
Abstract
Introduction
Patient-centricity calls for accurate consideration of patients’ preferences at every step of the care pathway. Decision aids (DAs) are interventions that provide patients with information about treatment options, enabling shared decision-making (SDM). This study investigated the practice of SDM by breast cancer (BC) specialists and the diffusion of DAs in the treatment of BC in Europe. The secondary objective of the study was to explore heterogeneity across respondents’ subgroups.
Methods
A prospective, cross-sectional, cross-country questionnaire targeting breast specialists was distributed online across breast cancer networks at both national and European level. The survey results were analyzed descriptively. Mann-Whitney-U tests, and probit regressions were performed to explore differences between subgroups.
Results
Respondents were mostly medical oncologists and surgeons. Respondents expressed high comfort with SDM approach (mean: 4.29, CI95%: 4.15-4.44). The majority reported DAs were available, and used, in their organization. Statistically significant gender differences were observed, indicating that female physicians might be more prone to adopting SDM approaches with patients.
Conclusions
Patient-centricity calls for consideration of patients’ values. The specialists in this survey showed a promising attitude towards SDM. DAs availability translates into use, although this mainly refers to paper tools, whereas digital tools seem mostly illustrated in the literature.
Introduction
Background
Thanks to the latest scientific and therapeutic advancements, breast cancer (BC) can now be considered a chronic disease for many patients, rather than a life-threatening illness. 1 In the past few years, plenty of treatment options became available to patients, ranging from chemo-to radiotherapy, or from endocrine-based to surgical interventions. In this context, accounting for patients’ preferences and values becomes not only ethically appropriate, but also crucial for therapeutic success.2,3 Patient decision aids (DAs) are interventions that support patients by making their decisions explicit, providing information about treatment options, and helping clarify congruence between decisions and personal values. A recent systematic review revealed that people exposed to DAs feel more knowledgeable and clearer about their values, which leads to a more active role in the decision-making process. 4
DAs facilitate shared decision-making (SDM), namely a process of collaboration between patients and clinicians to reach a joint decision about care involving multiple medically appropriate options.5,6 SDM is achieved by using appropriate communication techniques, understanding of the context in which patients live, and embracing their values on what is a good treatment outcome. 7 SDM is known to increase quality of cancer care, and is associated with less decision regret, better treatment adherence, less treatment failure.8-10 Recent updates of international BC clinical guidelines emphasized the need to foster the adoption of SDM approaches in clinical practice.11,12 Relatedly, attention towards the impact that patient-clinician gender-concordance might have on clinical decision-making has recently emerged. 13 On one hand, gender of treating physicians has been shown to have an impact on patient outcomes14,15; on the other hand, the physicians most involved in the treatment decision-making of women diagnosed with BC have the potential to significantly contribute to the spread of SDM approaches, and as such the influence of specialists like oncologists and surgeons has been investigated in previous studies. 16
The characteristics of DAs have changed over time, evolving from plain, paper-based interventions to increasingly sophisticated digital solutions. Quality standards, such as the International Patient Decision Aids Standards (IPDAS), have been developed, thus establishing a shared evidence-informed framework to guide developers and researchers in designing, building, and evaluating these tools. 17 However, previous works called for more knowledge on DAs, revealing the need for stronger evidence base on their development, implementation and cost-effectiveness. 18 Despite the growing interest shown both at the policy and professional levels, current use of DAs in clinical settings, as well as factors associated to their adoption, are therefore not clear.
Objectives
Using a cross-sectional survey, this work was primarily aimed at investigating the perceived practice of SDM by breast specialists and the uptake and diffusion of DAs in the treatment of BC care in Europe. The secondary objective of the study was to identify and explore heterogeneity across subgroups of respondents.
Methods
Survey Development
This is a prospective cross-sectional study. The reporting of this study conforms to STROBE guidelines. 19 The process of developing the survey questionnaire was iterative and followed a systematic approach. 20
Step 1: Item generation
To explore the individual attitude towards SDM and the use of DAs as tools to support breast specialists in engaging their patients in treatment-related choices, a scoping review of the literature was performed to inform the development of the study questionnaire. The survey items were initially drafted by two researchers based on existing questionnaires or interview guides retrieved in the research streams of SDM and DAs in BC care. The questionnaire was developed in English.
Step 2: Survey draft
The Questionnaire Appraisal System (QAS) framework was used, to assess questionnaire items’ reading, instructions, clarity, assumptions, knowledge/memory, sensitivity/bias, response categories and other. 21 Then, the questionnaire flow was evaluated jointly by the research team and an oncologist, focusing on the order, logic, and relevance of the questions. As result, the survey structure was updated, grouping questions differently or shifting question blocks. The resulting survey draft that formed the basis of cognitive testing contained up to 17 questions organized across three sections: (i) profiling, (ii) communication style and decision-making process, (iii) patient DAs. As for the profiling section, we used the term “gender” to refer to women and men as social categories. We believe this is consistent with our research focus on the behavioral and social dimensions of healthcare professionals’ experience. 22
Step 3: Cognitive testing
Cognitive interviewing is widely employed for pre-testing survey instruments, to evaluate whether respondents interpret the questions consistently, as intended by the investigator. Both think-aloud and verbal probing techniques have been used. 23 To select participants in the process of cognitive testing, a purposive sampling selection was applied satisfying criteria related to country, age, experience and gender. Overall, nine healthcare professionals were interviewed, representing 7 countries (ie, Albania, Belgium, France, Germany, Italy, Portugal, Spain), and with seniority that ranged from 2 to 40 years. All interviews were recorded. The questionnaire was not translated in national languages as English was deemed appropriate for the target respondents (ie, BC professionals regularly consult documents, guidelines, and various sources written in English).
Step 4. Final questionnaire
The final version of the questionnaire received ethical approval in November 2021 from the Ethical Review Board of Bocconi University (Milan, Italy), with application ID FA000375. The final questionnaire contained 17 questions, with filtering questions distinguishing between users, non-users, and potential users of DAs. Figure 1 displays the structure of the survey, reported in its integral version in Appendix Aand uploaded on Zenodo (10.5281/zenodo.7925762). Survey Flows by Users, Non-users and Potential Users. Abbreviations: PtDA = Patient Decision Aid; Q = Question; SDM = Shared Decision-Making.
Recruitment and Data Collection
Target respondents were breast specialists, specifically medical oncologists, surgeons, radiologists, radiation oncologists or any other professionals who may interact with breast patients at some point of the care pathway. The survey was disseminated through BC networks and scientific associations, both at national and international level in Europe. These included European Society of Breast Cancer Specialists (EUSOMA), European Commission Initiatives on Breast and Colorectal Cancer (ECIBS), Breast Surgical Oncology Platform (BRESO), Central-Eastern European Breast Cancer Surgical Consortium (CEEBCSC), Breast Centers Network (BCN), Seno Network Italia, Unicancer France, German Breast Group (GBG), Europa Donna Italia Scientific and Technical Committee. The breast specialists were approached via dedicated mailings or internal newsletters. Informed consent was obtained from all participants prior to survey access. Data was collected from April to August 2022 through the commercial electronic platform for survey services Qualtrics XM©. Due to the open distribution strategy of the survey, the response rate could not be calculated nor estimated. The final sample considered for the analyses included respondents who completed at least 70% of the survey items.
Data Analysis
Descriptive statistics of survey data were computed. We reported absolute and relative frequencies for categorial variables and means with associated standard deviations for metric variables. No missing data imputation was performed. Results were analysed both by gender, and professional roles (ie, medical oncologists, surgeons, and any other medical specializations). The breast units (BUs) could be classified as being certified based on nation-specific and/or European quality standards (ie, EUSOMA Breast Centres Certification), as opposed to not being classified under any certificates. Perceived barriers and facilitators to DA uptake were analyzed with the dual perspective of current users and non- or potential users. Means were compared using non-parametric Mann Whitney U tests. A series of ordered probit regression analyses were carried out for categorical variables that showed significant differences in the means across population subgroups. Each outcome was regressed on five theoretically grounded predictors: seniority, professional role, type of BU, the endorsement of “shared” decision-making archetype, and gender. Seniority was included based on evidence from diffusion-of-innovation research showing that more clinicians with longer tenue tend to adopt SDM practices more slowly and often perceive fewer relative advantages in doing so. 24 Professional role was considered because surgeons, oncologists, and radiologists play distinct roles in information exchange and preference elicitation. 16 Identification with the “shared” SDM archetype (Charles et al) was used as a proxy for a clinician’s general propensity to involve patients in treatment decisions. The type of breast unit (certified vs not certified) was included to account for the organizational culture and resource endowment, known to modulate the implementation of SDM interventions in breast-cancer services. 25 Finally, gender was retained due to documented differences in communication style and decision-making authority in oncology settings. Statistical significance was set at P < 0.05. 95% confidence intervals (95%CI) were reported. Given the exploratory nature of the analyses, P-values were interpreted descriptively and no power calculation was performed. As a sensitivity check, we conducted additional analyses excluding countries with fewer than 10 respondents. Analyses were performed using the Stata 17.0 statistical package (StataCorp LLC, College Station, TX, USA).
Results
Participants’ Profiling
Descriptive Information of the Study Participants (Total Sample)

Abbreviations: BU = Breast Unit; SD = Standard Deviation.
*At BU level.
Notes. 1 Others include: Albania, Austria, Belgium, Bosnia, Bulgaria, Croatia, Cyprus, Denmark, Georgia, Greece, Iceland, Latvia, Lithuania, Netherlands, Norway, Poland, Russia, Serbia, Slovenia, Spain, Turkey.
Decision-Making Archetypes, Process and Influencing Factors
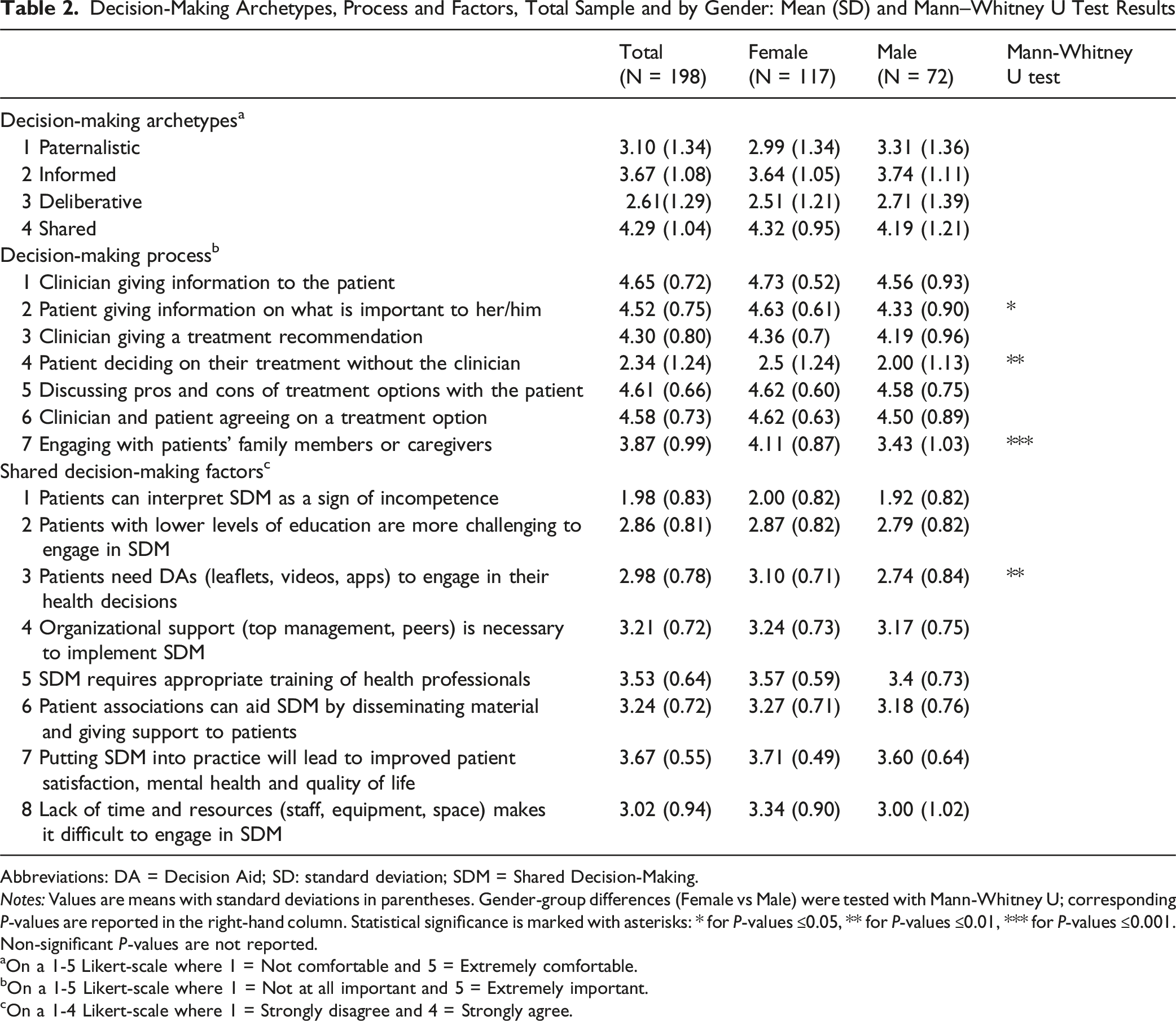
Decision-Making Archetypes, Process and Factors, Total Sample and by Gender: Mean (SD) and Mann–Whitney U Test Results
Abbreviations: DA = Decision Aid; SD: standard deviation; SDM = Shared Decision-Making.
Notes: Values are means with standard deviations in parentheses. Gender-group differences (Female vs Male) were tested with Mann-Whitney U; corresponding P-values are reported in the right-hand column. Statistical significance is marked with asterisks: * for P-values ≤0.05, ** for P-values ≤0.01, *** for P-values ≤0.001. Non-significant P-values are not reported.
aOn a 1-5 Likert-scale where 1 = Not comfortable and 5 = Extremely comfortable.
bOn a 1-5 Likert-scale where 1 = Not at all important and 5 = Extremely important.
cOn a 1-4 Likert-scale where 1 = Strongly disagree and 4 = Strongly agree.
Then, respondents were asked to state how relevant they found factors commonly involved in a decision-making process on a 1-5 scale. Providing patients with information was considered the most important dimension (mean: 4.65, CI95%: 4.55-4.75), followed by discussing pros and cons of treatment options with the patient (mean: 4.61, CI95%: 4.52-4.70), and agreeing with patients upon a treatment regimen (mean: 4.58, CI95%: 4.48-4.68). Female respondents reported significant higher scores compared to males with respect to item 2 (Patient giving information on what is important to her/him, P = 0.0179), item 4 (Patient deciding on their treatment without the clinician, P = 0. 0031) and item 7 (Engaging with patients’ family members or caregivers, P = 0.000).
Finally, the survey investigated the perceived barriers and facilitators of SDM using a 1-4 scale (a non-neutral scale was used to accrue respondents’ preferences). Females reported higher agreement scores to any SDM-related items than male responders. For some items, the gender difference was significant.
Sensitivity analyses excluding countries with fewer than 10 respondents, reported in Appendix C, revealed consistent patterns of item relevance across gender groups, supporting the validity of the associations identified in the overall sample. To explore whether cultural factors associated with different countries might influence shared decision-making (SDM) practices, additional analyses were conducted by clustering responses according to the type of healthcare system, namely tax-based, insurance-based, or mixed systems; however, no relevant relationship across groups were detected (see Appendix D).
Ordered Probit Regression Results for Four [(1)-(4)] Decision-Making Related Outcomes: Effect of Professional Role, Gender, Seniority, Decision-Making Archetype, and Type of Breast Unit
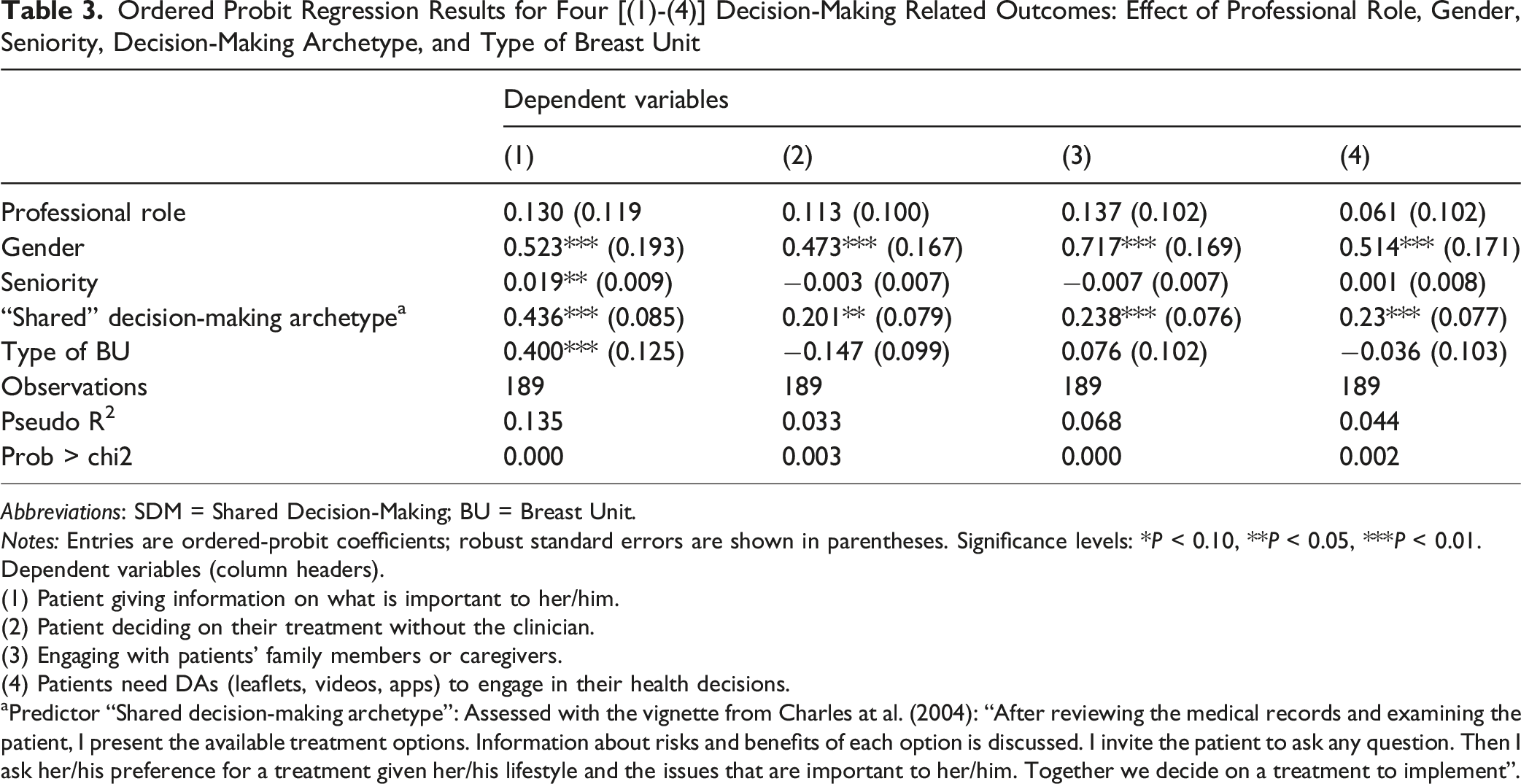
Abbreviations: SDM = Shared Decision-Making; BU = Breast Unit.
Notes: Entries are ordered-probit coefficients; robust standard errors are shown in parentheses. Significance levels: *P < 0.10, **P < 0.05, ***P < 0.01.
Dependent variables (column headers).
(1) Patient giving information on what is important to her/him.
(2) Patient deciding on their treatment without the clinician.
(3) Engaging with patients’ family members or caregivers.
(4) Patients need DAs (leaflets, videos, apps) to engage in their health decisions.
aPredictor “Shared decision-making archetype”: Assessed with the vignette from Charles at al. (2004): “After reviewing the medical records and examining the patient, I present the available treatment options. Information about risks and benefits of each option is discussed. I invite the patient to ask any question. Then I ask her/his preference for a treatment given her/his lifestyle and the issues that are important to her/him. Together we decide on a treatment to implement”.
Patient Decision Aids
Availability and Use of DAs (Distribution of Responses)

Abbreviations: DAs = Patient Decision Aids.
Moment of DA Use and Usage Frequency (Distribution of Responses, Total Sample)

Notes: Percentages are calculated out of the total number of observations in each DA category.
Perceived Enablers to the Uptake of DAs

Abbreviations: eHR = Electronic Health Records; DA: decision aids; SD: standard deviation.
Notes: Statistical significance is indicated with: * for P-values ≤0.05, ** for P-values ≤0.01, *** for P-values ≤0.001. P-values are calculated using Mann Whitney U test. On a 1-5 Likert-scale where 1 = Not at all relevant and 5 = Extremely relevant.
In terms of DA quality, leveraging on evidence-based information had the highest score both amongst current users of DAs (mean: 4.09, CI95%: 3.91-4.27), and potential users (mean: 4.29, CI95%: 4.10-4.48), whereas the factors that are perceived less important are the integration within the hospital IT system (mean: 3.41, CI95%: 3.19-3.63) and time of usage (mean: 3.90, CI95%: 3.72-4.08) for current users and potential users, respectively. In each item analyzed, self-reported values of current users are lower compared to the corresponding self-reported values of potential users.
Lastly, Figure 2 displays the perceived barriers to the uptake of DAs in the clinical practice from the non-user perspective (ie, specialists who declared not to use DAs even when in principle they were available to them, and specialists employed in centers where DAs were not provided). Interestingly, amongst respondents who could use available tools to facilitate treatment decisions, 9 (60%) nevertheless adopt different possibly unstructured or uncodified strategies, to engage their patients. The percentage of non-users is higher than the corresponding share of users in most of the question items. This gap in self-reported values is particularly relevant with respect to the need of an organized system to distribute the DAs within an organization (N = 6, 46% vs N = 3, 20%), and training for an accurate use of the DAs (N = 4, 31% vs N = 1, 7%). Perceived Barriers to the Uptake of DAs
Discussion
In an era of sustained commitment to patient-centricity at every step of the health care pathway, this survey investigated clinicians’ attitudes toward SDM and current use of DA in the area of BC. 29 The findings highlight a vigorous interest for participatory communication approaches with patients. Notably, our results suggest that the self-reported inclination to genuinely adopt a participatory and inclusive communication style is not randomly distributed among professionals, but is more often observed among female clinicians and those who, in line with the SDM archetype proposed by Charles et al, 26 demonstrate a greater tendency to engage patients as active partners in the decision-making process. This pattern was consistent across all dependent variables analyzed, indicating a broader alignment between individual orientations toward SDM and actual behaviors. While the intensity of DAs usage can vary based on the gender, DAs appear to be usable in different moments, ranging from first visits to follow-ups. On one hand, the availability of DAs seems to translate into actual use; on the other hand, professionals who do not have access to DAs within their organization still exhibit a strong inclination to use these instruments. DAs are accessible in multiple formats, with paper tools emerging as the most common in practice. Overall, the survey illustrates a promising landscape for DAs, yet a few specialists who were surveyed expressed a preference for not using these tools despite their availability. In such cases, long-established, tacit strategies for patient engagement still prevail and represent a latent obstacle to the wider diffusion of more sophisticated, evidence-based instruments. Lastly, female respondents appeared better inclined to use DAs in the clinical encounters, suggesting that gender of treating physician might play a role in the acceptance and use of these tools. Although this evidence is only reflective of the self-reported perceptions of respondents, this survey seems to suggest that there is not a one-size-fits-all approach with respect to how DAs are currently employed with patients.
Through widespread dissemination with BC networks, this study contributed to increasing awareness of what factors might influence SDM among health practitioners and has the potential to stimulate further adoption of SDM practices in the future. Yet, the fact that the literature on SDM and the use of DAs in BC care is more extensively developed in North America, particularly the United States (US), suggests that cultural factors, such as norms, values, and underlying assumptions, may influence how clinicians engage with patients and, ultimately, how health technologies are adopted in practice. 28 Indeed, several studies from the US have shown that structured policies, reimbursement mechanisms, and legal mandates have supported the systematic integration of SDM and DAs into clinical practice, especially in oncology. For example, the implementation of the Patient Protection and Affordable Care Act in the US explicitly emphasized patient engagement and SDM (establishing a program “to provide for the phased-in development, implementation, and evaluation of SDM using patient decision aids to meet the objective of improving the understanding of patients of their medical treatment options”), 30 leading several health organizations to adopt institutional SDM requirements. In contrast, many European healthcare systems lack unified policies or incentives supporting SDM, with substantial variation across countries in the degree to which SDM is embedded in national cancer strategies or clinical guidelines. Moreover, specific features of European healthcare systems, such as varying degrees of centralization or differences in primary vs specialist care pathways, may contribute to inconsistent implementation of DAs. Efforts to scale up SDM practices across Europe may benefit from coordinated strategies that combine policy incentives, clinician training, and integration of DAs into clinical workflows and national care standards.
In general, applying research findings in real-world settings can be challenging, and there may be difficulties in adopting new clinical innovations into routine practice. 31 The underlying factors facilitating or impeding the adoption of DAs in BC have been synthetized in a prior review of the literature under the lens of a consolidated implementation science framework, 32 concluding that knowledge to support the sustained implementation of SDM interventions in BC care was still limited. 25 Building on this, this survey interestingly highlighted that many of the proposed barriers to DAs uptake were viewed as obstacles more by individuals who did not use nor have the tools, possibly suggesting that the absence of access or usage of these instruments may result in an overestimation of the challenges involved in their use.
Based on these findings, we suggest that healthcare administrators prioritize integrating SDM practices and DAs into routine workflows by embedding them in eHRs, supporting staff training on their effective use, and allocating protected time during patients’ visits for SDM conversations. From a policy perspective, national and regional health authorities could develop formal guidelines and incentives that recognize SDM as a quality-of-care indicator, particularly in oncology. Moreover, ensuring equitable access to validated, culturally adapted DAs across institutions, regardless of size or geographic location, could reduce variation in practice and promote patient empowerment. Investments in education and awareness campaigns targeted at both clinicians and patients may also facilitate a shift in attitudes and organizational culture, fostering greater acceptance and normalization of SDM across the care continuum.
Contribution to the Literature
To our knowledge, this is the first survey extensively investigating clinician attitudes towards SDM and the uptake of DAs in the field of BC at the European level. Previous studies had a narrower focus in terms of perspective of analysis and geographical scope. A survey by Maes-Carballo et al (2021) only investigated the knowledge, awareness and attitude towards SDM amongst Spanish-speaking clinicians from Spain and Argentina, 33 not covering the use of DAs. A recently published study using focus group methodology investigated Portuguese general practitioners’ awareness and perception of PDAs. 34 Other published surveys investigated the level of SDM from the perspective of BC patients, as is the case of a German cross-sectional study in which BC patients who underwent surgery evaluated SDM using Shared Decision Making Questionnaire (SDM-Q-9).35,36
By revealing that the use of DAs with female BC patients might be influenced by the gender of treating physicians, this work also contributes to a growing body of literature that examines the impact of patient-clinician gender-concordance on patient outcomes. 13 A previous study showed that gender affects the relation between specific nonverbal behaviors and satisfaction, concluding that, for female physicians, the latter was related to female gender stereotypical nonverbal behavior (eg, more gazing at patient, less interpersonal distance, softer voice, less looking at medical chart). 37 Furthermore, for female physician–female patient consultations, doctor interruptions were positively related to patient satisfaction, whereas in male physician–male patient consultations interruptions worsened satisfaction levels. 38 A recent analysis of more than 20 000 US adult respondents to the 2018 and 2020 Medical Expenditure Panel Survey found that women who saw a female usual clinician were 6 – 9 percentage points more likely to be up-to-date with influenza, pneumococcal and shingles vaccination as well as breast, cervical and colorectal cancer screening; the same sex-concordance pattern was not observed among male patients, hinting at gender-specific mechanisms according to which females with female physician have a higher likelihood to adhere to preventive services guidelines. 39 However, the underlying factors explaining why patient-provider concordance might impact on patient experience and outcomes have been less extensively explored in the literature. In this area, another recent mixed-methods study investigated how patient-clinician gender concordance relates to trust, concluding that gender concordance showed no consistent effect, with participants often indicating that rapport, communication style and feeling respected mattered more than sharing the clinician’s gender. 40 Building on these qualitative insights. The statistically significant gender differences observed in our survey study with respect to SDM, namely the use of DA to explain clinical contents or the stronger tendency to involve caregivers, contributed to shed some light in this regard, offering concrete behavioral pathways through which gender concordance may shape patient experience and outcomes.
Limitations
This study comes with limitations. The overall number of responses collected is relatively small. Furthermore, some countries were only sporadically represented in the survey, and the category “Other countries” grouped together a heterogeneous mix of contexts, further limiting the granularity of country-level interpretation. This affects the representativeness of the findings across all European BC centers. However, the results of this survey were treated descriptively and interpreted with an exploratory approach, and should therefore be considered as indicative rather than definitive. Additionally, online surveys are susceptible to selection bias, as certain population subgroups may be difficult to reach (eg, older respondents). 41 Social desirability bias can influence survey scores, as respondents may answer questions based on what is socially expected rather than their true attitudes toward patient-physician relationship style and SDM. To minimize the impact of these biases, the study purpose was disclosed, and anonymity of the responses was ensured. 42 The survey was administered in English, which could have posed a challenge for respondents from different nationalities and backgrounds in accurately interpreting the survey questions. To mitigate the risk of collecting inconsistent responses, a cross-country cognitive testing exercise was carried out to validate the survey structure and items. Lastly, this survey illustrates self-reported perceptions from the clinicians’ perspective, and it is not informative of the actual diffusion of DAs in Europe. The results do not reflect the specificities of any country nor of the underlying health systems, and as such should be interpreted only as exploratory and with caution. Nonetheless, the study contributes valuable insights into shared decision making in Europe, a topic that remains relatively underexplored.
Conclusions
Patient-centricity calls for accurate consideration and reflection of patients’ values, preferences and choices at every step in the treatment pathway. The progress in BC care has revived interest in SDM, given to a broad spectrum of alternative therapeutic options available to patients, and the potential for better patient outcomes and improved quality of care arising from treatment plans aligned with patient values. Published literature suggests that participatory approaches and the use of DAs to support treatment decisions have been more extensively studied and implemented in North America. Nonetheless, the level of interest in SDM demonstrated by the BC specialists in this study points to a promising outlook for the continued advancement of SDM practices in Europe. Future research should investigate patient-perspective studies, prioritizing the efforts towards implementation trials evaluating the real-world effectiveness of DAs. 43 Notably, there are promising ongoing initiatives in this regard, like the EU-funded CINDERELLA project that is assessing the impact of an AI platform to support SDM in locoregional breast cancer treatment.44,45 Future work should therefore clarify which factors can lead to the sustained adoption of SDM practices and DAs in clinical settings, with particular attention to barriers and facilitators linked individual characteristics – including physician gender-related differences and patient-clinician gender-concordance, which may shape communication styles, decision-making dynamics, and openness to shared decision-making, as observed in this study – so as to move toward increasingly patient-centric healthcare systems.
Supplemental Material
Supplemental material - Evidence on Patient Decision Aids and Shared Decision-Making across Breast Centers in Europe: A Cross-Sectional Survey Study
Supplemental material for Evidence on Patient Decision Aids and Shared Decision-Making across Breast Centers in Europe: A Cross-Sectional Survey Study by Vittoria Ardito, MSc, Natalia Oprea, PhD, Oriana Ciani, PhD in Cancer Control.
Footnotes
Acknowledgements
The author would like to thank the networks of breast cancer professionals involved in disseminating this survey.
Ethical Considerations
The authors confirm that all methods were performed in accordance with the relevant guidelines and regulations. In November 2021, the Ethical Committee of Bocconi University (Milan, Italy) approved the survey protocol (FA000375).
Consent to Participate
All survey participants signed informed consent and agreed to the publication of the study results.
Authors contribution
Funding
This study was conducted as part of the ShareView project, “Supporting shared decision-making and communication in metastatic breast cancer”, funded by Pfizer Global Medical Grants in partnership with Sharing Progress in Cancer Care (SPCC), and the CINDERELLA project, which was funded by the European Union (EU grant HORIZON-HLTH-2021-DISEASE-04. Project number 101057389). The funder did not have a role in study design, data collection and analysis, decision to publish, or preparation of this manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Survey data will be made available upon request to the corresponding author.
Supplemental Material
Supplemental material is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.