
Abstract
Background
Chronic lymphocytic leukemia (CLL) poses a growing challenge to public health. Tracking temporal trends in the burden of CLL provides critical evidence for guiding health strategies.
Methods
Using Global Burden of Disease 2021 data, we analyzed incidence, prevalence, deaths, disability-adjusted life years (DALYs), and the corresponding age-standardized rates (ASR), percentage changes, and estimated annual percentage changes (EAPC) for CLL from 1990-2021. Das Gupta’s method was used to analyze the changes in CLL burden. The frontier analysis was employed to further investigate the relationship between CLL burden and social development.
Results
Global CLL incidence, death, and DALYs burden have decreased, while prevalence increased. High social development index (SDI) regions remained associated with a heavier burden but showed a downward trend, while other SDI regions showed a certain upward trend. The prevalence of CLL in East Asia increased significantly. The incidence and mortality rates of male were still higher than those of female. Smoking, high body mass index, and occupational exposure to benzene or formaldehyde remained key risk factors.
Conclusion
The global burden of CLL has decreased, but significant regional differences remain.
Introduction
Chronic lymphocytic leukemia (CLL), the most common type of leukemia in adults, is characterized by the clonal proliferation and accumulation of large numbers of mature and typical CD5+, CD10- small B lymphocytes in the blood, bone marrow, lymph nodes, and spleen.1,2 Globally, CLL accounts for approximately 25%-30% of all leukemia cases. 3 Epidemiological data from 2021 reported more than 100,000 new cases and over 40,000 deaths worldwide. It predominantly affects the older adults and occurs more frequently in males. 4 Its incidence also varies significantly across geographic regions and ethnic groups, with higher rates observed in white populations in North America and Europe, and notably lower rates in Asian populations. 5
CLL progression is usually slow, but its heterogeneity is significant, and some patients may experience rapid progression and a poor prognosis.6-8 In recent years, the widespread use of targeted therapies (such as BTK inhibitors 9 and BCL-2 inhibitors 10 ) and immunotherapy 11 (such as anti-CD20 monoclonal antibodies) has significantly transformed the treatment landscape of CLL, resulting in substantial improvements in patient survival and quality of life. Despite the clinical significance of CLL in hematologic malignancies, comprehensive assessments of its global disease burden remain insufficient. In addition, the global burden of CLL is influenced by multiple factors, including population aging, improved diagnostic capability, therapeutic advances, and changing patterns of risk factor exposure. Therefore, a systematic evaluation of this burden is essential to elucidate temporal trends in epidemiology and to provide an evidence-based foundation for targeted prevention and control strategies.
The Global Burden of Disease 2021 (GBD 2021) study provides comprehensive estimates of 371 diseases and injuries, 88 risk factors, and 204 countries and regions, offering a valuable resource for understanding global epidemiological trends of CLL. 12 On this basis, we analyzed CLL data from 1990 to 2021, including incidence, prevalence, deaths, and disability-adjusted life years (DALYs), and calculated the estimated annual percentage change (EAPC) to assess temporal trends in disease burden. On this basis, we analyzed CLL data from 1990 to 2021, including incidence, prevalence, deaths, and (DALYs, and calculated the EAPC to assess temporal trends in disease burden.
Methods
Data Source
The data on CLL from 1990 to 2021 are obtained from the GBD 2021 database (https://vizhub.healthdata.org/gbd-results/). As our study does not involve any direct data collection from human participants or identifiable personal information, it does not require ethical approval. We obtained estimates of incidence, prevalence, deaths, and DALYs, along with the 95% uncertainty intervals (UIs). The reporting of this study conforms to the GATHER 13 and STROBE 14 guidelines.
Data Analysis
We analyzed the number of CLL patients by sex, social development index (SDI) region, and geographic region from 1990 to 2021, as well as the global age distribution at disease onset. To enable comparisons across regions while accounting for differences in age structure, the age-standardized rate (ASR) was calculated using the following formula
15
:

Temporal changes in disease burden were assessed using percentage change and EAPC. The percentage change in case number from 1990 to 2021 was calculated as:


EAPC and its 95% confidence interval (CI) were calculated as:

A rising trend was defined when both EAPC and its 95% CI were greater than 0, a declining trend when both were less than 0, and a stable trend when the 95% CI included 0. P-values <0.05 were considered statistically significant.
To decompose changes in CLL burden, Das Gupta’s method was applied, attributing variations to population growth, aging, and epidemiological trends. 16 Additionally, the frontier analysis was conducted to evaluate the relationship between CLL burden and social development. In this context, frontier refers to the lowest burden that can be achieved based on the development status of a country or region. Nonparametric data envelopment analysis was used for analysis.17,18 The distance between a country’s observed DALYs rate and the frontier value corresponding to the country’s SDI is defined as the effective distance, which represents the health gains that have not been achieved at the current level of development. 19 All analyses in this study were performed using the R software version 4.4.1.
Results
Trends in the CLL Incidence
In 2021, there were 117,987 new cases of CLL worldwide (95%UI: 98,330 to 132,718), reflecting a 103.56% increase since 1990 (Table S1, Figure 1(A)). The ASR for incidence from 1990 to 2021 exhibited a downward trend [EAPC: −0.47 (−0.67 to −0.28)]. Regional analysis based on the SDI revealed an increase in incident cases across all SDI regions from 1990 to 2021. However, the ASR in high SDI regions decreased in 2021 [ASR (95% UI): 2.38 (2.16 to 2.52)] compared to 1990 [ASR (95% UI): 3.08 (2.90 to 3.20)]. The ASR trend in low SDI regions remained stable, while the ASR in other SDI regions increased. By geographic region, Western Europe reported the highest number of incident cases in both 1990 [19,518 (18,323 to 20,520)] and 2021 [31,227 (27,486 to 34,098)]. In contrast, Oceania reported the lowest number of incident cases in both years [1990: 1 (0 to 4); 2021: 0 (0 to 1)]. High-income North America had the highest ASR in both 1990 [4.89 (4.60 to 5.06)] and 2021 [3.10 (2.80 to 3.27)], while South Asia had the lowest ASR [1990: 0.08 (0.03 to 0.11); 2021: 0.11 (0.05 to 0.15)] (Figure 1(C)). Trends in New CLL Cases. (A) Incidence Number or Rate Trend Dual Axis Chart From 1990 to 2021 (B) Age Structure of New Male and Female Cases in 2021, (C) ASR Trend Changes in Each Region
In the global distribution (Figure 2, Table S2), Monaco had the highest ASR in 2021 [6.94 (3.56 to 10.60)], while the Northern Mariana Islands had the lowest. Among the 185 countries reporting an increase in ASR, Jordan showed the largest rise [1361.09% (201.32 to 4465.83%)]. In contrast, 16 countries experienced a decrease, with Nauru showing the largest decrease [-89.94% (−99.20 to 649.93%)]. Sri Lanka exhibited the largest upward trend in ASR [EAPC: 4.97 (4.08 to 5.87)], while Mauritius had the largest downward trend [EAPC: −10.70 (−12.10 to −9.28)]. The Global Distribution of Incidence on (A) ASR in 2021, (B) Percentage Change Between 1990 and 2021, and (C) EAPC
Although the global trend of incident cases has declined over the past 30 years, an increasing trend has been observed in high-middle SDI, middle SDI, low-middle SDI regions. Globally, aging (60.70%) and population (55.45%) was the primary drivers of the disease burden, while epidemiological changes had a mitigating effect (Table S3). A similar pattern was observed in high SDI regions, where aging (79.90%) and population (71.30%) played a more significant role. In contrast, medium and low SDI regions were more influenced by epidemiological factors, although low SDI regions remained predominantly affected by aging and population dynamics. Among these regions, East Asia (48.71%) and Oceania (193.74%) were particularly impacted by epidemiological trends. At the country level, the United States was least influenced by epidemiological trends (−162.17%), with a greater impact from aging (139.27%) and population (122.90%). American Samoa (500.07%) exhibited the highest trend share (Table S4).
Trends in the CLL Prevalence
In 2021, the global number of CLL patients reached 721,066 (598,861 to 814,073), with an ASR of 8.34 (95% CI: 6.94 to 9.40) per 100,000 people (Figure S1A). The ASR demonstrated overall stability (EAPC = 0.15, 95% CI: −0.11 to 0.40). Regional analysis revealed a decreasing ASR trend in high SDI areas [EAPC (95% CI): −0.61 (−1.02 to −0.20)], whereas other SDI regions exhibited increasing trends (Table S1, Figure S1C). From a geographical perspective, East Asia had the largest number of patients in 2021, with a 616.77% increase compared to 1990. Australasia had the highest ASR at 22.88, and High-income Asia Pacific had the highest prevalence in 1990, with 30.40 per 100,000 people. Regarding ASR trends, Oceania experienced the largest decrease [EAPC (95% CI): −7.50 (−8.41 to −6.59)], while East Asia showed the largest increase [EAPC (95% CI): 4.80 (4.59 to 5.01)].
Regarding global trends (Figure S2), Northern Mariana Islands had the lowest ASR [95% CI: 0.01 (0.00 to 0.02)]. Countries with low prevalence (0 to 1) were mainly located in West Africa, South Asia, and Oceania. Monaco had the highest ASR [95% CI: 46.32 (23.19 to 72.66)]. Nauru experienced the largest decrease in the percentage change in number of cases (−88.32%), while Jordan showed the largest increase, with a 2261.62% rise in the patient numbers. In the global EAPC distribution, 34 countries or territories showed decreasing ASR trend, with the largest decrease observed in Mauritius [95% CI: −10.29 (−11.86 to −8.70)]. In contrast, 160 countries or territories showed an increasing trend, with Sri Lanka showing the largest increase [95% CI: 6.98 (6.04 to 7.94)].
Decomposition analysis (Table S3) revealed that global prevalence was primarily driven by age (45.59%) and population (45.66%), with the epidemiological trends only 8.75%. The effect for males (11.96%) was slightly greater than that for females (2.43%). Among SDI regions, age (64.24%) and population (62.03%) were dominant factors in high SDI areas, while epidemiological trends were more influential in middle SDI and low-middle SDI regions. The proportions of these factors in high-middle SDI and low SDI areas were relatively balanced.
Trends in the CLL Deaths
In 2021, the global number of CLL deaths reached 45,573 (95% UI: 37,693 to 51,085), reflecting a 55.66% (18.39% to 98.54%) increase from 1990 (Figure S3A). Among the SDI regions, only low-middle SDI regions exhibited an upward trend in mortality, while all other SDI regions showed downward trend. Western Europe recorded the highest number of deaths. The ASR trends in six geographic regions (South Asia, Central Europe, Andean Latin America, Western Sub-Saharan Africa, Central Sub-Saharan Africa, and Southern Sub-Saharan Africa) were increased, with the largest upward trend observed in Western Sub-Saharan Africa [EAPC (95% CI): 0.80 (0.74 to 0.85)]. In contrast, Tropical Latin America and North Africa and the Middle East maintained stable trends. Western Europe showed the most significant downward trend [EAPC (95% CI): −1.41 (−1.54 to −1.28)] (Figure S3C).
Regarding global trends (Figure S4), Ethiopia had the highest ASR of deaths in 2021(2.33 per 100,000 people), while the Northern Mariana Islands had the lowest (0.0015 per 100,000 people). A total of 26 countries experienced a decrease death numbers, whereas 178 countries showed increase (Table S2). Jordan demonstrated the largest percentage increase in death numbers (736.50%), whereas the country with the largest decrease was Nauru, with a reduction of −90.34%. Among the ASR trends, 25 countries showed stability, and 72 countries experienced an upward trend. Sri Lanka showed the largest increase [EAPC (95% CI): 3.28 (2.44 to 4.14)] and Afghanistan showed the smallest increase [EAPC (95% CI): 0.06 (0.03 to 0.10)]. The ASR trend in 105 countries decreased, with the largest decrease observed in Mauritius [EAPC (95% CI): −10.98 (−12.25 to −9.70)].
The global mortality rate was declining, while the total number of deaths was increased, primarily due to ageing (81.41%) and population (89.43%) factors. Epidemiological factors were contributing to the reduction in the mortality rate. In the low-middle SDI and low SDI regions, the mortality rate was exacerbated by epidemiological factors, with contributions of 18.49% and 14.23%, respectively. Notably, in Oceania, epidemiological trends (236.54%) represent the primary factor driving increased mortality (Table S3).
Trends in DALYs Caused by CLL
Global DALYs showed a downward trend [EAPC (95% CI): −1.52 (−1.63 to −1.40)] (Figure S5). The primary drivers were age (117.02%) and population (119.60%), while epidemiological trends (−136.62%) contributed to the reduction in DALYs. However, an exception was observed in low-middle SDI regions, where an upward trend was evident, potentially attributable to epidemiological factors (15.39%). Among the regions, only Andean Latin America [EAPC (95% CI): 0.35 (0.10 to 0.59)], Western Sub-Saharan Africa [EAPC (95% CI): 0.72 (0.67 to 0.78)], Central Sub-Saharan Africa [EAPC (95% CI): 0.47 (0.42 to 0.52)], and Southern Sub-Saharan Africa [EAPC (95% CI): 0.72 (0.45 to 0.98)] exhibited an upward trend.
The global DALY trend revealed that Ethiopia had the highest age-standardized DALY (ASR DALY) rate, at 49.60 (26.05 to 83.55) per 100,000 people, while the Northern Mariana Islands had the lowest rate, at 0.02 (0.01 to 0.08) per 100,000 people (Figure S6). Sri Lanka experienced the most rapid DALYs increased [EAPC (95% CI): 3.35 (2.52 to 4.18)], primarily driven by epidemiological trends (41.95%), age (27.99%), and population (30.05%) factors (Table S4).
The main risk factors for CLL were categorized into 3 levels: behavioral risks, metabolic risks, environmental/occupational risks (primary), tobacco use, high body-mass index, occupational carcinogens (secondary), and smoking, as well as occupational exposures to benzene and formaldehyde (tertiary). The population and uncertainty interval of DALYs associated with all risk factors were 238,075 (148,124 to 348,309), accounting for 23.72% (15.83% to 32.73%) of the total DALYs (Table S5). The most significant risk factor associated with chronic lymphocytic leukemia in high and high-middle SDI regions was smoking, whereas elevated body mass index (BMI) demonstrated the strongest association in low SDI regions (Table S6).
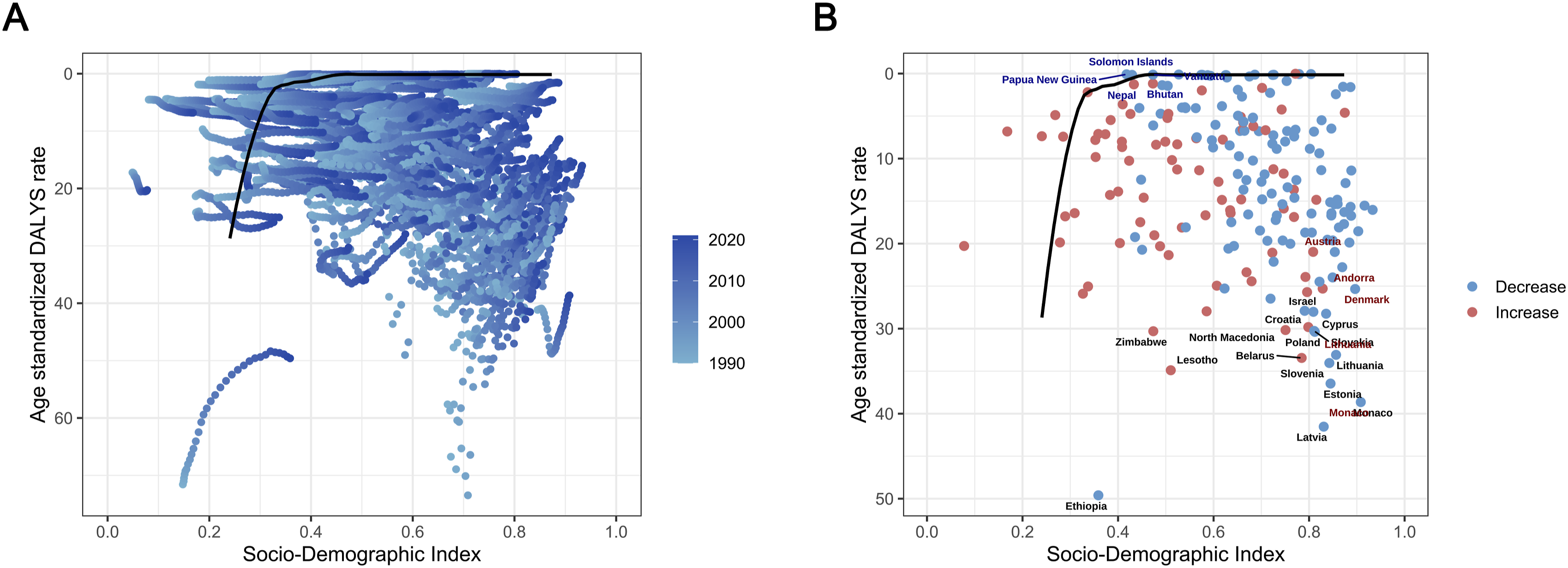
The relationship between SDI and DALY rate (Figure 3) indicates that when the SDI is below 0.4, the burden of CLL gradually decreases (Figure 4(A)). Between SDI values of 0.4 and 0.8, the burden increases. And when the SDI exceeds 0.8, the burden decreases again. Frontier analysis suggests a gradual temporal reduction in CLL burden, with higher-SDI countries demonstrating greater potential for burden improvement (Figure 4(B)). Relationship Between Social Development Index and Age-Standardized DALYs Rate From 1990 to 2021 Frontier Analysis of the Relationship Between SDI and Age-Standardized DALYs Rates. (A) The Progress of the Year (B) Each Point Represents a Country, the 15 Countries that Deviate Most Significantly From the Boundary (Black Solid Line) are Marked in Black, the 5 Countries With the Smallest Distance Difference Among Low SDI (<0.5) Countries are Marked in Blue, and the 5 Countries With the Largest Distance Difference Among High SDI (>0.5) Countries are Marked in Red. Countries Exhibiting Increased DALYs Rates in 2021 Compared to 1990 are Shown in Red, whereas Those With Decreased Rates are Displayed in Blue
Sex Patterns of CLL
Whether it was incidence, prevalence or deaths, the proportion of males is higher than that of females (Figure 1B, S1B, S3B). From 1990 to 2021, the global ASR of incidence exhibited a downward trend in both males [−0.63 (−0.81 to −0.45)] and females [−0.39 (−0.59 to −0.19)]. New cases of CLL predominantly occurred in individuals over 20 years of age, with the number of males surpassing that of females in most age groups, except for those aged 90-94 years and those over 95 years. The sex disparity in prevalence mirrored that of incidence, with a stable trend in females [EAPC (95% CI): −0.06 (−0.29 to 0.16)] and an increasing trend in males [EAPC (95% CI): 0.31 (0.03 to 0.58)]. In terms of mortality, the ASR for males remained higher than that for females. However, the global CLL mortality rate showed a downward trend overall [EAPC (95% CI): −1.45 (−1.56 to −1.34)], with the decline in females [EAPC (95% CI): −1.66 (−1.77 to −1.54)] being more pronounced than that in males [EAPC (95% CI): −1.35 (−1.46 to −1.25)].
Discussion
Our study investigates the global epidemiology and temporal trends of CLL from 1990 to 2021 using the most recent GBD 2021 database. We systematically analyzed global data on CLL incidence, prevalence, mortality, and DALYs, employing rigorous epidemiological assessment methods. Our findings reveal an overall decline in the global CLL burden over the past 3 decades, although certain regions and countries continue to experience increasing trends.
The CLL burden varies significantly across different SDI regions. High SDI regions exhibited a heavier burden, albeit with a downward trend in recent years. This pattern may be largely explained by distinct epidemiological factors, including broader cancer registry coverage, advanced diagnostic techniques, and an aging population, which collectively enhance case detection while increasing the overall burden. In these regions, early diagnosis, improved treatment accessibility, and the widespread use of novel therapies have contributed to declining ASR despite persistently high incidence. In contrast, ASR in middle and low-middle SDI regions continued to show an upward trend, largely due to the expanding registry systems and improved detection capabilities, which together have revealed more previously undetected cases. 20 Only the ASR trend in the low SDI region is stable. This may be influenced by unfavorable epidemiological factors, including limited screening programs, inadequate hematology diagnostic facilities, and incomplete case reporting, which collectively lead to underdiagnosis and underestimated disease burden. 21 The advancement of drug research and development has notably influenced the burden of CLL in high SDI regions. New targeted therapies, such as B-cell lymphoma-2 (BCL-2) inhibitors and Bruton tyrosine kinase (BTK) inhibitors (eg, acalbrutinib, zanubrutinib, and venetoclax), have increased by 20.8% and 23.6% from 2015 to 2024 in the United States,22,23 substantially altering the treatment landscape of CLL in developed countries. However, the high cost and limited accessibility of these drugs have led to significant inequalities in CLL treatment worldwide. These disparities underscore the urgent need for targeted interventions and the allocation of resources in resource-limited settings to address the growing burden of CLL. In addition, the paradoxical phenomenon of declining ASR alongside increasing numbers of new CLL cases may reflect not only the effects of population aging and growth but also improvements in diagnostic accuracy and disease recognition. Advances in diagnostic technologies, such as flow cytometry, immunophenotyping, and molecular testing, have substantially enhanced the early and accurate detection of CLL. 24 These developments may have led to a marked increase in the “true incidence” recorded by cancer registries over time. Moreover, the expansion of screening programs and more comprehensive registry coverage have further amplified this trend.
Geographically, the incidence, ASR of incidence, and prevalence of CLL were higher in Western Europe, high-income North America, and Australia. This geographical difference may be attributed to genetic factors. Studies have demonstrated that the incidence of CLL varies significantly among different races and populations, suggesting the pivotal role of genetic factors in disease development. 25 For instance, the risk of CLL is not increased in Asians who have settled in Western countries such as the United States and Europe, further indicating that genetic factors are key determinants of CLL susceptibility. 26 Genome-wide association studies (GWAS) have identified several genetic variants associated with CLL risk, including single nucleotide polymorphisms (SNPs) located in regions such as chromosome 6p25.3 (IRF4), 11q24.1 (ATM), and 15q23 (BMF).27,28 These genetic variants may increase susceptibility to CLL by affecting biological processes such as immune regulation, DNA repair, and apoptosis. 29 However, racial differences in CLL-related SNPs have been observed. Notably, some CLL SNPs identified in European populations were not significantly associated with susceptibility in Chinese populations, 30 which may explain the regional differences in CLL incidence. Additionally, we observed a significant increase in the prevalence of CLL in East Asia, which could be attributed to rapid population aging and significant improvements in healthcare in the region (particularly in Japan, South Korea, and China). 31 Advances in diagnostic technologies and increased disease awareness have contributed to the identification of more cases.
Globally, we found that CLL incidence, mortality, and DALYs were higher in males than in females. Sex-specific analysis revealed notable differences in the burden of CLL. Previous studies have shown that CLL is more common and exhibits a more aggressive clinical course in men than in women, 32 a trend confirmed by our results. The higher incidence and mortality in men may be attributed to a combination of biological factors 33 (eg, genetic abnormalities, hormonal differences) and behavioral factors (eg, greater exposure to environmental risk factors). Lin et al 34 found that differences in DNA methylation may contribute to sex differences in CLL risk through an epigenome-wide association study (EWAS). In addition, females may have a stronger immune response due to the presence of 2 X chromosomes. Key X-linked immune genes such as TLR7, TLR8, CD40L, and KDM6A enhance women’s immune surveillance capabilities, which may contribute to the lower incidence of CLL in women.35,36 However, current research remains insufficient to fully explain the mechanisms underlying these sex differences. Understanding these disparities is crucial for developing targeted prevention and treatment strategies to address the specific needs of each sex.
We also investigated risk factors influencing CLL DALYs. Among these, smoking stands out as a major risk factor. Cigarettes release numerous carcinogens, including tobacco-specific nitrosamines, polycyclic aromatic hydrocarbons, and volatile organic compounds, 37 which are implicated in cancer development. While a clear association between tobacco use and CLL incidence has not been established, several GBD studies on CLL have suggested smoking as a potential risk factor associated with its burden.20,30 Thus, tobacco control remains an important preventive measure against CLL, and global efforts to reduce smoking rates should be intensified. Additionally, a high BMI is a significant risk factor. Research has shown that obesity may be linked to CLL incidence and mortality. 38 In a cohort study, obese patients exhibited poorer baseline responses to induction therapy containing rituximab and had lower complete remission rates. 39 Therefore, interventions targeting obesity, such as promoting healthy diets and physical activity, could help mitigate the impact of metabolic risk factors on CLL incidence. Importantly, the strongest risk factors varied across SDI regions, which may reflect differences in lifestyle, living standards, and healthcare systems. In high-SDI regions, historical patterns of tobacco consumption and longer life expectancy may increase the observed contribution of smoking; however, given the rising prevalence of smoking in low-SDI regions, it has also become a major risk factor. 40 In middle- and high-middle-SDI regions, rapid nutritional transitions have amplified the role of high BMI. 41 In low-SDI regions, factors such as limited healthcare access, environmental or occupational exposures, and competing health priorities may alter the relative weight of smoking and metabolic risks. These findings underscore the need for region-specific strategies tailored to the dominant risk profiles.
Although aging is recognized as a major contributor to the global CLL burden, few studies have proposed population-specific interventions for the elderly. For older adults, geriatric assessment can guide individualized treatment planning, balancing efficacy and tolerability. Age-appropriate therapy selection, including dose-adjusted chemotherapy or targeted therapies such as BTK inhibitors, may improve outcomes while minimizing adverse effects. 42 Supportive care measures, such as infection prevention, nutritional optimization, and management of comorbidities, are also crucial for maintaining quality of life in this population. 43 Implementing these interventions can help mitigate the impact of aging on CLL burden, particularly in regions with rapidly aging populations.
Compared with previous GBD-based studies on CLL, our analysis provides several novel contributions. For instance, Ou et al 44 primarily described incidence, mortality, and DALY trajectories from 1990 to 2019 and projected trends to 2030 using EAPC, but did not decompose the relative contributions of population growth, aging, and epidemiological changes. Similarly, Rehman et al 45 systematically examined ASDR and DALYs by region and SDI but lacked a frontier analysis to benchmark national performance relative to their socio-development levels. Chen et al 46 employed decomposition methods to analyze overall leukemia burden, partitioning demographic and epidemiological drivers, but did not specifically focus on CLL or apply frontier analysis to evaluate country-level disparities. Our study used the updated GBD 2021 database and found a global decline in CLL burden, which contrasts with the increasing trend reported in GBD 2019. 20 We further applied decomposition analysis to separate the effects of population growth, aging, and epidemiological changes on case numbers. In addition, we performed frontier analysis to evaluate disparities between CLL burden and social development. These approaches extend and complement previous research.
Our study has several limitations. First, the accuracy of GBD data depends on the quality of input data from various sources, which may vary by region. Furthermore, the study period concludes in 2021, and more recent data may reveal further trends or changes in the burden of CLL. Finally, as with all GBD analyses, it is based on observational data and therefore cannot establish definitive causal relationships between risk factors and disease outcomes.
Conclusion
From 1990 to 2021, the global incidence, mortality, and DALY burden of CLL decreased, while the prevalence increased. High-SDI regions, such as Western Europe, high-income North America, and Australia, have a heavy burden but show downward trend. Conversely, regions with lower SDI show an upward trend. Notably, East Asia experienced a significant increase in CLL prevalence. Furthermore, persistent sex disparities were observed, with males demonstrating higher incidence and mortality rates compared to females. Smoking continues to be 1 of the major risk factors for CLL. These findings underscore the need for region- and population-specific strategies. Priorities include improving access to novel therapies in high-SDI regions, strengthening primary care and exposure prevention in low- and middle-SDI regions, and tailoring interventions to the elderly population to address the impact of aging.
Supplemental Material
Supplemental Material - Global Burden of Chronic Lymphocytic Leukemia From 1990 to 2021
Supplemental Material for Global Burden of Chronic Lymphocytic Leukemia From 1990 to 2021 by Chen Chen, Ling Wang, Shenghong Du, Yu Qiu, Yan Liu, Qingliang Teng in Cancer Control
Footnotes
Ethical Approval
Not applicable. The study used publicly available, anonymized, and aggregated data from the Global Burden of Disease (GBD) database. Ethical approval and informed consent were therefore not required.
Author contributions
Chen Chen: Data curation, Formal Analysis, Methodology, Resources, Software, Validation, Writing – original draft. Ling Wang: Data curation, Formal Analysis, Software, Visualization, Writing – original draft. Shenghong Du: Formal Analysis, Methodology, Resources, Visualization, Writing – original draft. Yu Qiu: Formal Analysis, Methodology, Validation, Writing – original draft. Yan Liu: Conceptualization, Investigation, Project administration, Supervision, Validation, Writing – review & editing. Qingliang Teng: Data curation, Formal Analysis, Software, Writing – original draft.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the This work was supported by Tai’an Science and Technology Development Guiding Project (No. 2022NS217), and the Shandong Province Medical and Health Science and Technology Project (No. 202403040826).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.