
Abstract
Background
Pancreatic cancer places a substantial global health and economic burden. However, the epidemiological characteristics and chronological trends of pancreatic cancer in high-income Asia-Pacific have not been systematically analyzed.
Methods
Data obtained from the GBD 2021 database were used for this cross-country secondary analysis. We used Joinpoint regression to analyze the temporal trends of pancreatic cancer disease burden in the high-income Asia-Pacific. Age-period-cohort model was used to estimate and describe the impact of age, period, and cohort effects on health outcomes. Bayesian age-period-cohort model was used for the projection of pancreatic cancer incidence from 2022 to 2036.
Results
In high-income Asia-Pacific, the age-standardized prevalence rate (ASPR), mortality rate (ASMR), and disability-adjusted life-years (DALYs) rate (ASDR) were estimated to be 11.2 (95% UI, 9.69-12.17), 9.56 (95% UI, 8.34-10.34), and 197.6 (95% UI, 178.87-210.6) per 100 000 population, respectively, in 2021, which were all higher than those in across Asia. From 1990 to 2002, the age-standardized incidence rates (ASIRs) trend was rather stable. Instead, the ASIRs trend went up gradually from 2002 to 2011 in both males (APC = + 1.03, 95% CI: 0.85, 1.20) and females (APC = + 1.64, 95% CI: 1.40, 1.89). ASIRs and ASMRs went up considerably with increasing age, especially over 60. The ASIRs in the high-income Asia-Pacific region are predicted to go down in the years ahead, from approximately 12.81 in 2021 to approximately 11.11 in 2036 for males, and from approximately 8.97 in 2021 to approximately 8.42 in 2036 for females.
Conclusion
A comprehensive upward trend in ASIRs, ASPRs, ASMRs, and ASDRs of pancreatic cancer was observed in the high-income Asia-Pacific between 1990 and 2021. Given the poor prognosis of pancreatic cancer, prevention strategies are paramount, especially for modifiable factors like smoking, alcohol drinking, and obesity.
Plain Language Summary
The primary objective of this study was to contribute to assessment of pancreatic cancer disease burden in the high-income Asia-Pacific nations (Japan, Singapore, Republic of Korea and Brunei Darussalam). Hopefully, the study results can be utilized to optimize the deployment of healthcare resources and reduce the unnecessary burden of pancreatic cancer.
Introduction
Pancreatic cancer is a lethal condition of the digestive system and has a poor prognosis. 1 The incidence and mortality rates of pancreatic cancer have been increasing in the past decades. 2 Pancreatic cancer places a substantial global health and economic burden worldwide, especially on developed and higher HDI countries.3,4 GLOBOCAN 2022 revealed that there were about 511 000 diagnoses and 467 000 deaths from pancreatic cancer globally in 2022, with global incidence ranking twelfth and global mortality ranking sixth among all cancers. The disease is among those with the most dismal prognoses, accounting for nearly 5% of all cancer deaths worldwide. 5 A study covering 43 countries including Japan and South Korea, demonstrated that by 2030, the incidence of pancreatic cancer in all the 43 countries is projected to increase steadily. 6 Owing to the lack of typical early symptoms as a red flag, pancreatic cancer is mostly diagnosed at an advanced stage and is not eligible for radical surgery, which leads to frustrating outcomes. 7 Despite of the combination of chemotherapy or chemoradiotherapy, the 5-year survival from pancreatic cancer remains as low as 9%. 8 The increasing incidence and mortality of pancreatic cancer and its poor survival figures stress the need for further research on pancreatic cancer.
The significant annual economic cost of cancer has posed a tremendous public health challenge in the Asia-Pacific region. 9 When it comes to cancer epidemiological research in Asia-Pacific, previous studies have mainly focused on liver cancer, gastric cancer, and so on.10-12 However, the latest epidemiological characteristics of pancreatic cancer in the Asia-Pacific have not been adequately researched, and the studies on high-income Asia-Pacific are currently lacking. 13 Therefore, an increasing number of studies on pancreatic cancer in the high-income Asia-Pacific are expected to be performed. For now, no study has comprehensively analyzed the GBD 2021 data on pancreatic cancer, and emphasizing pancreatic cancer in high-income Asia-Pacific is necessary.
The primary objective of this study was to contribute to detailed assessment of pancreatic cancer disease burden in the high-income Asia-Pacific nations (Japan, Singapore, Republic of Korea and Brunei Darussalam). Hopefully, the study results can be utilized by various countries to improve the deployment of healthcare resources and reduce the unnecessary burden of pancreatic cancer.
Methods
Data Source
The GBD is an international collaborative, publicly available source of the most updated epidemiological data. Data from 1990 to 2021, obtained from the GBD 2021 study, which is available online,14,15 were used for this cross-country secondary analysis. DisMod-MR 2.1, a Bayesian disease modelling meta-regression tool, was primarily applied to estimates in the GBD database. DisMod-MR 2.1 model is able to generate internally consistent incidence, prevalence and mortality estimates by age, sex, and year. 16 We extracted and reported the incidence, prevalence, mortality, and DALYs numbers and rates stratified by sex and age groups, as well as their respective 95% uncertainty intervals for pancreatic cancer in Asia and high-income Asia-Pacific. DALYs is a measure of disease burden that takes into account the premature death, diseases, and injuries to evaluate the total years of healthful loss. 17 Since the data were derived from the publicly accessible GBD database, no ethical approval or informed consent was necessary.
Statistical Analyses
This study used Joinpoint software (version 4.9.1.0) to perform the Joinpoint analysis. 18 We conducted the age-period-cohort analysis on the R-based web tool developed by the US National Cancer Institute. 19 The Bayesian age-period-cohort analysis was performed in R (version 4.4.1) software using the BAPC and INLA packages. 20
Joinpoint Analysis
Temporal trends of the pancreatic cancer disease burden in high-income Asia-Pacific were assessed using Joinpoint regression analysis. Joinpoint regression model builds a multi-phase regression based on the time distribution characteristics of the disease and conducts trend fitting and optimization according to the data points in every line segment. Joinpoint software calculates APC and AAPC with their respective 95% CI for each segment. APC assesses the trend of each interval of segmented functions, while AAPC evaluates the average trend across the entire study interval. When the 95% CI of the AAPC estimate was greater than 0, it denoted a rising trend. And if less than 0, it suggested a descending trend; if equal to 0, a steady trend. 18
Age-Period-Cohort Analysis
The age-period-cohort model was used to estimate and describe the impact of age, period, and cohort on health outcomes. 21 Based on Poisson distribution, the age-period-cohort model is capable of informing cancer incidence and mortality. Age effects (longitudinal age curves) refer to the risk of health outcomes correlated with age. Period effects (period rate ratios) refer to the influence of changes over time on outcomes among all age brackets. Cohort effects (cohort rate ratios) are portrayed as changes in the incidence or mortality across groups of people with the same birth years. If the estimate for age, period, and cohort effects is greater than 0, it indicates a risk factor; if less than 0, a protective factor. This study incorporated pancreatic cancer data extracted from the GBD 2021 database for the past three decades. Age and period were divided into 5-year consecutive intervals, from <5 to 95+, and from 1992-1996 to 2017-2021, for further evaluation.19,22
Bayesian Age-Period-Cohort Analysis
Since the Bayesian age-period-cohort (BAPC) model shows higher accuracy and better coverage, we used BAPC model integrated nested Laplace approximations for the projection of pancreatic cancer incidence from 2022 to 2036 in the high-income Asia-Pacific.20,23 The population estimates for high-income Asia-Pacific regions were taken from the official Internet website. 24
Results
Descriptive Analysis
Prevalence, Deaths, and DALYs for Pancreatic Cancer in Asia and High-Income Asia-Pacific in 1990 and 2021 (Generated From Data Available at https://vizhub.healthdata.org/gbd-results).

Abbreviations: 95% UI, 95% uncertainty intervals; ASRs, age-standardized rates.
Figure 1 displays the prevalence, incidence, and deaths numbers of pancreatic cancer cases in different age groups in 2021. Figure 2 illustrates the age-standardized incidence, prevalence, and mortality rates of pancreatic cancer in Asia and high-income Asia-Pacific in 2021 by age. Before 90-94 years, the incidence rates in both Asia and high-income Asia-Pacific exhibit a consecutive upward trend with age, especially after the 60-64 year range, when the incidence rates increase more dramatically. Similar trends were observed in the prevalence rates among both sexes in Asia and among females in high-income Asia-Pacific. When it comes to mortality rates, steadily rising trends with age were observed in both Asia and high-income Asia-Pacific among females. For males, there shows a decreasing after 90-94 years. Overall, in terms of age-standardized rates in most age groups in both regions, male suffered more. In Asia, the incidence rates and mortality rates are higher for males than females before 90-94 years, and the prevalence rates are higher for males than females before 85-89 years. Similarly in high-income Asia-Pacific, the incidence rates and prevalence rates are higher for males than females before 85-89 years, and the mortality rates are higher for males than females before 90-94 years. The distribution of absolute DALYs and age-standardized DALYs rates due to pancreatic cancer by age group, sex, and nation/region in 2021 is depicted in Figure 3. Since data of some certain countries were not included in the GBD database, they are not displayed in the figure. Although pancreatic cancer incidence was highest in the elderly, there were geographical differences as to which age group carried the largest pancreatic cancer related burden. In Japan, the greatest burden was concentrated in people aged 70-74, while the 60-64 age group population placed the heaviest burden in Korea. Age-specific Pancreatic Cancer Case Numbers in High-Income Asia-Pacific and Asia in 2021. (A) High-Income Asia-Pacific, (B) Asia, (C) Brunei Darussalam, (D) Japan, (E) Republic of Korea, (F) Singapore. Age-Standardized Incidence, Prevalence, and Mortality Rates of Pancreatic Cancer in Asia and High-Income Asia-Pacific in 2021 by Age, (A) Incidence Rates in Asia, (B) Prevalence Rates in Asia, (C) Mortality Rates in Asia, (D) Incidence Rates in High-Income Asia-Pacific, (E) Prevalence Rates in High-Income Asia-Pacific, (F) Mortality Rates in High-Income Asia-Pacific. Distribution of Absolute DALYs and Age-Standardized DALYs Rates due to Pancreatic Cancer by Age Group, Sex, and Nation/Region in 2021, (A) DALYs Counts, (B) Age-Standardized DALYs Rates.


Trends in the numbers and age-standardized incidence, prevalence, mortality, and DALYs rates of pancreatic cancer in Asia and high-income Asia-Pacific from 1990 to 2021 are illustrated in Figures 4 and 5. An upward trend was observed in the age-standardized incidence, prevalence, and mortality rates in both regions, with males constantly outnumbering females. In Asia, the increase of incidence, prevalence, and mortality rates in males was more significant than that in females, whereas in high-income Asia-Pacific, a contrary feature was observed. From 1990 to 2021, the DALYs counts for males and females in both regions increased continuously and considerably. However, there was a marginal growth in age-standardized DALYs rates for females in both regions, and a moderate downward trend for males in the high-income Asia-Pacific. Trends of Numbers and Age-Standardized Incidence, Prevalence, Mortality, and DALYs Rates of Pancreatic Cancer in Asia, (A) Incidence, (B) Prevalence, (C) Mortality, (D) DALYs. Trends of Numbers and Age-Standardized Incidence, Prevalence, Mortality, and DALYs Rates of Pancreatic Cancer in High-Income Asia-Pacific, (A) Incidence, (B) Prevalence, (C) Mortality, (D) DALYs.

Joinpoint Analysis
The results of the Joinpoint regression analyses of the age-standardized incidence, prevalence, and mortality rates of pancreatic cancer in the high-income Asia-Pacific from 1990 to 2021 are depicted in Figure 6. From 1990 to 2002, the ASIRs trend was rather stable. While the ASIRs trend went up gradually from 2002 to 2011 in both males (APC = + 1.03, 95% CI: 0.85, 1.20) and females (APC = + 1.64, 95% CI: 1.40, 1.89). Since 2011, the trend of incidence rates has begun to fluctuate slightly. A similar chronological trend was observed for ASPRs. In terms of ASMRs, there was an upward trend from 2002 to 2012, marginal in males (APC = + 0.58, 95% CI: 0.44, 0.73) and moderate in females [APC = + 1.89 (2006-2011), 95% CI: 1.02, 2.76]. Table 2 lists the AAPC results for different locations. The AAPC for Singapore (0.10, 95% CI: −0.11,0.31) and for Brunei (0.06, 95% CI: −0.17,0.28) suggested that the general trend of pancreatic cancer mortality in Singapore and Brunei remained steady. Joinpoint regression results of the age-standardized incidence, prevalence, and mortality rates in Japan, Singapore, the Republic of Korea, Brunei Darussalam and Asia are shown in Supplemental Figures 1-5. Joinpoint Regression Analysis of the Sex-specific Age-Standardized Incidence, Prevalence, and Mortality Rates for Pancreatic Cancer in High-Income Asia-Pacific From 1990 to 2021. (A) Age-Standardized Incidence Rates. (B) Age-Standardized Prevalence Rates. (C) Age-Standardized Mortality Rates. AAPC Results for Prevalence, Mortality, and DALYs Rates in Asia and High-Income Asia-Pacific From 1990 to 2021. Abbreviation: 95% CI, 95% confidence intervals.

Age, Period and Cohort Effects on Incidence and Mortality
The longitudinal age curves, period, and cohort RR of pancreatic cancer incidence and mortality in the high-income Asia-Pacific are shown in Figure 7 and Supplemental Figure 6. After controlling for period and cohort factors, ASIRs and ASMRs went up considerably with increasing age, especially over 60. After controlling for age and cohort factors, the RR of ASIRs experienced a decline then increase, and then decline. A downward trend of RR was seen in ASIRs and ASMRs in both sexes from 1994 to 2004. In males, the RR of ASMRs decreased from 2004 to 2019, whereas in females, the RR increased during the same period. After controlling for age and period factors, the RR of ASMRs exhibited a slight upward tendency from birth year 1927 to birth year 1967, followed by a mild downward trend from birth year 1972 to birth year 2017. Longitudinal Age Curves, Period and Cohort RR of Pancreatic Cancer Incidence in High-Income Asia-Pacific for Both Genders (A, D, G), Males (B, E, H) and Females (C, F, I).
Trends of Age-Standardized Incidence Rates Projected by BAPC
We performed BAPC to forecast the temporal trends of age-standardized pancreatic cancer incidence rates by gender, and the results of high-income Asia-Pacific are depicted in Figure 8. Overall, the age-standardized incidence rates in the high-income Asia-Pacific region are predicted to go down in the years ahead, from approximately 12.81 in 2021 to approximately 11.11 in 2036 for males and from approximately 8.97 in 2021 to approximately 8.42 in 2036 for females. While in Singapore, the Republic of Korea and Brunei, the ASIRs are predicted to grow. Japan will be the only country in the region where the incidence rate of pancreatic cancer is predicted to decrease among males. Projections of Pancreatic Cancer Incidence Trends in High-Income Asia-Pacific, (A) High-Income Asia-Pacific, (B) Japan, (C) Singapore, (D) Republic of Korea, (E) Brunei Darussalam.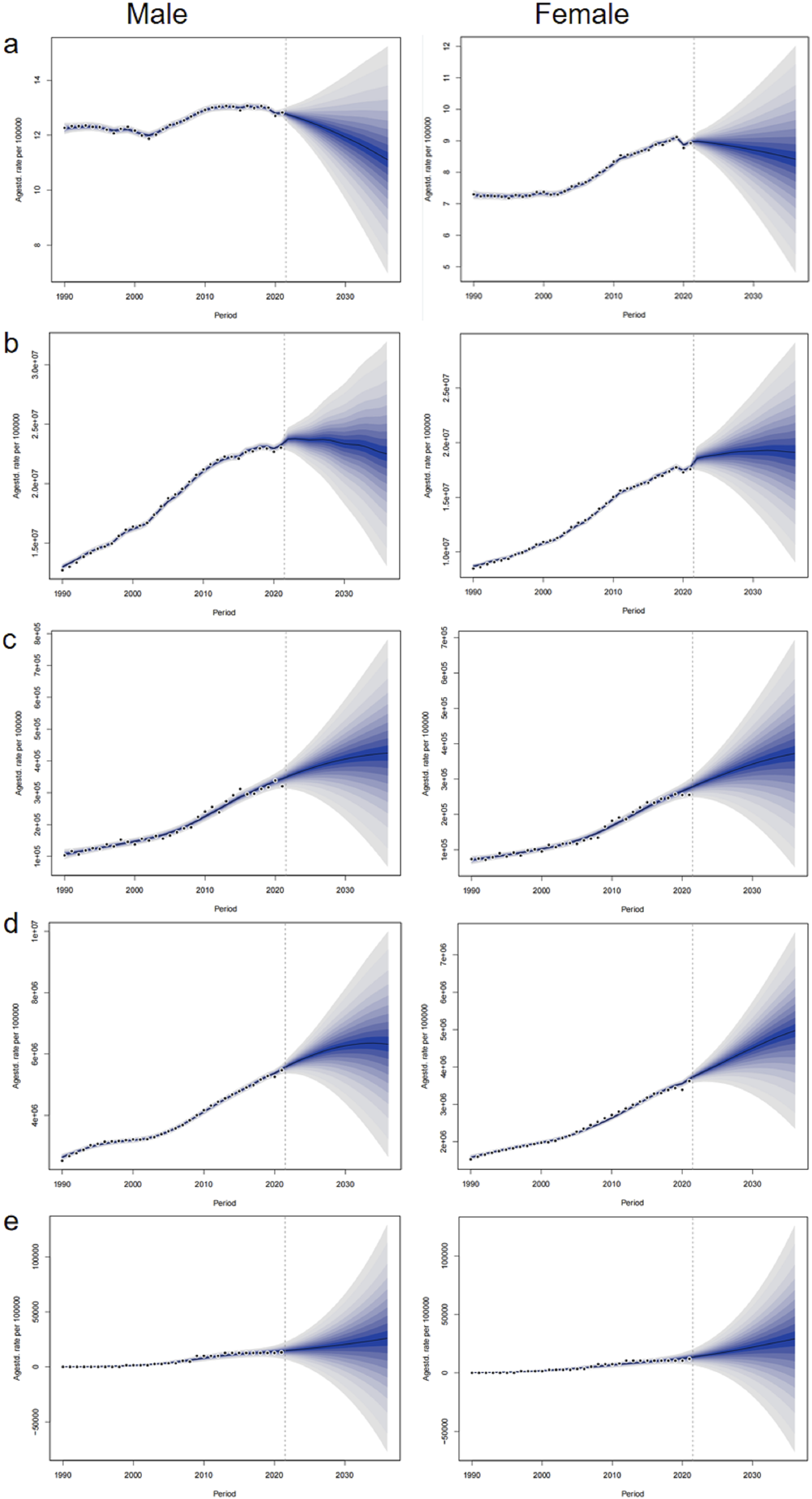
Discussion
GBD 2021 study, which involved 204 countries and territories from 1990 to 2021, conducted a rigorous evaluation of the loss of human health attributable to 371 diseases and injuries. 14 The GBD 2021 added updated and post-COVID-19 data to the database, thus supersedes GBD 2019 database, now is the most comprehensive disease burden research effort by far. 15 GBD 2021 study provided the most comprehensive epidemiological information of pancreatic cancer from 1990 to 2021. 14 In this study, for the first time we used the latest data extracted from GBD 2021 to analyze the epidemiological characteristics and variation tendencies of pancreatic cancer burden in high-income Asia-Pacific over the past three decades. Also, we made predictions for the next 15 years. It’s indicated that the probabilistic forecasts derived from the BAPC model were accurately calibrated and did not exhibit excessive width. 25 Future research could consider incorporating more appropriate and accurate models to further validate and expand our findings.
Overall, there demonstrated an increase in ASIRs, ASPRs, ASMRs, and ASDRs of pancreatic cancer in high-income Asia-Pacific between 1990 and 2021, and were all higher than those across Asia in 2021. These results are in keeping with the conclusions reached in previous studies that the pancreatic cancer burden is greater in economically developed nations.26,27 This is mainly because obesity, diabetes, smoking, and alcohol consumption are relatively more prevalent in high-income nations, which are all risk factors for pancreatic cancer.28-30 However, in the Asia-Pacific region, the obesity problem is significantly more severe in lower- and middle-income countries. 31 A dose-response meta-analysis indicated that high alcohol intake, particularly liquor, was correlated with the increased risk of pancreatic cancer. 32 Smoking is positively associated with increased pancreatic cancer risk, and quitting smoking before 65 may reduce this risk. 33 It’s particularly noteworthy that Brunei demonstrated the lowest incidence and prevalence among the four countries in the region, and no significant difference was observed between males and females compared to the other three countries. A very much possible reason is the prohibition of alcohol drinking due to religion. 34 Japanese males are the only population in the region predicted to have a decrease in pancreatic cancer incidence. This is possibly associated with the reduction in obesity prevalence. From 2020 to 2021, the obesity prevalence in Japan decreased from 4.5% to 4.0% for males, and from 2.4% to 2.0% for females, with the decrease for males being 0.1% more than that for females. 35 The enforcement of the revised Health Promotion Act and Tokyo Metropolitan Ordinance in April 2020, which aim to prevent second-hand smoke, may also contribute to the decline in pancreatic cancer incidence. 36 Pembrolizumab has got approval in Japan since 2018, and nal-irinotecan and olaparib have been approved in Japan since 2020. 37 Whether the predicted decrease of pancreatic cancer incidence in Japan is correlated with the newly approved medicines still calls for further research. We have noticed that the upward trend of female ASIRs is evident both from 1990 to 2021 and in the prediction for the next 15 years. The research on the actual changing trends of the risk factors of pancreatic cancer in high-income Asia-Pacific is currently deficient, which means it will be a new research orientation. According to a literature review, metformin for diabetics may reduce the risk of pancreatic cancer, while insulin therapy may increase the risk. 38 Because of its poor prognosis, the prevention strategy for pancreatic cancer is of paramount significance, particularly for modifiable factors like smoking, alcohol drinking, and obesity.
In the vast majority of time during observation period, males carried a heavier pancreatic cancer burden than females. This is possibly because there are more drinkers and smokers in men than in women.32,39 Smoking increases the pancreatic cancer risk by 75%, making it the strongest environmental risk factor. 40 However, in some age groups in our study, especially over 90-94, the age-standardized rates of pancreatic cancer were higher in females than in males. Females are estimated to have greater pancreatic cancer burdens than males, pretty likely because females tend to have a longer lifetime rather than higher incidence, prevalence, and mortality rates. 41
From the Joinpoint analysis results, it’s noteworthy that ASIRs showed an upward trend from 2002 to 2011. We speculate it is correlated with diagnostic improvements. In Japan, the National Health Insurance started to cover the expense of 18F-fluorodeoxyglucose positron emission tomography in 2002. The coverage was extended to include the diagnosis of metastasis and recurrence in 2006. 42 The increase of ASMRs did not start to decelerate or undergo a transition until 2012, which can be potentially attributed to the introduction of FOLFIRINOX and gemcitabine + albumin-bound paclitaxel regimens, which have been proven to show satisfactory outcomes for pancreatic cancer patients. 43
The age effect results suggest that the incidence rates of pancreatic cancer increase with the growth of age, with the most significant growth occurring over 60. The high-income Asia-Pacific is severely aging, with South Korea and Japan being aging countries. Elderly people in South Korea are expected to account for 20% of the population by 2025, and 25.5% by 2030. 44 In 2020, the proportion of the elderly population in Japan was 29%, and this percentage is expected to reach 38.4% by 2065. 45 The denser population of the elderly also possibly account for the greater pancreatic cancer burden in the high-income Asia-Pacific than in the whole Asia. A study shows that 50% of pancreatic cancers are diagnosed after the age of 70 years. The increased number of driver gene mutations and the greater cumulative effect of tobacco exposure in the elderly also account for the growth in incidence with advancing age. 46 Pancreatic cancer development is a process featured by a stepwise accumulation of genetic mutations. 47 Approximately 10% of the cases of pancreatic cancer are attributed to genetic alterations. 48 Tobacco use is not only a leading cause of pancreatic cancer globally, but also associated with 14% of pancreatic ductal adenocarcinoma deaths. 49
Since the mid-1970s, the survival rates for most common cancer types have shown improvement, while pancreatic cancer remains an exception. As the fourth leading cause of cancer-related mortality, pancreatic cancer has an overall 5-year relative survival rate of only 9%. 8 Pancreatic ductal adenocarcinoma accounts for over 90% of all cases of pancreatic cancer, and is often diagnosed at an advanced stage due to the deficiency of typical symptoms and effective screening approaches. The early diagnosis is paramount for this devastating disease. The application of radiomics models based on CT in the early diagnosis of pancreatic cancer could become an important direction for future research. 50
Notably, the screening, diagnosis, and treatment of cancer have been postponed in many countries owing to disruptions caused by the COVID-19 pandemic. 51 It was demonstrated in previous study that cancer diagnosis rates in America were lower than expected in 2020 and 2021. 52 Although no significant variation was observed in period RR around 2019, no conclusion can be reached that COVID-19 is irrelevant to pancreatic cancer incidence. Conversely, it calls for further and deeper research on the association between COVID and pancreatic cancer incidence. The statistical models in the current study do not account for potential covariates, such as socioeconomic status, healthcare access, and lifestyle factors, which might influence pancreatic cancer trends. Future studies could consider including these potential covariates for further research.
This analysis has several limitations, which are applicable to all studies using the GBD database. Firstly, the accuracy and completeness of estimates depend largely on the quality of data reporting systems and collection methods of different countries. Like the deficiency of DALYs number in 5-year age intervals in Brunei and Singapore in this analysis. The data discrepancies might introduce systematic biases during comprehensive analyses, and have the potential to influence the overall estimation of regional disease burden. Moreover, data heterogeneity may trigger selection bias, especially in regions with limited data coverage. This issue may potentially lead to either an underestimation or an overestimation of disease burdens. Also, confounding factors resulting from differences in data collection and medical practice between countries may have led to bias in the study results. The use of multiple complex models raises the possibility of overfitting, particularly in the projection analyses like BAPC analysis.
Conclusion
An overall increase in ASIRs, ASPRs, ASMRs, and ASDRs of pancreatic cancer was observed in the high-income Asia-Pacific between 1990 and 2021. Most of the time, males carried a heavier pancreatic cancer burden than females. Japanese males are the only population in the region predicted to have a decrease in pancreatic cancer incidence. Given the poor prognosis of pancreatic cancer, prevention strategy is of paramount significance, particularly for the modifiable factors like smoking, alcohol drinking, and obesity.
Supplemental Material
Supplemental Material - Pancreatic Cancer in High-Income Asia-Pacific: A Population-Based Study
Supplemental Material for Pancreatic Cancer in High-Income Asia-Pacific: A Population-Based Study by Donghong Wang and Zhibin Ma in Cancer Control
Footnotes
Acknowledgments
The authors sincerely thank all open-access resources.
Statements and Declarations
Author Contributions
ZM and DW conceived the study. DW analyzed the data, prepared Figures and Tables, and drafted the manuscript. ZM reviewed and revised the manuscript. All authors made contributions to the article and approved the submitted version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available in GBD 2021 database.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.