
Abstract
Introduction
This study examined the roles of hematologists and other professionals in providing decision support to patients with relapsed or refractory leukemia and lymphoma.
Methods
This was a qualitative study using in-depth semi-structured interviews involving 11 hematologists in Japan.
Result
We identified 7 categories related to the roles of hematologists in providing direct decision support to patients: (1) preparing patients before informed consent, (2) selecting the information to convey, (3) choosing a method for conveying this information, (4) respecting the intentions of patients and their families, (5) directing decision-making and considering fairness, (6) considering the emotional aspects of patients and their families, and (7) providing support after discussing treatment options. We also identified the following 5 subcategories related to the roles of hematologists in multidisciplinary collaboration: (1) communicating with other professionals, (2) gathering information from them, (3) providing information to them, (4) managing the entire medical team, and (5) encouraging nurses to actively participate with patients throughout the decision-making process.
Conclusion
Through content analysis, the hematologist’s direct role in decision-making was extracted as preparation and consideration in situations where information about decision-making is communicated, and emotional support after the information is communicated. In addition, active participation in discussions, sharing information about the patient’s situation and relevant discussions, and emotional support as the hematologist’s expected roles in other professions were extracted. The results therefore suggest that a multidisciplinary team is needed to share information and provide multidimensional support to patients.
Introduction
The prognosis and illness trajectory of leukemia and lymphoma vary greatly depending on the degree of progression and subtype of the disease. However, irrespective of the illness trajectory, patients face the same issues and debates related to decision-making, such as how far to go with aggressive treatment during the relapse or treatment-resistant period and the choice of treatment and place of care.1-3 Even in relapse cases, such patients may have the option to receive high-dose chemotherapy treatments or hematopoietic cell transplantations aimed at remission and achieving long-term survival. Such treatment carries significant risks, including complications such as severe infections and bleeding due to bone marrow suppression and treatment-related death, and may result in transition from invasive treatment aimed at cure to end-of-life (EOL). Even when the disease is refractory to treatment, anticancer therapy aimed at disease control is often administered until the end of life. In such contexts, it is very difficult for patients and their families to make decisions about these complex treatment strategies and the high risks involved in the context of their own life values.4-6
The American Society of Clinical Oncology (ASCO) has published consensus guidelines for clinician-patient communication, specifically recommending that clinicians provide information that is congruent with their patients’ interests and intentions while jointly considering their goals for treatment. 7 It is also notable that hematologists’ communication skills have been receiving increasing attention in hematology clinical practice in recent years. An ethnographic study of hematologists' communication patterns when communicating bad news revealed 4 characteristics: (1) technical-defensive patterns, (2) an authoritative pattern, (3) a relational-recursive pattern, and (4) a compassionate sharing pattern, and the paper also suggested that hematologists were not good at expressing caring and empathy. 8 In contrast, a qualitative study examining the needs of patients with hematological malignancies when being told bad news reported identifying emotional support from their healthcare providers and information needs about future support systems. It was also noted that healthcare-team involvement is necessary to meet these patients' needs and support their decision-making. 9
Therefore, this study sought to clarify the following: (a) the way in which hematologists perceive the roles of doctors in providing decision-making support to patients suffering from relapsed and refractory leukemia as well as lymphoma, (b) the expected roles of hematologists in supporting decision-making via multidisciplinary collaboration, and (c) the roles hematologists expect other healthcare providers to fulfill.
Methods
The purpose of this study was to determine hematologists’ role in decision support for patients with leukemia and lymphoma. Physicians at institutions with hematology wards and hematology outpatient clinics where chemotherapy and bone marrow transplantation are performed were included. The eligibility criteria for physicians included being Board Certified Hematologists and having at least 5 years of experience. Hematologists meeting these criteria were considered to have experience seeing patients with relapsed or refractory leukemia or lymphoma. Subjects were selected using opportunistic sampling, which is used in selecting those with common characteristics and the potential to provide a rich, appropriate, and diverse research agenda. Eligible physicians were asked to recommend a qualified physician who met the inclusion criteria to the head of the hematology department of a hospital in Tokyo. The recommended physicians were informed orally and in writing about the purpose and methods of the study and the voluntary participation clause. Although this is a qualitative study and it is difficult to theoretically calculate the sample size, we chose a sample size of 10 to 15 participants based on previous studies9-11 using the same content analysis method as in this study. The acceptance rate of recommended physicians was 100%.
Verbal and written explanations of the research objectives and procedures were provided to all participants, and written consent was obtained. This study was approved by the Institutional Review Board of University of Tokyo (Approval No. 3443). The study was initiated at the University of Tokyo and completed at Kyoto University.
To collect the data, we conducted in-depth interviews to identify the attributes and roles of doctors as well as the expected roles of nurses in providing decision-making support to patients with relapsed or refractory leukemia and lymphoma. Specifically, we scheduled face-to-face semi-structured interviews in private rooms between August and December 2011. All the interviews conducted were audio recorded and fully transcribed by 1 researcher (a research nurse), who also took detailed field notes during each interview. Physicians were first asked for their demographic details, including age, the type of facility where they worked, and the number of years they had worked in their area of specialization. We then asked them about their roles in treating patients suffering from relapsed or refractory leukemia and lymphoma.
To analyze the data, interview data were transcribed verbatim from the audio recordings. Interview data were then numbered for each participant, separated from personal information, and anonymized. A content analysis was then conducted. First, 1 researcher extracted all statements related to the 3 study topics from each transcript (eg, the role of hematologists, the role of hematologists in multidisciplinary collaboration, and the expectations of other professionals in the context of providing decision-making support). We then carefully conceptualized the text and categorized it into content areas through content analysis using the Klaus Krippendorff 12 method. The units, codes, and categories were decided through consensus. Next, another experienced qualitative researcher read the original interviews and classified them into categories and subcategories. The coder read the original interview text and independently determined the subcategory into which the content fell. The rate of agreement between the researchers and coders was 91%. Finally, the coder and the researcher discussed the units they disagreed on until they reached a consensus.
Results
Participant Characteristics
Characteristics of doctors and interview details.

∗Mean(Range).
The Role of Hematologists in Direct Decision Support
Role of hematologists in providing direct decision support (n = 11).

*1IC = informed consent; *2PHS = Personal Handyphone System (A phone used by doctors to communicate with staff in the hospital).
Preparing Patients Before Informed Consent (IC)
This category comprised 4 subcategories. Several participants talked about preparing patients and families for IC discussions, including “Gathering preliminary information for explaining issues to patients” and “Encouraging family members to participate in decision-making.” As such, physicians were expected to prepare patients before IC discussions. For instance, they would provide patients with information regarding the risk of relapse.
Selecting the Information To Convey
This category comprised 3 subcategories. In subcategory (1) “Choice of information to provide to patients,” more than half of the participants said that they did not provide their patients with prognoses. More importantly, more than half said they may not even tell their patients the truth, depending on the severity of the illness, to avoid a loss of hope; they were very selective about the information they chose to provide to their patients.
In subcategory (2) “Providing patients and families with information to help them make treatment decisions,” more than half of the participants identified “Communicating the advantages and disadvantages of treatment options” and “Telling patients and their families the information they need to make treatment decisions.” They provided information they believed would help patients and their families fully understand all the options before making a final decision.
In subcategory (3), “Providing patients and families with information to help them understand the patients’ current situation,” a large number said they would inform family members about the possibility of sudden changes and specific prognoses, with more than half saying they would explain the issues so that patients could visualize what may happen to them in the future. Generally, participants provided information to help patients and their families clearly understand their current situations.
Choosing the Way In Which To Communicate Information
This category comprised 2 subcategories. Nearly half of participants expressed the ideas of “I determine what I say and how I say it based on our long-standing relationship with the patients” and “Providing information based on the patient’s reaction and acceptance of their medical condition.” They carefully considered what they discussed and how they discussed it, especially considering their long-standing association with their patients. In this regard, they conveyed information based on how they thought patients would react and their level of acceptance. They also provided explanations according to what they believed patients intended and thought depending on their respective stages of readiness. Moreover, nearly half said that they would explain issues without using jargon, thereby ensuring that the information provided was easy to understand. Essentially, participants remained cognizant of the need to communicate both correctly and appropriately with patients and their families.
Respect for The Intentions Of Patients And Families
This category comprised 2 subcategories. In subcategory (1) “Respect for the will of patients and families,” more than half of the participants said they helped patients and families make decisions by supporting and respecting their wishes and desired treatments. In subcategory (2) “Setting goals in accordance with the preferences of the patients and families,” several participants said that they helped patients and families set feasible goals after listening to their wishes.
Directing decision-making and considering fairness
This category comprised 2 subcategories. In subcategory (1) “Considering the direction and fairness of treatment options recommended by doctors,” more than half of the participants said they explain treatment options with some direction while also providing options they find most beneficial. They talked about giving weight to treatment options and facilitating the decision-making process. Furthermore, they attempted to present information in a fair manner, being aware that the way they talk can affect the way patients perceive their treatment, as shown in subcategory (2).
Considering the Emotional Aspects Of The Patient And Family
This category comprised 3 subcategories. In subcategory (1)“explaining with consideration for emotions,” nearly half of the participants said they would attempt to instill hope among patients, and hence, provide explanations considering the related emotional aspects. In subcategory (2) “showing a supportive attitude to the patient”, several participants also expressed adopting a supportive stance to reassure patients that they were not abandoning them or their families. In subcategory (3) “attitude when facing patients and their families”, several participants talked about the doctor’s attitude toward patients, such as speaking with patients and families as equals and looking them in the eye.
Providing support after discussing treatments
Several participants said they informed patients about bad news and future treatments, after which they provided emotional support in consideration of any emotional variabilities.
Role of Hematologists in Multidisciplinary Collaboration and Providing Decision Support
The role of hematologists in multidisciplinary collaboration and decision support (n = 11).
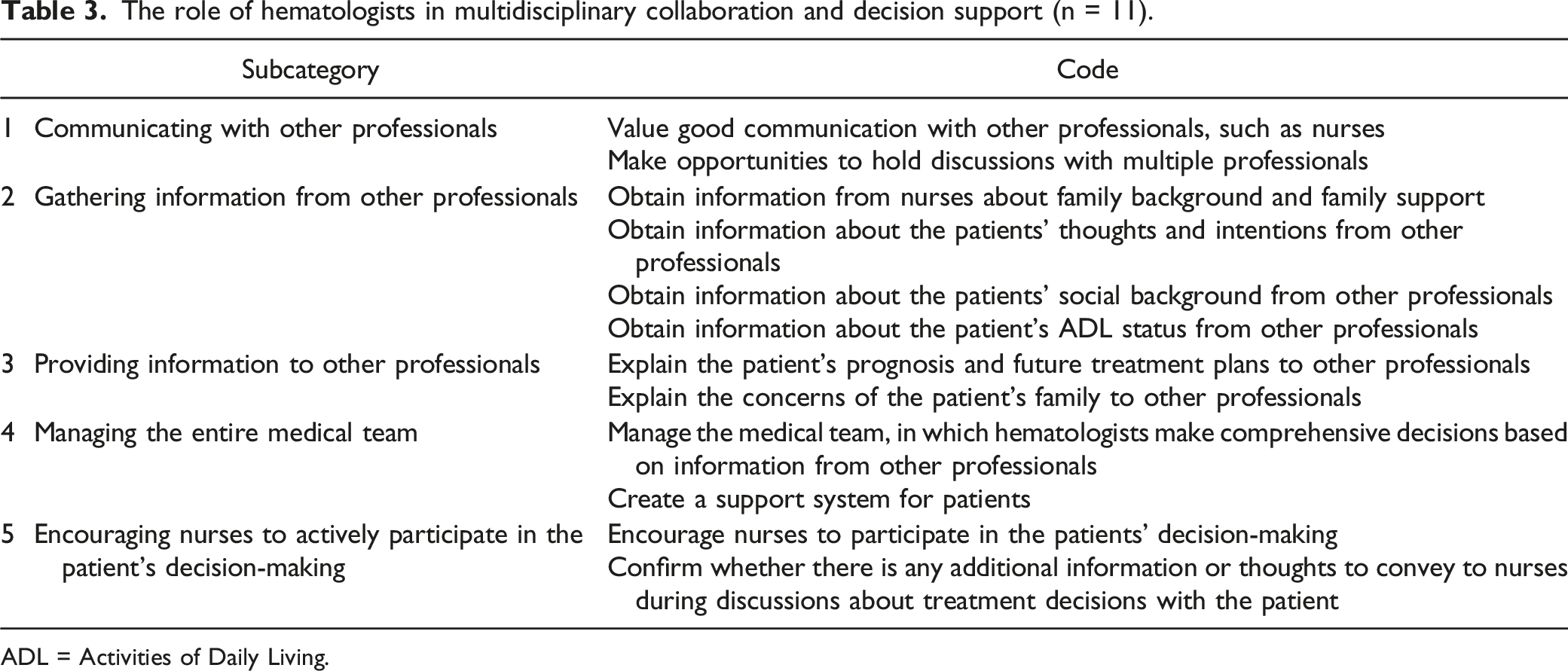
ADL = Activities of Daily Living.
Expected Roles of Other Professionals in Providing Decision Support
Expected roles of other professionals in decision support (n = 11).

Discussion
In this study, hematologists were interviewed to clarify their role and expectations of other professionals. The categories of hematologists’ direct role in decision-making were extracted, including preparation and consideration of the situation in which information about decision-making is communicated and emotional support after the information is communicated.
Hematologists presented treatment options based on a variety of factors, including the patient’s goals, emotions, the preparedness for the disease, and the severity of the disease. During this process, the hematologists worked with other professionals to understand specific information about the patient and family, including their background, goals, and intentions. They also said that they would decide what information to convey and carefully explain the treatment and medical condition, without using jargon, so that the patient and family could easily understand. ASCO guidelines recommend that physicians provide information that takes into account individual patient interests and preferences. 7 Although the present results are data obtained before these guidelines were developed, the hematologists who participated in this study were taking the actions recommended in the guidelines. The present results reveal more specific behaviors of hematologists with regard to what is recommended in the guidelines. For patients facing complex and risky treatment choices, it is important for hematologist to select information according to the patient’s wishes and to convey information in easy-to-understand terms.
Hematologists were expected other professionalsto pay attention to the emotional aspects of the patient and family to minimize their anxiety. In addition, they expected nurses and other professionals to listen to the patient and family’s wishes and thoughts about treatment, share them with the physician, and serve as emotional support for the patient and family. Moreover, hematologists were expected to understand the patient’s wishes and preferences, explain complex and difficult-to-understand treatments and medical conditions, and present options that were consistent with the patient’s wishes. ASCO guidelines also emphasize the need to form a rapport with patients and their families and to assess and support coping needs. 7 The hematologists who participated in this study wanted to implement this in collaboration with other professionals. The wishes and intentions of patients and their families change as the disease progresses or symptoms worsen. Therefore, it is thought that by having physicians and other professions work together to understand the wishes of patients/families at that time, decision-making support in accordance with the wishes of patients/families will become possible.
Leukemia and lymphoma may be treated through chemotherapy, even in cases of relapse and during the refractory phase. This makes it difficult to determine when to transition from curative treatments to those more focused on quality of life (QOL).13,14 Previous studies have reported that hematologists are reluctant to discuss EOL issues while primary disease treatments are still possible.15,16 A number of the hematologists who participated in the study had a variety of ways of explaining the prognosis to patients and their families. For example, in some cases, they informed the family about the possibility of a sudden change in prognosis, including specific figures, while in other cases, depending on the severity of the disease and the stage of life, they did not inform them of the prognosis at all or withheld the fact. Furthermore, more than half of the respondents stated that they would explain the treatment that they thought would be most beneficial to the patient.
A number of the hematologists who participated in this study also had a long history of working with patients to understand their individual backgrounds, and what they talked about and how they communicate, while also having a direction that the hematologists thought was suitable, and gave the patients some direction as they spoke. This suggested that hematologists attempt to tailor their decision-making support to the needs of their patients. On the other hand, hematologists infer patients' needs based on their previous experience, which runs the risk of making suggestions that are not in line with the patients’ original needs. Previous studies have reported that hematologic oncology patients take a passive role in the treatment decision-making process due to the complexity of their treatment and disease 17 and expect their physicians to take a paternalistic role. 16 When hematologists provide some treatment direction and paternalistic response to hematologic oncology patients with these characteristics, patients may not fully understand the advantages and disadvantages of treatment and may not make an informed choice. If treatment is responded to, the patient’s quality of life improves, but if treatment is not effective, the patient may die in the hospital during active treatment. In addition, patients may not be able to live the life they want, with increased risk of infection and prolonged hospitalization. 1 Hematologists need to have frank discussions with patients, keeping in mind the direction they think is best for the patient, and working with other professionals to understand the patient’s wishes.
Hematologists who participated in this study indicated that the role they expected of multidisciplinary professionals was to inform them about patient thoughts, information, and methods of care that the physicians were unaware of. They also expected other professions to play a role in providing emotional support to patients and their families. In a previous study of oncologists, including hematologists, lack of information about the patient was the most frequently cited factor hindering patient involvement in decision-making. 18 Physicians also recognized that having a third party present during decision-making discussions supported patient decision-making and facilitated involvement and reflection on treatment decisions. 18 In that previous study, physicians emphasized the importance of obtaining information about the patient and the presence of a third party in the decision-making situation, which was similar to the findings of the present study. This confirms the importance of a multidisciplinary approach to facilitate decision-making in accordance with the patient’s wishes. In making treatment decisions, it is necessary to organize information not only from a medical perspective, but also based on the patient’s priorities and values. Obtaining such information is difficult for hematologists alone, and multidisciplinary collaboration is important. By understanding the patient’s needs and organizing the information necessary for decision-making, it is expected that the discussion between the attending hematologist and the patient will be deepened. 9
Finally, it is important to note that the survey for this study was conducted in 2011 and there was not much collaboration with the palliative care team, 15 the participants in this study did not mention the role they expected to play regarding palliative care physicians. Recently, however, the effects of early palliative care have been reported in clinical hematologic oncology. A study evaluating the effects of early introduction of palliative care and continuous psychological support by a multidisciplinary team in patients with acute leukemia reported a reduction in symptoms due to acute stress reactions compared to the usual care group. 19 It has also been reported that patients undergoing hematopoietic stem cell transplantation who received regular twice-weekly visits by a palliative care physician had a higher QOL at 3 months of hospitalization compared to the group that received usual care. 20 In patients with leukemia and lymphoma, where the potential for rapid change is high, it is expected that hematologists and palliative care specialists will support patients and begin discussing long-term goals early, in case treatment goals suddenly change. 21
This study had some limitations. The first is that the data collection and analysis were conducted between 2011 and 2012. Therefore, because treatment outcomes for hematologic tumors have improved compared to a decade ago, the data cannot be directly applied to decision support for patients with such tumors and their families today. However, the patients with treatment-resistant hematologic tumors have not changed significantly in their characteristics or treatment environment,1,22 and it is significant to clarify the hematologist’s role in decision support. Second, the use of the opportunistic sampling makes it difficult to generalize the findings. In this study, we collected the opinions of hematologists at hospitals where hematologic oncology patients are mainly treated, such as cancer hospitals and university hospitals in Japan, and we believe that we were able to collect diverse opinions regarding the role of decision support as perceived by hematologists. Based on the present study, research is needed to clarify the decision support roles of other professionals who care for patients with leukemia and lymphoma, including nurses. This would make it possible to construct a model of shared decision-making support for hematologic oncology patients through multidisciplinary collaboration.
Supplemental Material
Supplemental Material - Qualitative Analysis of the Roles of Physicians and Nurses in Providing Decision Support to Patients With Relapsed or Refractory Leukemia and Lymphoma
Supplemental Material for Qualitative Analysis of the Roles of Physicians and Nurses in Providing Decision Support to Patients With Relapsed or Refractory Leukemia and Lymphoma by Miharu Morikawa, and Yuki Shirai in Cancer Control
Footnotes
Acknowledgments
The authors would like to thank Mizuki Takegata for her help in checking the coding. We would like to thank all of the hematologists who took part in the interviews who were willing to share their experiences of taking part in this study. We would also like to thank Professor Kiyoshi Miyagawa for his efforts in preparing this study. In addition, we thank Research Square for publishing this paper as a preprint. Qualitative analysis of the roles of physicians and nurses in providing decision support to patients with relapsed or refractory leukemia and malignant lymphoma | Research Square
Authors’ Contributions
Miharu Morikawa and Yuki Shirai contributed to the design and implementation of the research and to the analysis of the results. Miharu Morikawa wrote the article in consultation with Yuki Shirai.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the JSPS KAKENHI: Grant Numbers JP19H03932 and JP23792581.
Ethics Approval
This study was approved by the Institutional Review Board of University of Tokyo (Approval No. 3443). The study was initiated at the University of Tokyo and completed at Kyoto University.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.