
Abstract
Introduction
Young women under 30 years with breast cancer (BC) are an emerging challenge. The purpose is to identify prognostic factors for survival in young women under 30 years of age with BC.
Material and methods
A retrospective cohort study was conducted among women younger than or equal to 40 years with BC and who were treated at the State Cancer Center during the period 2012–2017. Overall survival was assessed using the Kaplan–Meier method and the log-rank test. Univariate and multivariate analysis assessed survival predictors using Cox proportional hazards regression model.
Results
282 young women were included. The >30-year-old subgroup showed a significant association with excess weight (P = .002) compared to the <30-year-old group. The <30-year-old subgroup showed a poor overall survival (56.7%), as well as highly significant values in advanced clinical stages, metastatic nodules, metastasis, and neoadjuvant therapy (P < .001). In Model 3 of the multivariate analysis, age <30 years (HR = 3.0; 95% CI 1.1 to 8.6), triple negative subtype (HR = 2.6; 95% CI 1.1 to 6.0), tumor size >5 cm HR = 2.3; 95% CI 1.03 to 5.1), and advanced clinical stages (HR = 6.6 95% CI 1.3 to 35.5) persisted as predictors.
Conclusions
Being very young (<30 years) is a predictor for limited survival compared to the age of 30–40 years, as well as the tumor covariates for a worse prognosis: triple negative subtype, advanced stages, positive lymph nodes, and distant metastases in liver.
Introduction
Breast cancer is the most common cancer in women around the world. Although it rarely occurs before the age of 40, it is the most common within this age group. 1 In Mexico, the incidence of these cases is reported in a range of 10 to 15%. 2 Due to a later diagnosis associated with multiple factors, such as lack of knowledge of the disease, financial status, 3 level of education, and lack of medical training to detect cancer early, young women generally present advanced clinical stages with molecular subtypes and more aggressive biological characteristics.4,5 Increased body mass index (BMI) in premenopausal women shows a higher proportion of hormone receptor negative, with a predominance of triple negative breast cancer (TNBC) molecular subtype.6,7
Young women have been reported to have a poorer survival rate compared to their older counterparts,8,9 which is associated with an advanced clinical stage and the presence of metastases. 10 Survival tends to be less favorable in the human epidermal growth factor receptor 2 (HER-2) and TNBC phenotypes, and these molecular subtypes are overrepresented in young women at diagnosis. 11 TNCBs usually stand out for their biological peculiarities, reduced survival rate, and lack of effective treatment, as well as an evident tendency to present distant metastases, 12 mainly in bone and liver. 13 Previous studies reported that women <40 years have stronger treatment and additional reproductive challenges. However, the prognostic impact of age remains unclear in this clinical context. This study aimed to identify the main predictors of survival in young women under 30 years of age with BC.
Material and Methods
Participants and Study Design
We conducted a retrospective cohort study from a database that included all women diagnosed with invasive BC and who were ≤40 years old during the period January 2012–December 2017 who were treated at the State Cancer Center (CECan), in Veracruz, Mexico. The sample size was delimited by 100% of the women with invasive BC, aged ≤40 years and who met the rest of the selection criteria from a database with N = 1462 patients. Statistical power will be calculated if no significant association is found between the group <30 years with poor survival.
The maximum monitoring time was 60 months, with a prior evaluation at 24 months. Patients were classified as exposed or unexposed according to age <30 years and ≥30 years. Monitoring included the time interval between the date of diagnosis and the date of the last visit or the date of death from any cause. For the rest of the cohort, the monitoring time ended on December 31st, 2017. The selection criteria were women aged ≤40 years, residing at the state of Veracruz with a confirmed diagnosis of BC during the period January 2012–December 2017 who were treated at the CECan and had a complete clinical record. Information was collected from secondary sources, such as medical records and information provided by the Department of Social Work.
Variables
Survival was the main response variable, which was defined as the time elapsed between the confirmation of the diagnosis of BC and the death of the patient. Death was verified through the death certificate provided by the social work area, or the records made by the Epidemiological System and Death Statistics.
Patients were classified into two groups: <30 years and 30 to 40 years. Predictor variables were: age at diagnosis, clinical stage (according to the criteria established by the American Joint Committee on Cancer, AJCC), 14 positive lymph nodes, metastasis (present or absent at the time of diagnosis), and type of treatment (neoadjuvant or adjuvant). Other recorded covariates were overweight and obesity, which were defined according to the BMI classification proposed by the World Health Organization. 15 The sociodemographic variables included education (no studies, basic education, and secondary-junior high education), occupation (housework or worker), and socioeconomic status, which was classified according to the following variables: family income (55%), work (10%), family expenses (10%), housing (20%), and family health (5%).
The histologic grade score was assessed using standard institutional protocols (considering the following differentiation status: well, moderately, poorly differentiated, and unknown). According to the molecular subtypes for BC, the status of ER, PR, and HER-2 was determined by immunohistochemical analysis (IHC), which was performed by standard procedures on 2–5 mm thick sections for staining, fixed a minimum of 6 and a maximum of 48 hours, and with the use of antibody clones validated for ER, PR, and HER-2. ER and PR are considered positive with a percentage of 1% of positive neoplastic cells. HER-2 overexpression was determined by IHC or FISH technique, scoring a scale from 0 to 3+ and was evaluated as follows: Positive (3+, intense and uniform staining, >10% neoplastic cells), indeterminate (2+, complete and weak staining in >10% of neoplastic cells), and negative (0–1+, no staining is identified, it is weak or incomplete in at least 10% of neoplastic cells). The molecular subtype classification used for this study was as follows: Luminal A: ER +, PR >20%, Ki67 <20%, histologic grade (HG) 1 or 2, and HER-2−; Luminal B: ER +, PR <20%, ki67 >20%, HG 3, HER-2±; HER-2: HER-2 +, ER−, and PR−; Triple negative: ER−, PR−, and HER-2−. These criteria are in accordance with the 2019 Colima Consensus Statement. 16
Statistical Analysis
The continuous variables were expressed as means and standard deviations or as medians and ranges. The categorical variables were expressed as percentages and compared using the chi-square or Fisher’s exact test. Survival analysis was calculated using the Kaplan–Meier method. Patients who were still alive at the end of the monitoring or whose status was unknown were considered as censored data. The survival probabilities for each possible prognostic factor were compared using the Log–Rank test. A multivariate Cox regression analysis was conducted to identify those predictors of survival adjusted for the rest of the covariates. Model 1 included Age, overweight, schooling, and tumor size, while Model 2 included, in addition to the previous ones, histological grade, clinical stage, and metastasis (liver). Finally, Model 3 included metastatic nodes, molecular subtypes, and treatment. In the multivariate analysis, the hazard ratio (HR) and its 95% confidence intervals were estimated. Analyses were carried out using the statistical software SPSS, version 25.0 (IBM Inc., NY, USA).
Results
Clinical and Pathological Characteristics and Treatment.
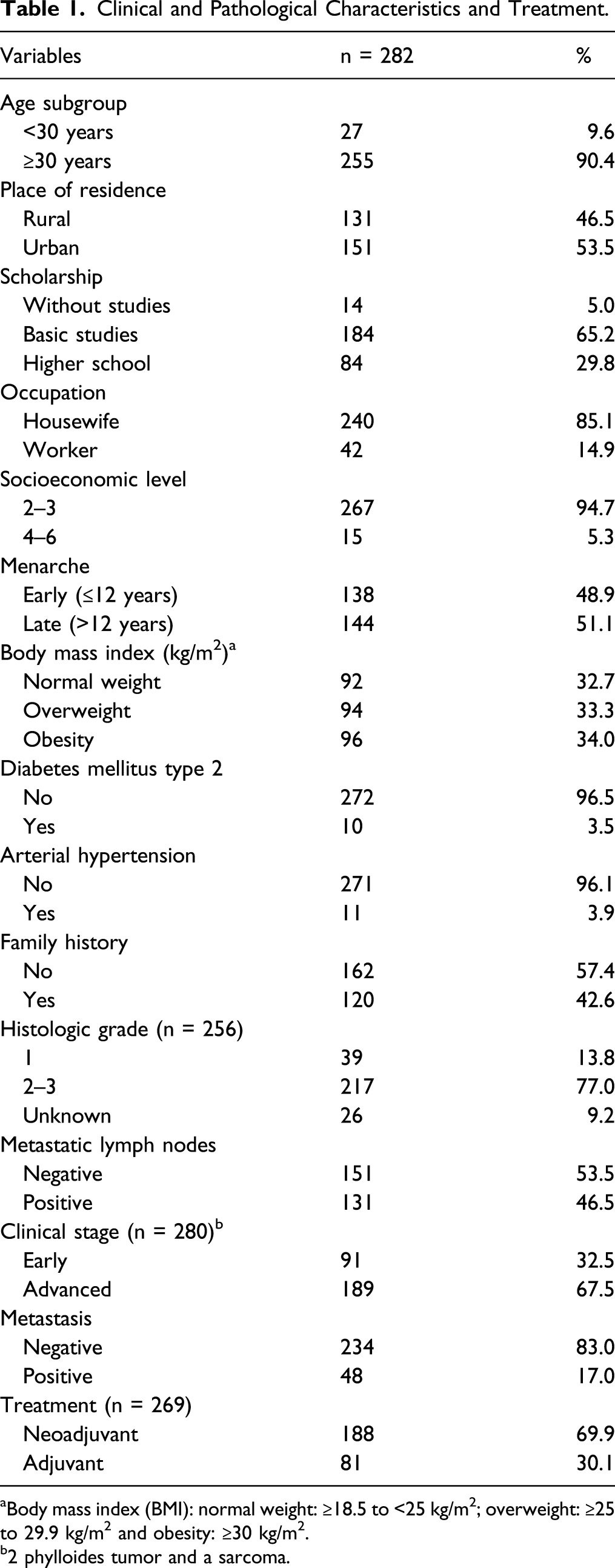
aBody mass index (BMI): normal weight: ≥18.5 to <25 kg/m2; overweight: ≥25 to 29.9 kg/m2 and obesity: ≥30 kg/m2.
b2 phylloides tumor and a sarcoma.
Demographic and Clinical Factors Related to Young and Very Young Subgroups.

aProportions were compared through the chi-square test. Significant value P < .05.
bBasic level of education: primary and secondary. BMI = Body mass index.
Survival According to Age, Clinical Variables and Treatment at 5-Year of Follow-Up.

aKaplan–Meier method.
bLog–Rank test.
CBody mass index (BMI): overweight ≥25 kg/m2 + obesity ≥30 kg/m2. 15

Overall survival according to age, clinical variables, and tumor subtypes. Estimation of survival function using Kaplan–Meier curves. (A
Predictive Factors of Poor Survival in a Multivariate Analysis.

Dependent variable: survival.
aHR: hazard ratio obtained by Cox regression.
b95% CI: confidence interval at 95%.
cExcess weight included to subjects with overweight and obesity. It was defined as body mass index (BMI) ≥ 25 kg/m2. 15
dBasic level of education = primary and secondary. HER-2 human epidermal growth factor receptor 2 positive.
Discussion
Very young women with BC have been distinguished by presenting histopathological and biological characteristics of reserved impact and lower survival. Our study revealed that age <30 years in women with BC turned out to be a predictor for poor survival rate (HR = 3.0; 95% CI 1.1 to 8.6, P = .04), compared to its counterpart (30–40 years). The lower survival rate was significantly related to a wide variety of aggressive characteristics, such as tumor size (HR = 2.3 95% CI 1.03 to 5.1; P = .04), advanced clinical stage (P = .03), positive nodes (HR = 2.4; CI 95% 1.1 to 5.5; P = .03), and triple negative molecular subtype. The characteristics describing this very young subgroup are consistent with other studies.17-19 Likewise, Han et al reported that, in patients <35 years, the risk of death increases by 5% for each 1-year decrease in age. 20
In consistence with the age subgroup, a predominance of the triple negative molecular subtype (37.14%) was observed and, in addition to being an important subtype of poor prognosis, it was associated with the probability of survival in the multivariate analysis (HR = 2.6; 95% CI 1.1 to 6.0, P = .03), in addition to that reported in previous studies. 21 The presence of HER-2 tumors was also evident in 13.47% of the total; a similar figure was reported by Sabiani et al, 11 who also showed a poor survival rate, although not as significant as in our cohort.
Of clinical importance was the high percentage of diagnoses in advanced stages among the very young population (80.0%), a figure comparable to that reported by Goksu et al, 22 but higher than those reported in the Latin American population. 23 The association between the clinical stage and low survival can be explained by the higher risk of late diagnosis in young women, due to the low perception and suspicion of cancer risk from the first symptoms to the first contact with a doctor, as well as the time interval between diagnostic biopsy results and initiation of treatment. 24
The results of this research add evidence supporting the fact that very young women show quite violent local growth and rapid progression and presented a high rate of metastasis with a direct impact on significantly lower survival (P < .001) and the main organs remotely affected were bones and liver, as observed in a study in Moroccan women. 25 However, in the multivariate result, only liver metastasis was associated with a higher risk of death (HR = 7.8; P = .005). In contrast, Mustillo et al emphasize that survival was higher in women <40 years with initial brain metastasis. 26 However, it must be remembered that metastasis is an important predictor of severe and poor survival, but prognosis will be determined by metastatic pattern and molecular subtype.
Notably, almost all women of the cohort were from a low socioeconomic status (94.7%). Regarding formal education, 65.2% had completed at least junior high school, which is consistent with economic and education levels reported by Mexican authors and other Latin American cohorts.21,27 Other authors suggest that low socioeconomic status and lower education are associated with poor survival from BC, additionally, social and cultural environment may have influenced her late visit to the doctor and access to some aspects of treatment. 28
Epidemiological studies of the combination of BC and obesity pose unique challenges, experience more treatment-related complications, and worse prognosis,21,29 and are associated with an increased risk of progression, recurrence, and survival decrease of young women with BC. 30 Although in our study these data were not significant in the multivariate analysis, we found a predominance of overweight in women ≥30 years, as reported in previous studies 31 and that is related to that reported by the National Health and Nutrition Survey 2018 (ENSANUT, since it is an acronym in Spanish). 32
An aggressive treatment has been justified in young women with BC due to its worse prognosis. 33 More than half of the patients in our cohort received neoadjuvant treatment, which was significantly associated with the probability of survival (P < .001). The nature of the disease at a young age may foster the implementation of new diagnostic, preventive, and therapeutic approaches to reduce the mortality figures that most afflict this population.
The previously described variations on very young women with BC may be strongly related to the low identification of various risk factors and the performance of self-care practices among younger women, as well as differentiated conditions for access to health services, early detection tests, and timely treatment that, as a consequence, make young women look for medical assistance at advanced stages at the time of diagnosis, presence of metastases, and a significant predominance of excess weight, among other elements associated with a poor outcome.
The main limitations of this study include its retrospective nature and the inherent restrictions on the quality of information in clinical records. Our cohort represented 5 years of follow-up at the largest State Oncology Center; taking into account the significance of these results, they need to be validated with a larger sample size in more hospitals.
Conclusions
Our results show poor survival for the very young subgroup (age <30 years) and are related to aggressive characteristics of the tumor, the influence of the triple negative subtype, as well as the presence of very large tumors, positive nodes, advanced disease, and presence of distant metastases at the time of diagnosis. These findings may have important implications regarding the etiology and prognosis of BC in very young women. However, more research is required to support or reject this hypothesis.
Footnotes
Author Contributions
Conceptualization, M.T.A.B., K.A.S.J and R.E.G.G.; methodology, M.T.A.B., K.A.S.J, E.C.G.R. and J.M.R.; validation, M.T.A.B., K.A.S.J. and E.C.G.R.; formal analysis, J.M.R and C.A.A.R.; investigation, K.A.S.J, E.C.G.R. and M.T.A.-B.; writing-original draft preparation, M.T.A.B., K.A.S.J., C.L.L.S and J.M.R; writing-review and editing, M.T.A.B, J.M.R. and R.E.G.G.; CLLS supervision, M.T.A.B., J.M.R
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Research Ethics Committee of the CECan, of State Cancer Center, Ministry of Health of the State of Veracruz, with registration number C.E.I./2018/053.