
Abstract
Background
The importance of D-dimers (DD) assessment in the diagnostic algorithm of venous thromboembolic (VTE) disease is well known. Increase of DD concentration may be also associated with neoplastic disease. Many studies documented that high concentration of DD before solid tumour surgery indicates more advanced disease and poor life expectancy. The prognostic value of the DD concentration variability in the perioperative period, in women undergoing breast cancer surgery, has not been analysed so far. Thus, the aim of the present prospective study was to assess whether the trend of DD concentration changes in the perioperative period may predict cancer recurrence in women undergoing breast cancer surgery.
Materials and methods
189 consecutive women with histopathological diagnosis of breast cancer (BC) referred for surgical treatment were included. DD concentration was measured twice in each patient: at the time of admission to hospital and at the time of discharge home. Enoxaparin in standard dose of 40 mg daily s. c. was used as primary VTE prophylaxis in all of the patients.
Results
The recurrence of BC, within 1 year observation time, occurred in 13 patients (6.8%), in 11 (5.8%) patients with DD increase after surgery and only in 2 (1.1%) without an increase in DD, P = .0179. Increase in DD concentration after BC surgery was an independent positive predictor of disease relapse (OR 8.600, LCI 1.451, UCI 96.80, P = .0371) together with the lack of postoperative radiotherapy (OR 6.009, LCI 1.305, UCI 31.95, P = .0245), whereas the lack of postoperative chemotherapy predicted no BC relapse (OR .07355, LCI .0056, UCI .58, P = .0245).
Conclusions
Increase of DD in the early postoperative period may be considered as additional independent predictor of recurrence of BC within 1 year.
Keywords
Introduction
Despite advances in diagnostic technologies and treatment modalities, neoplastic diseases are still the major health threat all over the world. 1 Breast cancer (BC) is the most frequently recognised neoplastic disease in women, with an estimated 2.3 million new cases diagnosed annually. 2 The number of BC diagnosed worldwide has been increasing at an alarming rate in the last decades. 3 Thus, many efforts are made to detect cancer cells or their products on molecular level, and especially, to find the molecular and/or biological predictors of treatment relapse and worse survival.
D-dimers (DD) are the degradation products of cross-linked fibrin. In healthy people, DD are present in plasma only in trace amounts. The importance of DD in the venous thromboembolic disease (VTE) diagnostic algorithm is well known. 4 DD are a key factor in the assessment of pre-test probability in the diagnostics of VTE. 4 Concentration below the cut-off point excludes thromboembolic complications in low or intermediate clinical probability group. 4 It is worth to note that the increase in DD concentration may be also associated with neoplastic disease, vasculitis, as well as other inflammatory diseases.5,6 Moreover, elevated DD levels are reportedly associated with higher risk of mortality. 6
Several studies confirmed an association between DD and tumour stage, lymph node involvement, and overall survival in patients with solid tumours, such as lung cancer, breast cancer, oesophageal cancer, gastric cancer, colon cancer and gynaecological malignancies.7-12 Markedly increased plasma DD levels indicated advanced stage of disease and poor clinical outcome in cancer patients.13-17 Diao et al. showed that increased plasma DD was predictive of asymptomatic blood born metastasis in gastric cancer patients. 18
Much less information concerned the role of DD variability at the time of surgical treatment of neoplastic disease. Perioperative DD variability in women undergoing BC surgery has not been analysed so far. Identification of the group at high risk of recurrent breast cancer may contribute to the development of better treatment strategies in this group of patients.
The aim of the present prospective study was to assess whether the variability of DD concentration in the perioperative period may predict cancer recurrence in women undergoing BC surgery.
Materials and Methods
The study was conducted between June 2016 and November 2020 in accordance with the protocol approved on 11 May 2016 by the Bioethics Committee at National Tuberculosis and Lung Diseases Research Institute in Warsaw (signature KB-12/2016). All patients gave their written informed consent to participate in the study. The reporting of this study conforms to STROBE guideline. 19
Consecutive female patients with histologically confirmed BC, referred for surgical treatment in the Oncological Surgery Department, Masovian Cancer Hospital in Wieliszew in Poland, were included. Depending on the clinical TNM classification (eighth edition), patients were qualified for surgery or neoadjuvant chemotherapy followed by surgery. The eligibility criteria for surgery were the following stages: 0 (TisN0), IA (T1N0) and IIA (T2N0 luminal A or luminal B HER 2 negative). Patients diagnosed with higher stages were first qualified for neoadjuvant chemotherapy (NACT).
The criteria of exclusion from the study were the presence of distant metastases (stage IV) and the use of anticoagulant therapy before hospital admission.
All the patients were operated on by the same surgeon, according to the same protocol of surgical treatment. The extent of the operation depended mainly on the local and locoregional stage of disease.
Four types of surgery were performed: 1. Breast Conserving Treatment (BCT) with sentinel lymph node procedure (SLN) 2. Mastectomy (MS) with sentinel lymph node procedure (SLN) 3. Breast Conserving Treatment (BCT) with axillary lymph node dissection (ALND) 4. Modified Radical Mastectomy (MRM)
In patients with stage T1-T2N0, the preferred treatment option was BCT with SLN. An alternative option was MS with SLN In the absence of contraindications to the breast conserving treatment, the final choice was made by the patient after a detailed discussion of both types of treatment.
Patients in the T1-T2N1 stage were qualified for surgery after NACT. In this group, lymphadenectomy was always performed, while the scope of breast surgery included BCT or MS, as described above.
In the T3-T4N1 stage, patients were qualified for MRM preceded by NACT.
NACT was applied according to the current recommendations. 20 Patients who received NACT had biopsy-confirmed metastases to axillary lymph nodes (N1) or tumours larger than 5 cm in diameter (T3) in imaging tests (ultrasonography or mammography) or the triple-negative breast cancer (no expression of oestrogen, progesterone and herceptin 2 receptors in immunohistochemical staining) and the tumour diameter larger than 2 cm (T2). The NACT regimen depended on the molecular subtype of the cancer and the clinical condition of the patient. Surgery was performed within 2–3 weeks after the completion of NACT in all of the patients.
Postoperative treatment (radiotherapy and adjuvant chemotherapy) was conducted in accordance with the current recommendations. 20 Adjuvant chemotherapy was used in case of HER2-positive, triple-negative breast cancer and the presence of metastases in the axillary lymph nodes. Patients after BCT procedure or with ≥4 metastases to the axillary lymph nodes were qualified to postoperative radiotherapy. All patients diagnosed with BC containing oestrogen receptors were treated by hormones therapy.
Ultrasound examination (US) of the proximal deep veins of the lower limbs was performed in all of the patients twice: at admission and before the discharge from the hospital. The US was performed with the E-CUBE 11 apparatus from Alpinion Medical Systems Co with the use of a linear probe operating at a frequency of 5–10 MHz in the real-time B presentation. US compression test of the proximal deep veins of the lower limbs was performed according to generally accepted principles. 21 The criterion for the diagnosis of venous thrombosis was a positive compression test result, which meant the absence or incomplete collapse of the examined vein under compression with the transducer. The negative compression test result excluded the presence of thrombosis.
DD concentration was measured twice in each patient: at the time of admission to the hospital and at the time of discharge home. The concentration of DD was determined in plasma using COBAS INTEGRA 400 analyser with the Tina-quant D-dimer Gen.2 reagent. The increase of DD concentration was defined as an increase by 5% or more, related to the baseline concentration, the other results were defined as ‘no increase’. Enoxaparin in the dose of 40 mg s. c. was used as an antithrombotic prophylaxis during the entire hospitalisation in all of the patients.
As recommended, the patients reported for postoperative follow-up visits every 3 months for at least 1 year. The aim of such visits was the detection of local recurrence, locoregional recurrence or distant metastases.
Statistical Analysis
Statistical analyses were performed using Statistica v.9. The data were presented as means (+/− SD), medians, and ranges, and the relationships between the qualitative and quantitative variables were investigated. The statistical significance of these relationships was checked using the Chi-square test, V-square test, Wilcoxon test, Kruskal–Wallis test and Mann–Whitney test. The progression-free survival was assessed using Kaplan–Meier survival curves. It was assumed that the level of significance indicating statistically significant results was P < .05.
Results
189 women, median age 55 years (range 29–86 years), were enrolled into the study.
Characteristics of Study Patients.

Deep vein thrombosis (DVT) was not found in any of the study patients, neither on admission nor on the day of discharge.
Median DD Concentration by Locoregional Stage (pTNM) and NACT Use.

Baseline and postsurgical DD concentrations were significantly higher in NACT (+) patients, comparing to NACT (−). Postsurgical DD concentration was significantly higher in stage III comparing to stage 0–I and II.
Median DD Concentrations According to the Type of Surgery Performed.

In the group of patients who underwent the sentinel node procedure (BCT + SLN or MS + SLN), the median concentration of DD before and after surgery was significantly lower than the concentration of DD in the group of patients whose scope of surgery included removal of all axillary nodes (BCT + ALND or MRM).
In 98 patients (52%), an increase in DD concentration after surgery was observed (group 1), and in 91 patients (48%), no increase in the concentration of DD was noted (group 2). The median concentrations of DD before and after operation were as follows: group 1 were 292.37 and 426.15 μg/L and group 2 were 443.17 and 339.00 μg/L. The median increase and decrease in DD concentrations were: 94.78 μg/L (range: 6–1532.58 μg/L), and 98.00 μg/L (range: 2.85–2157 μg/L), respectively.
Trends of DD Change According to Preoperative NACT Use and pTNM Stage.

The percentages of patients qualified for NACT in the groups with an increase and a decrease in D-dimer concentration after surgery were similar, and no significant differences in DD trend were found between patients with different pTNM stages.
During the follow-up (median of 35 months), 13 patients (6.8%) were diagnosed with cancer recurrence. One patient experienced a local recurrence, two in regional lymph nodes, and in the remaining patients, distant metastases were diagnosed: to the bone in 6 patients, to the liver in 2 patients, simultaneously to the liver and bone in 1 patient and to the brain in 1 patient. Among patients with an increase in DD concentration after surgery, subsequent cancer recurrence was noted in 11 individuals (11.0% CI [6.2–18.5]%). Among patients without an increase in DD concentration after surgery, subsequent cancer recurrence was noted only in 2 cases (2.2% CI [.6–8.5]%) (P = .0179).
Factors Predicting Relapse After BC Surgery (Multiple Regression Analysis).
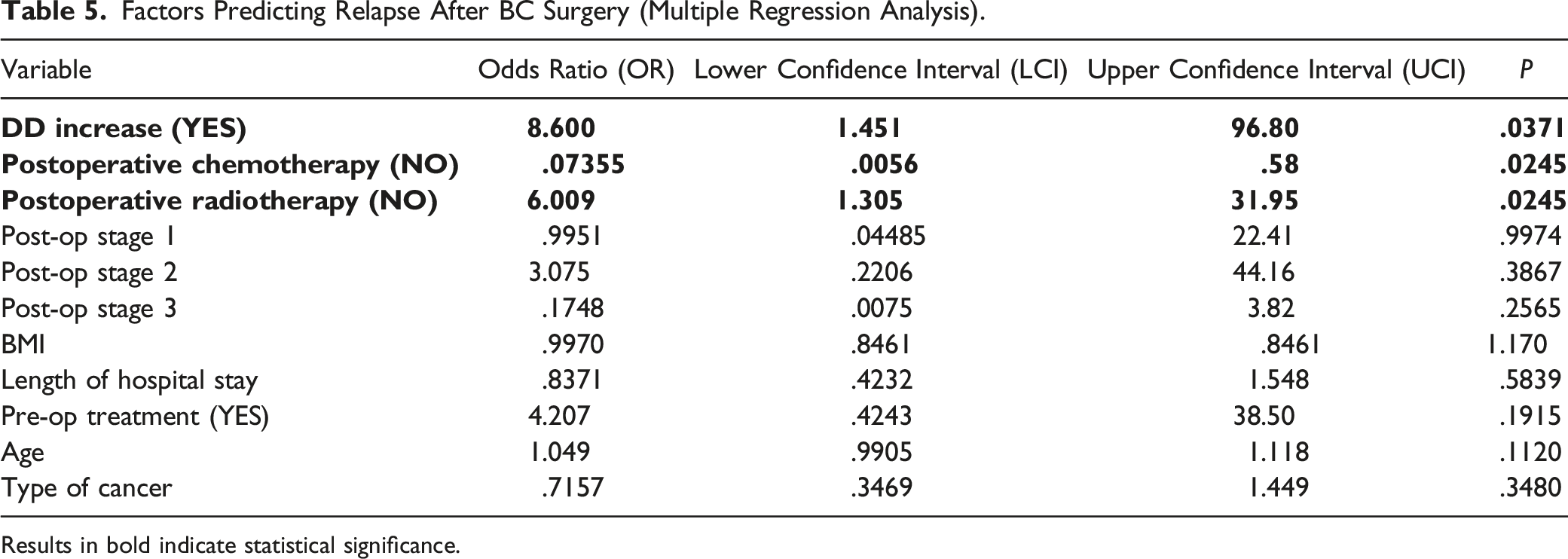
Results in bold indicate statistical significance.
Kaplan–Meier analysis of progression-free survival (PFS) showed a significantly shorter PFS in patients with DD concentration increase (P = .026, Figure 1) and stage III disease (P < .0001, Figure 2). Additionally, shorter PFS was observed in those who did not receive postoperative radiotherapy (P = .0006, Figure 3) and in those who received postoperative chemotherapy (P = .0211, Figure 4). Median survival was not reached in any of the groups. Kaplan–Meier analysis of progression-free survival related to trend of DD concentration, P = .026. Kaplan–Meier analysis of progression-free survival related to postoperative disease stage, P < .0001. Kaplan–Meier analysis of progression-free survival related to postoperative radiotherapy, P = .0006. Kaplan–Meier analysis of progression-free survival related to postoperative chemotherapy, P = .0211.



Discussion
Over the past 20 years, numerous studies have been published assessing the prognostic value of D-dimers in cancer patients. Most studies concerned patients who received surgical treatment due to various solid tumours, such as non-small cell lung cancer, colorectal cancer, gastric cancer, oesophageal cancer, pancreatic cancer, renal cancer and also in breast cancer.7,8,10,13,22-34 The majority of publications showed that increased preoperative concentration of DD was associated with reduced overall survival and progression-free survival.34-37
Negative prognostic significance of DD was also documented in non-surgical population of cancer patients. A Korean study analysed overall survival in patients with disseminated gastric cancer, enrolled in palliative chemotherapy, in relation to the pre-treatment DD concentration. Median survival of patients with lower DD concentrations (<1.5 μg/mL) was 22 months, while median survival of those with higher values (≥1.5 μg/mL) was 7.9 months (P = .019). 37
The present study group concerned consecutive patients with loco-regional breast cancer diagnosis. All the patients underwent surgical treatment in accordance with current guidelines. All of them received thromboprophylaxis with enoxaparin 40 mg sc during their hospital stay. It is worth emphasising the very high effectiveness of thromboprophylaxis in patients treated surgically due to breast cancer, as none of our patients developed postoperative DVT. Thus, DVT was excluded as a cause of elevated DD concentration before surgical treatment as well its subsequent increase in postoperative period.
Preoperative DD was significantly higher in patients who received NACT comparing to those who did not receive it. This finding illustrates the possible influence of NACT itself on DD level, but it should be emphasised that the NACT group was heterogeneous, and the higher concentration of DD could also be caused by the presence of metastases to lymph nodes in this group.
Postoperative DD was significantly higher in pathological stage III patients comparing to stage 0–II and significantly higher in patients who underwent MRM comparing to other types of surgery.
There was no statistically significant difference in median baseline DD concentrations between the groups with various pTNM stages. Lack of correlation between baseline DD concentration and pathological tumour stage, in the present study, was probably caused by the fact that only patients with locoregional disease were included, and that in those with higher locoregional stage, who were treated with NACT, DD was not assessed before chemotherapy.
Other authors have demonstrated a correlation between lymph node involvement and preoperative DD concentrations in BC patients. In a retrospective study, Halugodu et al showed that in breast cancer, preoperative plasma DD levels indicated advanced stage of disease, lymph node involvement and lymphovascular invasion. There was no significant relationship with tumour size and histopathological grade of tumour. 2
In a small prospective study of 70 patients (35 diagnosed with breast cancer and 35 with benign breast disease), Ghadhban et al showed that baseline DD level was normal (<.25) mg/l in 97.1% of patients with benign breast disease, but it was elevated in 88.6% of breast cancer patients. DD concentration was correlated with tumour size and grade, lympho-vascular invasion, and lymph nodes involvement. The authors concluded that increased plasma DD was a bad prognostic factor in breast carcinoma especially in advanced breast carcinoma where it indicated lympho-vascular invasion and metastasis. 38 Blackwell et al 39 also documented that plasma preoperative DD level was a marker of lympho-vascular invasion, clinical stage and lymph node involvement in operable breast cancer. Nevertheless, Fregoni et al 40 and Kacan et al 34 have not found significant correlation between lymph node involvement and DD levels. Moreover, Kacan et al 34 found no relationship between DD levels and locoregional relapse. Giaccherini et al showed in prospective clinical and laboratory data from the HYPERCAN study in 701 resected breast cancer patients that pre-chemotherapy DD levels were significantly associated with tumour size and lymph node metastasis. 41
In the literature, there is much less data evaluating the usefulness of DD assessment in the postoperative period. 42 Hara et al showed that a high D-dimer level on postoperative day 7 could predict tumour recurrence and reduced life-expectancy in patients with advanced gastric cancer, treated with gastrectomy. In this retrospective study, due to high postoperative DD concentration, the cut-off DD value of 4900 μg/L was identified as an independent predictive factor for both the overall survival and relapse-free survival. 42
To the best of our knowledge, our study is probably the first that evaluated a predictive value of the trend of D-dimer concentration in women undergoing breast cancer surgery.
In the group of patients with an increase in DD concentration after surgery, cancer recurrences were significantly more frequent than in the remaining patients (5.8% and 1.1%, respectively, P = .0179).
In patients with postsurgical DD increase, the risk of breast cancer relapse was 8.6-fold higher comparing to those patients in whom DD concentration lowered. Thus, we suspect that the trend of DD changes after surgery is more predictive of early relapse than the absolute DD values. DD increase was an independent significant predictor of cancer relapse within 1 year.
It seems that the removal of lymph nodes affected by cancer may have a greater impact on the concentration of DD after surgery than the extent of breast surgery. The involvement of axillary lymph nodes in patients with breast cancer was associated with higher concentrations of DD before surgery (probably due to NACT use), which in turn could directly affect their greater decrease after surgery.
Our data show that among 13 cases of early recurrence, in 4 cases, low stage of disease was diagnosed, and in 9 cases, no indications for NACT were found.
The lack of postoperative chemotherapy was a positive predictor of relapse-free 1 year survival in the multiple regression analysis.
Postoperative radiotherapy is an essential element of breast-conserving treatment (BCT + SLN and BCT + ALND). The indication for radiotherapy after mastectomy is the presence of metastases in more than 4 axillary nodes. The increased recurrence rate in patients not undergoing radiotherapy prompts consideration of qualification for radiotherapy in less advanced cases; however, the presented group is not numerous, and the conclusions require further multicenter studies.
Similarly, whether an increase in DD after surgery is a negative prognostic factor, independent of other prognostic factors (such as more advanced stages of pTNM, lack of postoperative radiotherapy), remains to be explored in large clinical studies.
Our study has several limitations: 1. The study was performed in 1 centre. 2. Relatively small number of patients was included. 3. No sample size calculations or justifications were made in this study. 4. Low number of patients were diagnosed with cancer relapse, due to relatively short postsurgical follow up, according to study protocol.
Conclusions
Increase of DD levels after operation in women treated surgically for breast cancer may be an independent, easy to assess and low-cost marker for prediction of early recurrences of breast cancer. Large scale investigations are necessary to confirm its clinical relevance in further practice.
Footnotes
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; they have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.