
Abstract
Objectives
Head and neck mucosa-associated lymphoid tissue (MALT) lymphoma, a rare subtype of non-Hodgkin lymphoma, has received limited attention regarding its prognosis. This study aimed to illuminate the clinical characteristics and identify prognostic factors for head and neck MALT lymphoma, intending to develop an accessible tool for clinicians to predict long-term survival probabilities and inform therapeutic strategies.
Methods
This multicentre retrospective study enrolled 424 head and neck MALT lymphoma patients from the Surveillance, Epidemiology, and End Results Program (SEER) database. Least absolute shrinkage and selection operator (LASSO)-Cox regression analysis identified independent prognostic factors for overall survival (OS), leading to the development of an age-based nomogram predicting OS probabilities at 5, 10, and 15 years. Evaluation included time-dependent receiver operating curve (ROC), calibration curves, and decision curve analysis.
Results
Multivariate Cox analysis highlighted age exceeding 65 years [hazards ratio (HR): 2.97, 95% confidence interval (CI): 1.94-4.57; P < 0.001] and unmarried status (HR: 1.58, 95% CI: 1.07-2.33, P = 0.023) as significantly associated with shorter OS, while black race correlated with longer OS (HR: 0.25, 95% CI: 0.09-0.69, P = 0.007). The age-based nomogram, integrating these factors, demonstrated efficacy in predicting 5-year [area under the curve (AUC): 0.640] and 10-year OS (AUC: 0.705), with an impressive AUC of 0.842 for the 15-year OS probability in the training cohort. Decision curve analysis affirmed the nomogram’s clinical utility, surpassing individual factors. Consistent results were observed in validation cohorts.
Conclusion
Our study provides crucial insights into head and neck MALT lymphoma, filling gaps in understanding its clinical landscape. The validated age-based nomogram serves as a practical tool for clinicians, offering enhanced prognostic precision and guiding personalized treatment strategies in this understudied lymphoma subtype.
Introduction
Extranodal marginal zone lymphomas of mucosa-associated lymphoid tissue (MALT) constitute a rare hematological malignancy, often manifesting in diverse anatomical sites such as the gastrointestinal tract, ocular adnexa, lung, and salivary glands.1,2 The pathogenesis of MALT lymphoma is strongly associated with chronic antigenic stimulation, which may result from infections (e.g., Helicobacter pylori in gastric MALT lymphoma) or autoimmune disorders (e.g., Sjögren’s syndrome and Hashimoto’s thyroiditis).2-4 Genetic abnormalities, such as the t(11;18)(q21;q21) translocation, have also been implicated in its pathophysiology, driving constitutive activation of NF-κB signaling pathways and promoting lymphomagenesis.2,5 Compared to the aggressive nature of diffuse large B-cell lymphoma (DLBCL), MALT lymphoma is characterized by unique clinical features, histological morphology, and an indolent course. 2 While most individuals within a predominantly elderly patient population may anticipate an unaffected lifespan in the presence of this disease, the course of MALT lymphoma exhibits diversity, with mortality rates escalating in cases of transformation to large cell lymphoma (occurring in less than 5% of cases), early disease progression, or an inadequate response to therapy.6-10
Head and neck MALT lymphoma represents a distinct and clinically significant subtype, with increasing incidence and unique diagnostic and therapeutic challenges.11,12 This subtype can involve various anatomical sites, including the salivary glands, thyroid, ocular adnexa, and larynx, leading to diverse clinical presentations that often mimic benign conditions, such as chronic inflammation or infection. 13 Diagnosis typically requires histopathological examination, immunohistochemistry, and molecular studies to distinguish it from other lymphomas and reactive lymphoid hyperplasia. 14 Despite its indolent nature, head and neck MALT lymphoma is associated with a high rate of dissemination and disease recurrence,15-17underscoring the need for effective management strategies. Treatment of MALT lymphoma varies depending on the site and stage of the disease. Localized disease is often treated with radiotherapy or surgery, while advanced or disseminated cases may require systemic therapies, such as chemotherapy (and/or immunotherapy with anti-CD20 monoclonal antibodies). 14 However, there is limited consensus on the optimal treatment approach for head and neck MALT lymphoma. Notably, a study from a Chinese cohort reported no significant differences in survival outcomes between surgical intervention alone and combined chemoradiotherapy, 18 though the findings were limited by small sample sizes and lack of comprehensive prognostic factor analysis.
The rarity of head and neck MALT lymphoma, combined with its clinical heterogeneity, has resulted in a paucity of dedicated studies. This has hindered our understanding of its clinical characteristics, prognostic factors, and optimal management strategies. To address these gaps, we conducted a comprehensive investigation using the Surveillance, Epidemiology, and End Results (SEER) database, a robust resource maintained by the National Cancer Institute that covers approximately 34.6% of the U.S. population. 19 The SEER database provides a unique opportunity to study rare malignancies on a population-based scale, offering insights into epidemiology, treatment patterns, and outcomes. In this study, we aimed to identify key clinical and prognostic factors associated with head and neck MALT lymphoma and to develop a personalized prognostic tool to guide clinical decision-making. Specifically, we constructed an age-based nomogram to predict long-term overall survival (OS), leveraging the extensive SEER dataset. By providing a novel predictive model, this study not only enhances our ability to estimate survival outcomes but also contributes to the growing body of literature on this rare and challenging malignancy. Ultimately, our findings aim to support clinicians in optimizing patient care and advancing the understanding of head and neck MALT lymphoma.
Methods
Study Design and Data Acquisition
All patients for this extensive population-based retrospective study were sourced from the SEER database, with data extraction conducted using SEER*Stat 8.35. This study adhered to the principles outlined in the Declaration of Helsinki. The reporting of this study conforms to the transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD) guidelines. 20
Inclusion and Exclusion Criteria of Patients
Patients diagnosed with head and neck MALT between 1975 and 2016 were initially identified from the SEER database. Inclusion and exclusion criteria were as follows: 1) malignancies originating in specified locations, such as the nasal cavity, paranasal sinuses, lips, base of tongue, gums, and others; 2) tumors with the International Classification of Diseases (ICD) code O-3 morphology 9699/3; and 3) exclusion of patients lacking complete records for Ann-Arbor stage, treatment, OS, and other crucial clinical information.
Covariates
The initial set of variables was obtained from the SEER database, which encompasses an extensive range of demographic, clinical, and treatment-related characteristics. A total of nine variables were included in the analysis: age at diagnosis (≥65 or <65), gender (male or female), race (White, Black, or Other), marital status at diagnosis (married or other), primary tumor site (nasal cavity and sinus, pharynx and larynx, oropharynx, nasopharynx, or oral cavity), Ann-Arbor stage (Stage I, Stage II, or Stage III–IV), surgery status (yes or none), radiation status (yes or none/unknown), and chemotherapy status (yes or none/unknown).
Dataset Splitting and Variable Preprocessing
All eligible patients in the dataset were randomly divided into training and validation cohorts using a 7:3 ratio through the “createDataPartition” function in R software. The training cohort was utilized for developing a predictive signature, while the validation cohort was employed to validate its predictive ability and clinical utility. Categorical variables were presented as counts and percentages, with a Chi-square test comparing differences between the training and validation cohorts. Prior to the analysis, categorical variables were transformed using one-hot encoding to ensure compatibility with the regression model.
Model Development and Evaluation
To identify independent prognostic factors associated with OS, Least Absolute Shrinkage and Selection Operator (LASSO)-Cox regression analysis was performed using the glmnet package in R software. 21 The LASSO penalty (L1 regularization) was applied to shrink the coefficients of less important variables to exactly zero, retaining only the most relevant predictors. 4 The degree of shrinkage was controlled by the tuning parameter lambda (λ). To determine the optimal λ value, 10-fold cross-validation was performed using the cv.glmnet function. The optimal λ was selected based on the lambda.min criterion, which minimizes the mean cross-validated error. This approach balances model complexity with predictive performance, ensuring generalizability and robustness. Variables with non-zero coefficients at the optimal lambda.min value were identified as significant prognostic factors and were subsequently included in univariate Cox regression analysis. Variables with a P-value <0.05 in the univariate analysis were included in the multivariate analysis. Hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated for each variable to quantify their association with OS. Significant variables from the multivariate analysis were used to construct a nomogram via R software, “rms” package.
Time-dependent receiver operating characteristic (ROC) curves was applied to evaluate the discrimination ability of the nomogram through “timeROC” function in R software, “timeROC” package. Besides, time-dependent Concordance index (C-index) of different models was also calculated to compare their predictive performance through “cindex” function via R software, “pec” package. Furthermore, calibration curves of different prediction time points of the nomogram were generated to assess the consistence between the actual- and predicted- OS probability of patients using “calibrate” function in R software, “rms” package. Decision curve analysis (DCA) was performed to evaluate the clinical utility and net clinical benefits of the nomogram in guiding clinical practice.22-24
Results
Clinical Characteristics of the Participants
Clinical Characteristics of Head and Neck MATL Lymphoma in the Training and Validation Cohort.
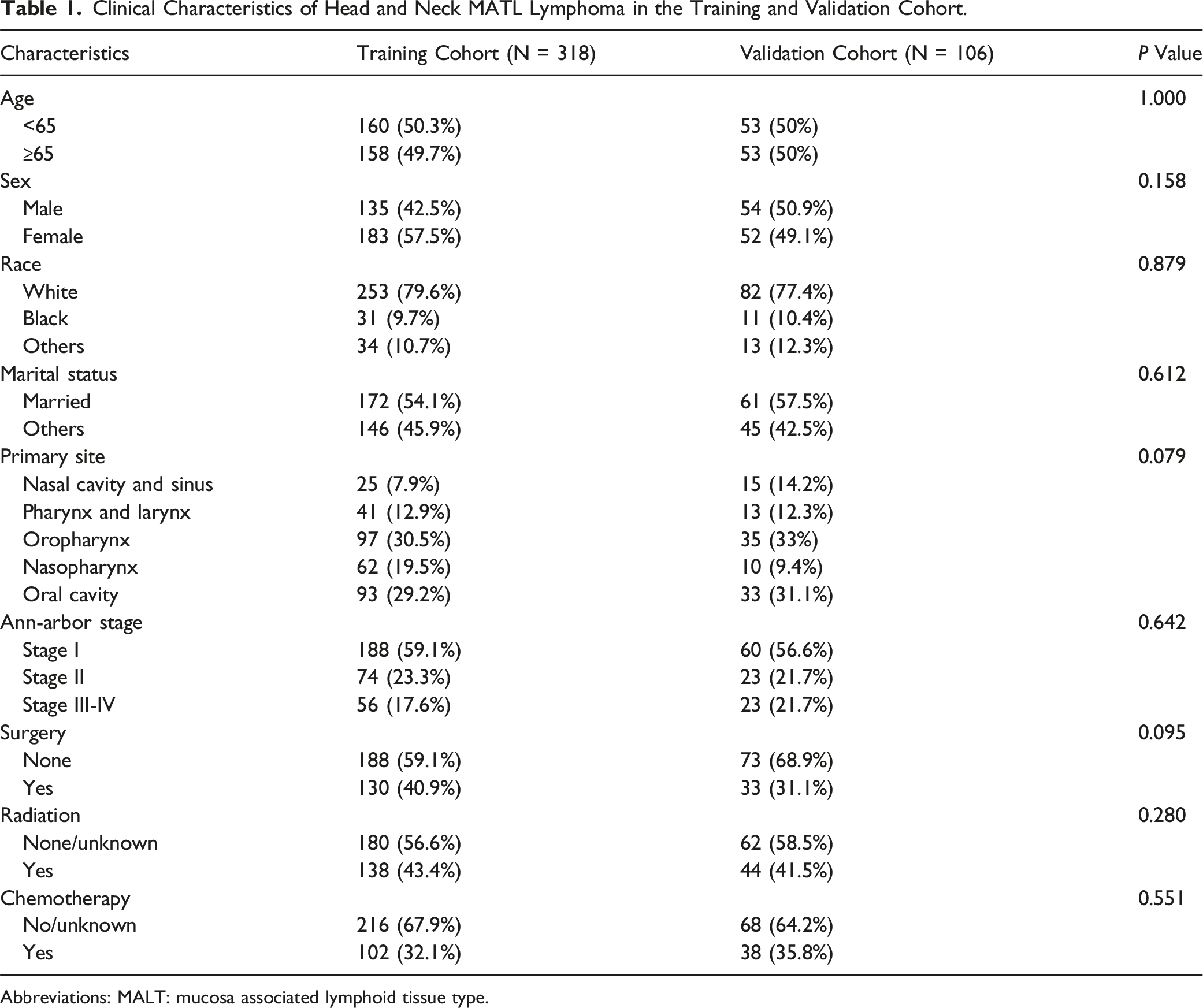
Abbreviations: MALT: mucosa associated lymphoid tissue type.
Prognostic Factors Identification and Age-Based Nomogram Development
The median OS for patients in both the training and validation cohorts was 14.8 years (95% CI: 13.7 years–not reached, Figure 1A), and 15 years (95% CI: 12.7 years–not reached, Figure 1B). Using LASSO regression, six potential prognostic variables were initially identified, including age, sex, marital status, race, Ann-Arbor stage, and chemotherapy (Figure 2 and Table S1). To further investigate prognostic factors for OS in patients with MALT lymphoma, univariate Cox regression analysis was performed in the training cohort. The analysis revealed significant associations between OS and variables such as age, race, marital status, and Ann-Arbor stage (Table 2). Subsequent multivariate Cox regression analysis demonstrated that age exceeding 65 years (HR: 2.97, 95% CI: 1.94-4.57; P < 0.001) and unmarried status (HR: 1.58, 95% CI: 1.07-2.33, P = 0.023) were significantly associated with shorter OS (Table 2). Conversely, head and neck MALT lymphoma patients of black race (HR: 0.25, 95% CI: 0.09-0.69, P = 0.007) exhibited a correlation with longer OS (Table 2). Recognizing that the predictive efficacy of individual factors is inferior to a combined approach, we developed a nomogram incorporating significant variables from the multivariate analysis to predict various time points of OS probability. As depicted in Figure 3, clinicians can easily estimate the 5-year, 10-year, and 15-year OS probabilities for head and neck MALT lymphoma patients in a clinical setting using this nomogram. Consequently, physicians can make timely and targeted interventions for high-risk patients. Kaplan-Meier survival curves illustrate the median overall survival (OS) time for head and neck mucosa-associated lymphoid tissue (MALT) lymphoma in the training cohort (A) and validation cohort (B). LASSO regression for identifying prognostic factors of overall survival (OS) in head and neck mucosa-associated lymphoid tissue (MALT) lymphoma. (A) Coefficient path plot showing the shrinkage of variable coefficients as the penalty parameter (log lambda) increases. (B) 10-fold cross-validation plot for selecting the optimal lambda. The Prognostic Factors of OS for Head and Neck MATL Lymphoma Patients in the Training Cohort. Abbreviations: OS: overall survival; MALT: mucosa associated lymphoid tissue type; HR: hazards ratio; CI: confidence interval. An age-based nomogram predicts the 5-year, 10-year, and 15-year overall survival (OS) probability of patients with head and neck mucosa-associated lymphoid tissue (MALT) lymphoma. This patient scored a total of 232 points on the nomogram, with estimated 5-year, 10-year, and 15-year OS probabilities of 66.0%, 42.8%, and 11.4%, respectively.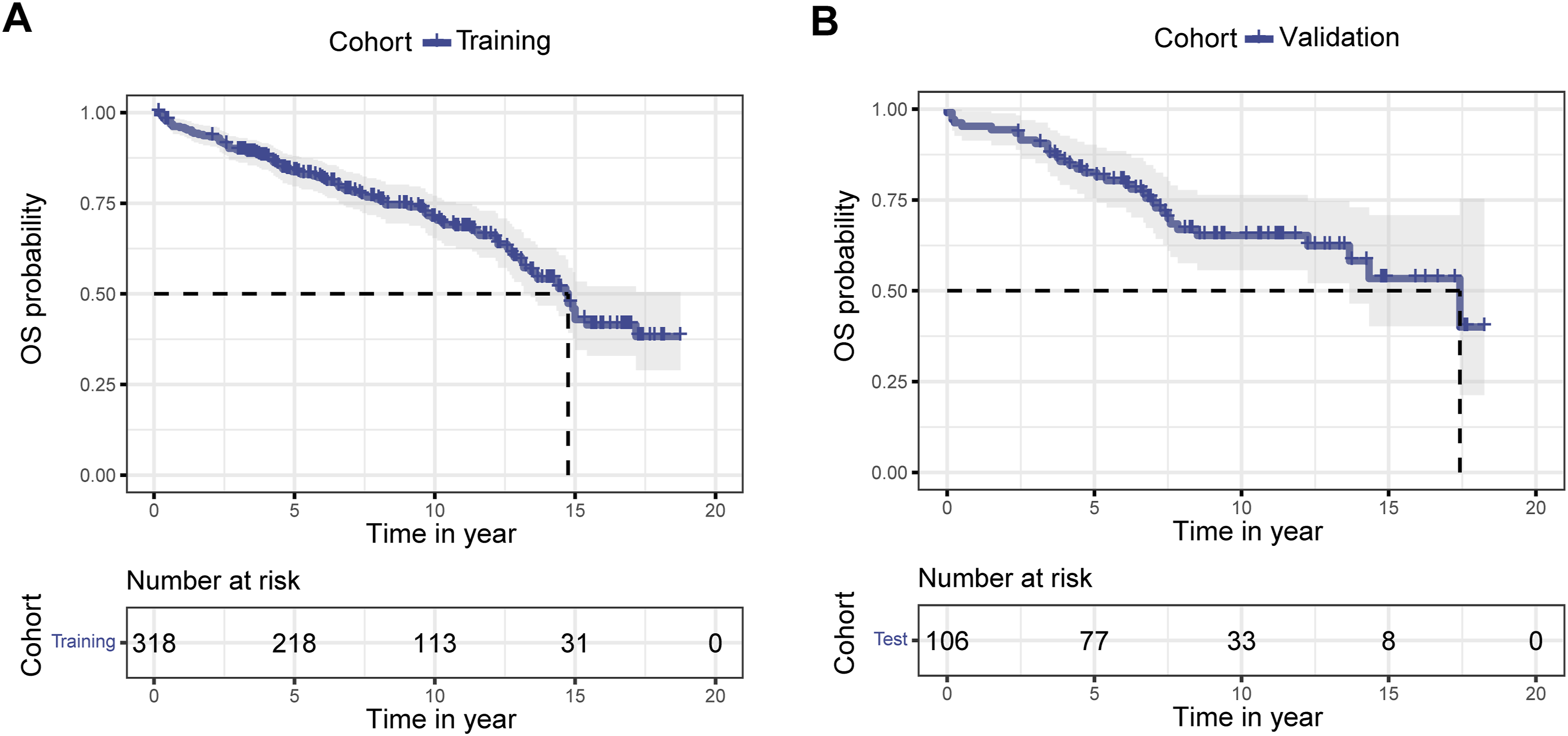



The Validation and Performance Evaluation of the Age-Based Nomogram
Then, we evaluated the predictive accuracy of the nomogram within both the training and validation cohorts. Analysis of time-dependent ROC curves demonstrated the effective performance of the age-based nomogram in forecasting the 5-year (area under the curve (AUC): 0.640) and 10-year OS (AUC: 0.705) probabilities for patients with head and neck MALT lymphoma in the training cohort (Figure 4A). Notably, the age-based nomogram exhibited impressive discriminative capabilities in predicting the 15-year OS probability, achieving an AUC of 0.842 (Figure 4A). These results were consistently observed in the validation cohort (Figure 4D). Subsequently, time-dependent C-indices were computed to assess the nomogram’s discriminative capacity at different time points. In line with the time-dependent ROC curves, the age-based nomogram consistently demonstrated satisfactory discrimination in predicting the 5-year, 10-year, and 15-year OS probabilities, ranging from 0.626 to 0.711 (Figure 4B and Table 3). Moreover, we compared the discriminative ability of the age-based nomogram with that of age and Ann-Arbor stage. As anticipated, our findings revealed that the age-based nomogram outperformed age and Ann-Arbor stage in terms of predictive power (Figure 4B and Table 3). This superior discrimination ability of the age-based nomogram was similarly observed in the validation cohort (Figure 4E and Table 3). Additionally, calibration curves were constructed for different prediction time points to assess the alignment between the actual OS probability and the OS probability predicted by the age-based nomogram. The results demonstrated satisfactory consistency between actual and predicted OS probabilities at various time points in both the training (Figure 4C) and validation (Figure 4F) cohorts. In summary, our findings underscore the excellent predictive performance of the age-based nomogram in estimating the 5-year, 10-year, and 15-year OS probabilities for patients with head and neck MALT lymphoma. Evaluation of the prediction performance of the age-based nomogram for the 5-year, 10-year, and 15-year overall survival (OS) probability of patients with head and neck mucosa-associated lymphoid tissue (MALT) lymphoma. (A–C) Displayed time-dependent receiver operating characteristics (ROC) curves (A), time-dependent Concordant index (C-index) (B), and calibration curves (C), respectively, for the age-based nomogram in the training cohort. (D–F) Displayed time-dependent ROC curves (D), time-dependent C-index (E), and calibration curves (F), respectively, for the age-based nomogram in the training cohort. (G–I) Showcased decision curve analysis (DCA) of the age-based nomogram at different prediction time points in the training cohort. Time-Dependent C-Index of the Nomogram in Predicting the 5-Year, 10-Year, and 15-Year OS of Head and Neck MALT Lymphoma. Abbreviations: OS: overall survival; MALT: mucosa associated lymphoid tissue type.

Clinical Utility and Risk Stratification Ability of the Nomogram
Subsequently, we assessed the practical applicability of the age-based nomogram in forecasting diverse time intervals for OS probability among patients with head and neck MALT in our study, utilizing DCA. As depicted vividly in Figure 4G–I, the nomogram proved to be highly advantageous for patients within a specific risk threshold range in the training cohort, surpassing the predictive capability of individual factors within the nomogram. Notably, DCA results in the validation cohort indicated a substantial clinical net benefit of the age-based nomogram when forecasting 5-year and 10-year OS (Figure S1A–C).
According to the nomogram, we computed the risk scores for each patient within the training and validation cohorts. Our analysis revealed that patients who succumbed to head and neck MALT exhibited higher risk scores than their counterparts who remained alive, a pattern observed in both the training (Figure 5A) and validation (Figure 5C) cohorts. To evaluate the risk stratification efficacy of the age-based nomogram, we categorized patients in the training and validation cohorts into low, moderate, and high-risk groups based on the transformed risk scores derived from the nomogram. Subsequently, Kaplan-Meier survival curves were constructed to visually represent the survival disparities among these risk groups. As anticipated, patients classified in the high-risk group demonstrated a significantly reduced OS probability compared to those in the moderate- and low-risk groups in both the training (Figure 5B) and validation (Figure 5D) cohorts. Collectively, these findings underscore the age-based nomogram’s ability to effectively discriminate between patients in distinct risk groups, highlighting its potential for prognostic stratification. Evaluation of the risk stratification ability of the age-based nomogram in the training (A-B) and validation (C-D) cohorts. (A) Presented waterfall plots demonstrating the distribution of nomogram-predicted risk scores among patients with different survival statuses in the training cohort. (B) Displayed a Kaplan-Meier survival curve illustrating the survival difference between different risk groups in the training cohort. (C) Showed waterfall plots for the validation cohort, and (D) presented a Kaplan-Meier survival curve for the survival difference between different risk groups in the validation cohort.
Discussion
Our study, encompassing a cohort of 424 participants with head and neck MALT lymphoma, provides a comprehensive analysis of the clinical characteristics and demographics associated with this rare malignancy. Notably, a significant proportion of participants were aged 65 and older, emphasizing the prominence of this disease in the elderly population. Our findings elucidate crucial prognostic factors influencing OS in patients with head and neck MALT lymphoma. Multivariate analysis highlighted age exceeding 65 years and unmarried status as independent factors significantly associated with shorter OS. The protective effect observed in black race patients adds nuance to the understanding of prognostic markers in MALT lymphoma. The recognition of these factors is pivotal for risk stratification and personalized treatment approaches. Consistent with other lymphoma types, age emerges as a robust prognostic factor for patients with head and neck MALT lymphoma. Its significant impact is evident across various lymphoma subtypes and has been incorporated into prognostic scores such as the International Prognostic Index (IPI) for DLBCLs, 25 the Follicular Lymphoma International Prognostic Index (FLIPI) 26 and FLIPI-2 27 for follicular lymphoma, the Mantle Cell Lymphoma International Prognostic Index (MIPI) for mantle cell lymphoma, 28 the Burkitt Lymphoma International Prognostic Index (BL-IPI) for Burkitt lymphoma, 29 and the International Extranodal Lymphoma Study Group (IELSG) prognostic index for primary central nervous system lymphomas (PCNSL). 30 In a recent study, Zhang and colleagues explored prognostic factors for head and neck MALT lymphoma based on 105 patients, 12 revealing that the IPI is also an independent risk factor for OS in these cases. Consequently, these findings underscored the pivotal predictive role of age in determining the OS for individuals with head and neck MALT lymphoma.
The association between marital status and the prognosis of lymphoma patients has been a focus of interest, with several studies suggesting a positive impact of marital status on cancer outcomes, including those with lymphoma.31-35 Evidence suggests that psychosocial factors, which play a crucial role in tumorigenesis and prognosis, may mediate the relationship between marital status and prognosis. 34 For instance, individuals in a marital relationship often benefit from stronger emotional support and better financial stability, which can boost confidence in fighting the disease and improve treatment adherence. 35 Practical support is another important factor that may help explain this positive association. Married patients often receive assistance in managing cancer-related challenges, such as transportation for medical appointments, medication management, or caregiving support, which may enhance their ability to endure and comply with treatment. 36 It is essential to recognize that this association is not necessarily due to marital status alone but rather reflects a complex interplay of social, psychological, and biological factors. The impact of marital status on prognosis underscores the importance of support systems in improving adherence to treatment and overall well-being. However, further well-designed cohort studies are warranted to investigate the mechanisms underlying the influence of marital status on the prognosis of malignancies, including MALT lymphoma, and to elucidate the independent contribution of marital status as a prognostic factor. Furthermore, we observed an association between black race and longer OS in patients with head and neck MALT lymphoma, which warrants further investigation. Potential explanations may include differences in tumor biology, genetic predispositions, or variations in healthcare-seeking behavior and treatment patterns. In a recent study conducted by Heiden and colleagues, 37 they investigated the racial disparities in the surgical treatment of clinical stage I lung cancer among veterans. Intriguingly, they observed that black patients had significantly better risk-adjusted OS compared to white patients. While our study identifies marital status and race as independent prognostic factors, the underlying mechanisms remain multifaceted and require further exploration. Incorporating detailed socioeconomic and biological data in future studies will be critical to providing a more comprehensive understanding of these associations.
As is well-known, the predictive efficacy of a single factor is inferior to that of a combination of factors. To enhance prognostic accuracy, we developed an age-based nomogram incorporating significant variables identified in the multivariate analysis to predict the OS probability of head and neck MALT lymphoma at different time points. The nomogram facilitates a practical estimation of 5-year, 10-year, and 15-year OS probabilities for clinicians. This tool enables a nuanced approach to patient management, allowing for timely interventions tailored to individual risk profiles. Our evaluation of the age-based nomogram revealed robust predictive accuracy in both training and validation cohorts. The nomogram consistently outperformed age and Ann-Arbor stage, highlighting its superiority in prognostic prediction. The clinical utility of the age-based nomogram was further emphasized through DCA, demonstrating its advantage over individual factors in predicting OS probabilities. Risk stratification based on nomogram-derived scores effectively categorized patients into low, moderate, and high-risk groups, with corresponding Kaplan-Meier survival curves illustrating significant differences in OS probabilities. This underscores the nomogram’s potential in guiding clinical decision-making and identifying patients who may benefit from more aggressive therapeutic strategies. While the age-based nomogram demonstrated excellent predictive performance for 15-year OS, the predictive accuracy for 5-year and 10-year OS was relatively lower. This may be attributed to several factors. First, the heterogeneity of the patient population, including variations in comorbidities, treatment regimens, and follow-up durations, could introduce variability in short- and mid-term outcomes. Second, the retrospective nature of the study and the reliance on the SEER database limit the availability of detailed treatment information and other potential prognostic factors, such as molecular and genetic markers, which may play a critical role in influencing outcomes over shorter time frames. These limitations may have contributed to the reduced accuracy observed at 5 and 10 years. Future studies should aim to incorporate additional prognostic variables, including molecular and genetic markers, as well as detailed treatment data, to enhance the model’s discriminatory power. Prospective studies with larger and more diverse cohorts will also be essential to validate and refine the nomogram, ensuring its clinical utility across all time points. Moreover, exploring dynamic prediction models that account for time-dependent changes in patient status could further improve the accuracy of short- and mid-term survival predictions. Additionally, machine learning approaches leveraging large sample sizes and a comprehensive set of predictive factors could be considered in future studies. For instance, Wen and colleagues 4 recently developed an effective nomogram to predict progression-free survival (PFS) in MALT lymphoma using LASSO-Cox regression analysis in a multicenter retrospective cohort study.
Despite the robustness of our findings, this study has some limitations. Firstly, the retrospective nature of the analysis may introduce bias, and the generalizability of our results may be influenced by the specific demographic characteristics of our cohort. Secondly, the data used in this study were drawn exclusively from the SEER database, which, while comprehensive, primarily represents the U.S. population. This may limit the applicability of our findings to other populations with different demographic, genetic, or healthcare characteristics. Thirdly, the data collection period for this study spans from 1975 to 2016, a timeframe during which significant advancements in treatment modalities, particularly chemotherapy and radiotherapy, have occurred. These advancements may have influenced patient outcomes, but the SEER database does not provide detailed information on specific treatment regimens or their evolution over time. As a result, we were unable to account for these changes in our analysis. Additionally, the uncertainty stemming from limited treatment information hinders our ability to definitively assess the impact of various treatment modalities on the prognosis of these individuals. To enhance the robustness and clinical utility of our findings, external validation using independent and more diverse population cohorts is essential. Future studies should aim to validate the predictive accuracy of our age-based nomogram in different geographic regions and healthcare settings. Such efforts would help confirm its utility in guiding clinical decision-making across broader patient populations.
Conclusions
In conclusion, our study provides valuable insights into the clinical characteristics and prognostic factors of head and neck MALT lymphoma. The development and validation of the age-based nomogram represent a significant contribution to enhancing prognostic precision and guiding personalized treatment strategies for patients with this rare malignancy. This practical tool enables clinicians to stratify risk and tailor interventions based on individual patient profiles. However, the retrospective nature of this study and the reliance on the SEER database may limit the generalizability of our findings. Future research with larger and more diverse cohorts, as well as prospective studies, is warranted to validate and extend our findings. These efforts will help address the limitations of this study and further refine the prognostic tools available for patients with head and neck MALT.
Supplemental Material
Supplemental Material - A Novel Age-Based Nomogram as the Best Predictor for Long-Term Overall Survival in Head and Neck Mucosa-Associated Lymphoid Tissue Lymphoma
Supplemental Material for A Novel Age-Based Nomogram as the Best Predictor for Long-Term Overall Survival in Head and Neck Mucosa-Associated Lymphoid Tissue Lymphoma by Chaoxin Fan, Aimin Jiang, Rui Zhao, and Miaomiao Chen in Cancer Control
Footnotes
Acknowledgments
We extend our gratitude to the SEER database for generously providing the original patient data on head and neck MALT lymphoma for this study.
Author Contributions
Conception/Design: C. F. and M. C.; Provision of study material: A. J. and R. Z.; Collection and/or assembly of data: C. F. and A. J.; Data analysis and interpretation: R. Z., C. F., and A. J.; Manuscript writing: C. F.; Final approval of manuscript: C. F. and M. C. All authors have read and approved the final manuscript, and they agree to be accountable for all aspects of the research, ensuring that the accuracy or integrity of any part of the work is appropriately investigated and resolved.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.