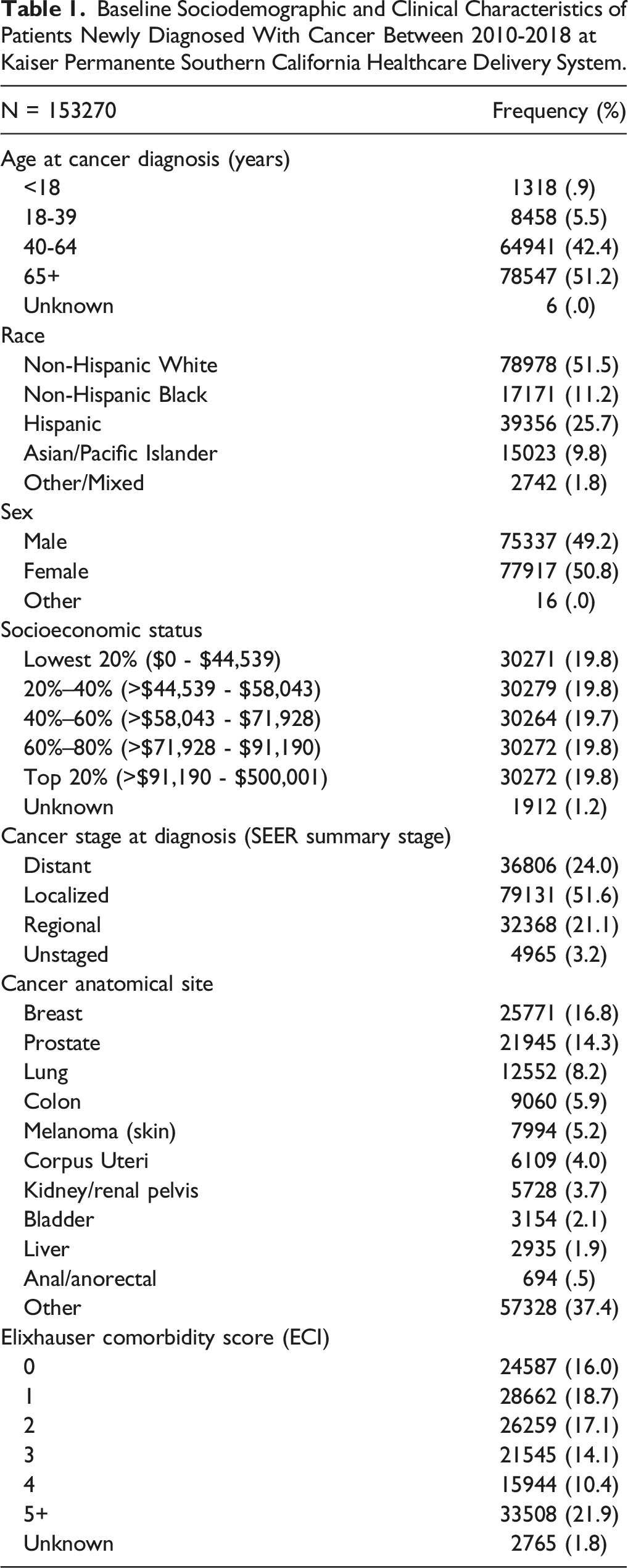
Of 153,270 patients included in the analysis, 29% died during the ensuing 10-year follow-up. Nearly 49% were patients of color, and 32% had an ECI > 4. After adjusting for age, sex, race/ethnicity, cancer stage, smoking status, insurance payor, medical center, year of cancer diagnosis, and cancer treatments, we observed a trend demonstrating higher mortality risk by decreasing socioeconomic status (SES) (P-trend<.05). Compared to patients in the highest SES quintile, patients in the lowest, second lowest, middle, and second highest quintiles had 25%, 21%, 18%, and 11% higher risk of mortality, respectively [(HR, 95%CI): 1.25 (1.21-1.29), 1.21 (1.18-1.25), 1.18 (1.15-1.22), and 1.11 (1.07-1.14), respectively]. When we additionally adjusted for ECI, the adjusted HRs for SES were slightly attenuated; however, the trend persisted. Patients with higher comorbidity burden had higher mortality risk compared to patients with ECI score = 0 in the adjusted model [(HR, 95%CI): 1.22 (1.17-1.28), 1.48 (1.42-1.55), 1.80 (1.72-1.89), 2.24 (2.14-2.34), and 3.39 (3.25-3.53) for ECI = 1, 2, 3, 4, and >5, respectively].
Conclusions
Comorbidity burden affects overall survival in cancer patients irrespective of racial/ethnic and SES differences. Reducing comorbidity burden can reduce some, but not all, of the mortality risk associated with lower SES.
Keywords
Introduction
Racial/ethnic and socioeconomic disparities in cancer outcomes are well documented. These disparities can partly be attributed to differences in access to care, systems of care, patient-level factors such as comorbidity burden, and social determinants of health. 1 People with suboptimal access to healthcare receive less preventive care, have less effective management of chronic diseases, less screening for early detection of malignancies, later presentations with a cancer diagnosis, and delays in cancer treatment initiation. However, disparities in cancer care are multifactorial and deep-rooted. Even when patients are cared for in a universal health care system and have similar access to care, lower socioeconomic status (SES) is a predictor of higher mortality risk. 2 Historically, racial/ethnic minorities have been associated with lower SES and worse cancer prognosis in the United States (US). 3 There are concerns that systemic racism and implicit racial bias affecting patient–provider interactions may result in poor health outcomes in people of color. 4 Implicit racial bias is a likely source of racial disparities in cancer patients as well. 5 However, race as a risk for health disparity, independent of SES, has also been reported, although this disparity seems to be mitigated in integrated healthcare systems. 6 While survival in cancer patients may be influenced by their treatments and care delivery, patients’ state of health may influence the cancer treatment they receive.
Lower SES is generally associated with a higher comorbidity burden. 7 However, little is known about the role of comorbidity burden in outcome disparities in cancer patients, independent of race/ethnicity and SES. Comorbidity burden affects patients’ ability to tolerate the best cancer treatments recommended for them, thereby affecting their cancer prognosis. 8 Cancer, as a group of illnesses, often require toxic treatments that need a high level of supportive care. The ability to deliver optimal cancer therapy in a timely fashion may be affected by comorbidities, as well as by factors associated with social determinants of health. Addressing these potential barriers to optimal care may lead to more equitable cancer treatment and outcomes.
The goal of this study was to evaluate the association of comorbidity burden with overall survival in patients with cancer, after accounting for race/ethnicity and SES differences, in an integrated healthcare delivery system in southern California. By including insured cancer patients within an integrated healthcare system, we were able to evaluate the association of comorbidity burden, race/ethnicity, and SES with overall survival without the confounding effects of variable insurance coverage and healthcare access.
Materials and Methods
Study Design, Subjects, and Setting
In this retrospective cohort study, 153,270 patients newly diagnosed with cancer between January 1st, 2010 and December 31st, 2018 at Kaiser Permanente Southern California (KPSC), a not-for-profit integrated healthcare delivery system, were included. Kaiser Permanente Southern California comprises of 15 community hospitals, over 220 medical offices, and serves more than 4.7 million racially/ethnically and socioeconomically diverse members. Patients diagnosed with cancer were identified from KPSC’s Surveillance Endpoints and End Results (SEER)-affiliated cancer registry. At KPSC, patients receive all medical care needs within the system. Data from the cancer registry were linked to KPSC’s electronic health records (EHR) that capture data on all care received by the health plan members, including diagnoses. Patients of all ages and all cancer anatomical sites were included. Patients with diagnosis of in-situ cancers were excluded. No other exclusion criteria were applied to enhance generalizability. Patients’ records were followed through December 31, 2019 (i.e., maximum of 10 years follow-up). The study was reviewed and approved by the Kaiser Permanente Southern California Internal Review Board (IRB #12339, Pasadena, CA, USA), which waived the requirement for written or verbal consent due to use of de-identified electronic health records which were collected as a part of routine care.
Outcome, Exposure, and Variables of Interest
The main outcome of interest was overall (all-cause) mortality. Patients’ records were followed from cancer diagnosis (baseline) through December 31, 2019, for vital status using a combination of death databases from KPSC, California state, and the National Death Index; thus, we had no loss to follow-up. Primary exposure of interest was comorbidity burden, defined using the Elixhauser comorbidity index (ECI). 9 ECI was based on comorbidities/conditions 1 year prior to cancer diagnosis. ECI was included as a categorical variable and had the following categories: 0 (no comorbidities), 1, 2, 3, 4, 5+, and unknown. Patients who did not have comorbidity data available 1 year prior to cancer diagnosis were included in the ‘unknown’ ECI category (<2% of sample). Covariates of interest included race/ethnicity, neighborhood SES, insurance payor (e.g., Medicare, Medicaid, employer, self), sex, smoking status, age at cancer diagnosis, stage at cancer diagnosis (SEER summary stage), year of cancer diagnosis, cancer treatments, and KPSC medical center. Race/ethnicity was coded according to the North American Association of Central Cancer Registries algorithm into the following categories: African American/Black; Asian/Pacific Islander; Hispanic; Native American; Other/Mixed; and non-Hispanic White. Neighborhood SES was categorized into quintiles based on geocoded aggregated neighborhood income at the census-block level.
Statistical Analysis
Descriptive statistics were reported using frequencies and percentages by race/ethnicity, geocoded neighborhood income (SES), and ECI. Crude and adjusted association of exposure and covariates of interest with the outcome (overall mortality) were reported using Cox proportional hazards model. Proportional hazards assumptions were validated by Schoenfeld residuals. Patients were followed from their cancer diagnosis (between 2010 and 2018) until death or end of study follow-up period (December 31, 2019), whichever occurred first. Hazard ratio and 95% confidence intervals (HR, 95%CI) were reported. The multivariable Cox proportional hazards models were adjusted for variables selected a priori based on epidemiological and clinical relevance. Observations with missing data were included in the analysis in the “Unknown” category; frequencies (percentages) and HR (95%CI) were reported accordingly. All analyses were performed in SAS 9.4 (Cary, NC), and GraphPad Prism 9 was used to make plots/figures.
Results
Baseline Sociodemographic and Clinical Characteristics of Patients Newly Diagnosed With Cancer Between 2010-2018 at Kaiser Permanente Southern California Healthcare Delivery System.
All patients were followed until date of death or end of study (December 31, 2019) (maximum follow-up was 10 years). Crude and adjusted association of comorbidity burden with overall mortality is shown in Figure 1. In the crude model, a trend in increased mortality risk by higher ECI score was observed (P-trend < .10). Patients with ECI = 4 and 5+ had nearly a 3-fold (HR = 3.98, 3.81-4.16) and 7-fold (HR = 7.33, 7.05-7.63) increased risk of mortality compared to patients with ECI = 0. A statistically significant association between comorbidity burden and mortality persisted in the multivariable model, after adjusting for neighborhood SES, race/ethnicity, age, sex, cancer stage, smoking history, insurance payor, medical center, year of cancer diagnosis, and cancer treatments. Compared to ECI = 0, having ECI = 1 and 2 increased the mortality risk by 22% and 48%, respectively (HR = 1.22, 1.17-1.28 and HR = 1.48, 1.42-1.55, respectively). Patients with ECI = 3, 4, and 5+ had 80%, 124%, and 239% increased risk of mortality than patients ECI = 0, respectively (HR = 1.80, 1.72-1.89; HR = 2.24, 2.14-2.34; and HR = 3.39, 3.25-3.53). The Kaplan–Meier curves for overall survival by ECI categories are shown in Figure 2. Forest plot showing crude and adjusted association of comorbidity burden with overall mortality in patients newly diagnosed with cancer. Kaplan–Meier curves comparing overall survival by Elixhauser Comorbidity Index categories in patients newly diagnosed with cancer.

Association of Race/Ethnicity and Socioeconomic Status With Mortality in Patients Newly Diagnosed With Cancer.

*Model 1: Adjusted for age, sex, race/ethnicity, cancer stage, smoking status, insurance payor, socioeconomic status (SES), medical center, year of cancer diagnosis, and cancer treatments. **Model 2: Adjusted for all variables in Model 1 and Elixhauser Comorbidity Index (ECI).
Regarding neighborhood SES, we observed a trend of higher mortality risk by decreasing SES quintiles in Model 1 (P-trend < .05). Compared to patients in the highest SES quintile, patients in the lowest, second lowest, middle, and second highest quintiles had 25%, 21%, 18%, and 11% higher risk of mortality, respectively [(HR, 95%CI): 1.25 (1.21-1.29), 1.21 (1.18-1.25), 1.18 (1.15-1.22), and 1.11 (1.07-1.14), respectively]. In Model 2 which incorporated ECI, this trend persisted even though the adjusted HRs were slightly attenuated (P-trend < .05).
Discussion
This study provides insight on the impact of comorbidity burden on overall survival in patients diagnosed with cancer in an integrated healthcare system. A trend demonstrating greater mortality risk by increasing comorbidity burden, measured by the ECI, was observed. The association of comorbidity burden with higher overall mortality was independent of racial/ethnic, neighborhood SES, health insurance payor, and access to care differences. Findings from this study highlight the existing comorbidity burden in patients with cancer and the need for incorporating comorbidity management in personalized cancer care.
Previous studies have reported on the negative prognostic impact of comorbidities on overall survival in patients with cancer.8-13 Increased overall mortality risk with increasing number of comorbidities were demonstrated before.10,11,13 Our findings are consistent; we observed a statistically significant trend in mortality risk by increasing ECI. Comorbidities, in general, are known predictors of mortality; in patients with cancer, the issue is more complicated as patients with high comorbidity burden are less likely to receive and complete the recommended cancer therapies.8,12 Presence of comorbidities may influence the treating physicians’ judgment in how aggressive they may be with delivering cancer treatment, thereby affecting overall prognosis. 10 While we did adjust for cancer treatment categories in our adjusted model, we did not have information on adherence to or completion of cancer treatment. However, based on our adjusted model, we can cautiously report that comorbidity burden is an independent predictor of overall mortality in patients with cancer. Though it is beyond the scope of our current study, it would be interesting to see how comorbidity burden affects cancer-specific survival.
Historically, race/ethnicity is an important predictor of overall prognosis in cancer patients. People of color are known to have lower survival following cancer diagnosis than non-Hispanic white cancer patients.3,14 On the other hand, lower SES, non-White race/ethnicity, and comorbidity burden are also inter-related. 15 There is much discussion about the influence of race on medical care and the effect of systemic racism. 4 Systemic racism in medical care can be related to access to care, systems of care, implicit bias and social determinants of health.4,5 However, majority of the previous studies did not account for racial/ethnic and SES differences in reporting the association of comorbidity burden with survival in patients with cancer. They did not address issues of health insurance or access to care either. Because our study was based in an integrated health care delivery system, and included insured cancer patients, we were able to reduce or eliminate the confounding effects of variable access to care and differences in systems of care. In the adjusted model, we observed lower overall mortality risk in Black and Hispanic patients compared to non-Hispanic white patients. Although this finding is contradictory to previous studies,3,14 it underscores the potential role that integrated healthcare system have in reducing racial/ethnic disparities in cancer outcomes.
Association of lower SES with poor health is well documented.16,17 Patients with cancer are no exception; we observed economically disadvantaged patients to have worse overall survival. This finding is important as it highlights disparities unexplained by access to care, insurance, cared delivery system, age, sex, race/ethnicity, cancer stage, and comorbidity burden. In our study we were able to adjust for age, stage, race/ethnicity and still observed disparity related to SES. When we further adjusted for comorbidity burden, the disparity related to SES was present but slightly attenuated. This suggests that increased comorbidity burden explains some of disparity related to SES. Future studies on other social determinants of health are needed to reduce SES disparities in patients with cancer.
Our study had some limitations. Since we did not assess cause-specific mortality, we were unable to differentiate between comorbidity-related and cancer-related mortality. We did not assess overall mortality risk by type of comorbidity present; it would be interesting to see if overall mortality risk varies by type or cluster of comorbidities. It would also be helpful to have data on severity of comorbidities and to assess the association by cancer type. We did not have data on diet or physical activity; thus, it is likely that some residual confounding exists. Further, patients in this study were all insured; the association between greater comorbidity burden and worse survival might be even stronger in uninsured populations. However, to our knowledge, this is the first study evaluating association of comorbidity burden with overall mortality in patients with cancer independent of differences in race/ethnicity, SES, insurance payor, and access to care. We had a large racially/ethnically diverse population of cancer patients of all ages. Because our study was based in an integrated healthcare delivery system, we had comprehensive EHR data that captured the full burden of comorbidities in our study population. Findings from our study highlight the overwhelming burden of comorbidities in patients with cancer and its role on overall mortality.
Conclusion
Comorbidity burden affects overall survival in patients with cancer irrespective of racial/ethnic and SES differences. Many of these comorbidities are modifiable; future research should focus on treatment strategies effective in reducing comorbidity burden in cancer patients, thereby reducing outcome disparities in this high-risk population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Institutes of Health/NHLBI (R01HL154319 (RH)), and Kaiser Permanente Southern California, a not-for-profit integrated healthcare system.