
Abstract
Purpose
To identify prognostic factors of survival and recurrence in advanced ovarian cancer patients undergoing radical surgery and HIPEC.
Methods
In a single Department of Surgical Oncology, Peritoneal Surface Malignancy Program, and over a 16-year period, from a total of 274 epithelial ovarian cancer patients, retrospectively, we identified 152 patients undergoing complete (CC-0) or near-complete (CC-1) cytoreduction, including at least one colonic resection, and HIPEC.
Results
Mean age of patients was 58.8 years and CC-0 was possible in 72.4%. Rates of in-hospital mortality and major morbidity were 2.6% and 15.7%. Only 122 (80.3%) patients completed Adjuvant Systemic Chemotherapy (ASCH). Rates of metastatic Total Lymph Nodes (TLN), Para-Aortic and Pelvic Lymph Nodes (PAPLN) and Large Bowel Lymph Nodes (LBLN) were 58.7%, 58.5%, and 51.3%, respectively. Median, 5- and 10-year survival rates were 39 months, 43%, and 36.2%, respectively. The recurrence rate was 35.5%. On univariate analysis, CC-1, high Peritoneal Cancer Index (PCI), in-hospital morbidity, and no adjuvant chemotherapy were adverse factors for survival and recurrence. On multivariate analysis, negative survival indicators were the advanced age of patients, extensive peritoneal dissemination, low total number of TLN and no systemic PAPLN. Metastatic LBLN and segmental resection of the small bowel (SIR) were associated with a high risk for recurrence.
Conclusion
CC-O is feasible in most advanced ovarian cancer patients and HIPEC may confer a survival benefit. Radical bowel resection, with its entire mesocolon, may be necessary, as its lymph nodes often harbor metastases influencing disease recurrence and survival. The role of metastatic bowel lymph nodes has to be taken into account when assessing the impact of systemic lymphadenectomy in this group of patients.
Introduction
Globally, Ovarian Cancer is the third most common gynecological malignancy with CLOBOCAN reporting, for the year 2020, 313 959 new cases and 207 252 deaths. 1
In advanced ovarian cancer, complete cytoreduction (CC-0), frequently involving multi-visceral resection, and the response to chemotherapy are the 2 most significant factors of long-term survival. 2 However, the reported overall 5-year survival does not seem to exceed 30% and there are major discrepancies of quality of care on both sides of the Atlantic. In a recent French study, only 30% of patients received appropriate care according to guidelines.3,4
There is evidence that intraperitoneal chemotherapy improves disease-free and overall survival, but this method has not been universally adopted.5-7 Over the last 30 years, cytoreductive surgery, in combination with hyperthermic intraperitoneal chemotherapy (HIPEC), has been shown to be a promising strategy for peritoneal malignancies by numerous observational and one randomized study.8-12 A recent prospective randomized trial showed that HIPEC may improve recurrence-free and overall survival. Importantly, the incidence of morbidity was the same in both the HIPEC and non-HIPEC group. 13 However, there is no universal standardized regime and there is concern with the associated reported toxicity.
Ovarian cancer progresses through the peritoneal surfaces and the lymphatic network. One prospective randomized trial showed that systemic para-aortic and pelvic lymphadenectomy (PAPLN) may offer a significant survival benefit, but the multicentric randomized LION study failed to reproduce these results.14,15 However, little attention has been paid to the impact of metastatic bowel (mesorectal-mesocolic) lymph node resection on completeness of cytoreduction, risk of recurrence, and overall survival. It appears that these nodes may affect long-term survival whenever the large bowel is involved.16-19 Also, recent research has focused on the potential therapeutic benefit of the excision of hepatic hilar and cardiophrenic lymph nodes.20,21
In locally advanced ovarian cancer, standard pelvic peritonectomy procedures, as described by Sugarbaker, 22 include the en-bloc resection of pelvic peritoneum, internal female genitalia and rectosigmoid with the relevant lymph nodes. In cases of pelvic carcinomatosis, many authors consider this en-block resection to be a crucial step in order to achieve complete cytoreduction, because the rectosigmoid colon and the pelvic peritoneum are invariably involved. This concept has been questioned in ovarian cancer surgery because of the potentially increased morbidity associated with bowel resection and certain authors have argued that sparing the large bowel does not seem to affect survival. 23 However, multiple bowel resections are necessary in 26%-50% of cases in order to achieve complete cytoreduction. 18
Although there are no randomized trials, the depth of bowel-wall invasion appears to be a prognostic survival indicator and the risk of associated metastatic large bowel lymph nodes (LBLN) is related to bowel wall invasion. 16 Ovarian cancer may metastasize to lymph nodes of the large bowel as if the primary site were of colorectal origin. 17 Therefore, in ovarian pelvic carcinomatosis, a radical rectosigmoid colectomy, up to the origin of its associated mesocolon, may be required for the en-bloc resection of the relevant bowel lymph nodes.
The present study is referred to patients with advanced ovarian cancer treated by one surgical team with a standard radical surgical technique. The main objective of the study was the identification of the degree of bowel involvement and rate of its metastatic lymph nodes, as well as their possible influence on survival and recurrence.
Methods
Patients
The files of 274 women with advanced epithelial ovarian cancer, treated over a 16-year period, were retrospectively reviewed, following permission by the Ethics and Compliance Committee of our Academic Hospital. The committee accepted our request under the conditions that there were no financial requirements for its execution, that it was in accordance with the legislation and that we had civil liability coverage, all of which were met. The signed informed consent form by the patients was in accordance to the daily clinical practice procedures of our Hospital, specifying that their anonymous data could be used for research purposes. Only 152 patients with stage IIIC disease, undergoing complete (CC-0) or near complete (CC-1) cytoreduction, that required at least 1 colonic resection, were included in the analysis. These patients underwent primary, interval, or even completion cytoreduction after incomplete surgery in other centers. From the latter group, 21 patients received NACT and the remaining 47 patients had inadequate primary debulking in other centers and, therefore, underwent completion cytoreduction.
Patients with borderline or non-epithelial tumors were excluded from the analysis.
Only patients with acceptable performance status (Karnofsky scale>50%), adequate cardiac-pulmonary-renal-hepatic-bone marrow function and with no distant or unresectable metastases were included in the study.
Treatments
A midline incision, from the xiphoid process to symphysis pubis, was routinely performed for maximal access to the abdominal cavity. After adhesiolysis, the extent of the disease was assessed by calculating the Peritoneal Cancer Index (PCI). 22 Cytoreductive surgery was possible using standard peritonectomy procedures, with the intention to remove entirely the macroscopically visible tumor. 24 Frequently with segmental colectomies, prophylactic divergent stomas were used. In all colectomies, a radical excision of the associated mesocolon and lymph nodes was performed. Until 2010, only bulky para-aortic and pelvic lymph nodes were removed. After 2010, systemic para-aortic and pelvic lymphadenectomy (PAPLN) was established as a standard step, including resection of all lymph nodes around the aorta and the inferior vena cava from the level of the left renal vein down to the common, external and internal iliac, presacral, and obturator nodes. At the end of surgery, the completeness of cytoreduction was assessed by calculating the CC-score. 24
HIPEC was applied after tumor resection and before the reconstruction of the gastrointestinal tract, using the open abdominal (Coliseum) technique. A continuous closed circuit of 2 inflow and 2 outflow drains, 1 heat exchanger, and 2 roller pumps connected to the inflow and outflow drains (Sun-Chip, Gamida Tech, France) were used. The cytostatic drugs, diluted in 2-3 L of Ringer’s Lactate or Normal Saline solution, were instilled in the abdominal cavity as soon as the temperature exceeded 40°C. The mean abdominal temperature was maintained at 42.5-43°C during perfusion. Cis-platin (50 mg/m2) and doxorubicin (15 mg/m2) were used for chemotherapy-naïve or platinum chemo-sensitive patients for 90 minutes. Platinum chemo-resistant patients received melphalan (60-70 mg/m2) or gemcitabine (1000 mg/m2) for 60 min. Early postoperative intraperitoneal chemotherapy (EPIC) was used in patients that underwent CC-1 surgery, via a Tenckhoff catheter, for the first 5 postoperative days. Taxotere (20 mg/m2), diluted in 1.5 L of D1.5W, was used for EPIC. All patients were recommended to receive adjuvant systemic chemotherapy (ASCH). All patients remained in the Intensive Care Unit (ICU) for at least 24 h. The patients who received EPIC remained in the ICU for 5 days.
Histopathology
The histopathological type and grade (G) were recorded for every case. Resected lymph nodes were separated in (a) PAPLN (aortocaval, external iliac, internal iliac, obturator, and presacral), (b) LBLN (Large Bowel Lymph Nodes), (c) SBLN (Small Bowel Lymph Nodes), (d) OLN (greater and lesser omentum lymph nodes), and (e) DLN (distant lymph nodes of any other nodal group above the renal vessels). The depth of the large bowel wall invasion was recorded as (a) serosal invasion (SI), (b) invasion of the muscular layers (MI) and (c) full bowel wall invasion, with the mucosa included (FBWI). The morbidity was classified according to Clavien-Dindo criteria. 25
Follow-Up
All patients were followed, until recurrence or death, every 3 to 4 months during the first year and every 6 months later. The diagnosis of recurrence was based on clinical examination, thoracic and abdominal CT scans (including PET-CT scan if necessary), and elevated CA-125 serum levels. Survival was recorded from the time of initial examination until death or until the last examination. Recurrences were recorded and characterized as distant or loco-regional ones.
Statistical Analysis
Statistical analysis was possible using the SPSS (Statistical Package for Social Sciences version 22.0). The results were expressed as mean (Standard Deviation-SD) or as median values (interquartile range-IQR). Qualitative variables were expressed as absolute and relative frequencies. Life table analyses were used to calculate cumulative survival and recurrences rate for specific time intervals (log-rank test in Kaplan-Meier analysis). The prognostic value of each variable for recurrence and survival was, firstly, assessed by univariate Cox regression analysis. Variables that showed significant association with the outcome were included in the multivariate Cox proportional-hazard model, in a stepwise method, in order to determine the independent predictors for recurrence and survival. The assumption of proportional hazards was evaluated by testing for interaction with a continuous time variable. Kaplan–Meier survival estimates for events were graphed over the follow-up period. All reported P values are two-tailed. Statistical significance was set at P < .05.
Results
Clinico-Pathological Characteristics
Clinicopathological Characteristics of Study Group.

The extent of large bowel involvement was not greatly influenced by NACT, although there was considerable reduction of the extent of small bowel burden. However, as there was no consistent method of assessing the reduction of the extent of bowel involvement in patients with NACT or those initially operated in other centers, this detail was not evaluated in our analysis.
Despite recommendations, only 122 (80.3%) patients were able to complete Adjuvant Systemic Chemotherapy (ASCH). The reasons that certain patients did not receive adjuvant chemotherapy are the following: 4 patients died in the early postoperative period, 12 patients developed severe (grade III & IV) postoperative complications, which rendered them very frail to continue with chemotherapy. The remaining patients, the vast majority of whom had received NACT, refused any further systemic treatment.
Postoperatively, all patients with primary debulking surgery received intravenous paclitaxel 175 mg/m2, carboplatin (area under the curve = 6), and bevacizumab 15 mg/kg for 6 cycles on day 1, every 21 days. Bevacizumab was omitted in the first cycle and continued as a single agent for 1 year. In case of interval debulking surgery, the patients received 3 cycles of paclitaxel and carboplatin pre-operatively and another 3 cycles postoperatively (at the same dosage as in the adjuvant setting). Bevacizumab was added to the first and second cycle of the neoadjuvant chemotherapy, whereas postoperatively it was administered again from the second cycle and until a total of 1 year was completed. Bevacizumab was administered according to international guidelines. However, we recorded only 2 cases of bowel anastomotic leakage and these were in the primary debulking group, with no previous exposure to Bevacizumab.
The included G1 were only 3 cases (2%), which does not have any effect on statistical analysis. However, all these were G1 cases with disseminated peritoneal disease, thus necessitating the need for systemic chemotherapy.
The 30-day in-hospital mortality was 2.6% (4 patients). One patient died because of pulmonary failure, 1 of postoperative peritonitis-sepsis, 1 of myocardial infarction, and 1 of massive pulmonary embolism. Morbidity was recorded in 44 (28.9%) patients. Grade I & II complications were recorded in 12 (7.9%) and 8 (5.3%) patients. Grade III complications were recorded in 7 patients (4.6%), 5 with intra-abdominal abscesses and 2 with bowel anastomotic failures. Grade IV complications were recorded in 17 patients (11.1%), including pulmonary embolism (3), anastomotic failure (6), intra-abdominal abscess (7), and wound dehiscence (1).
The mean and median (IQR) total number of the resected lymph nodes (TLN) was 26 (2-142) and 16 (9-36), respectively. Metastatic lymph nodes (MLN), regardless of the site of resection, were identified in 91 (58.7%) patients. The IQR of MLN, regardless of the site of resection, were 6 (1-67) and 2 (0-8), respectively. Bowel Serosal Invasion (SI) was observed in 148 (97.4%) patients, Bowel Muscularis Invasion (MI) was noted in 44 (28.9%) and Full Bowel Wall Invasion (FBWI), including the mucosa, in 9 (5.9%) patients. Radical omentectomy was performed in all patients who had either primary or interval debulking in our center. Radical resection of the omental remnant, after incomplete cytoreduction in other centers, was performed in 47 patients.
Tumor metastatic omental implants were found in all specimens, but metastatic Omental Lymph Nodes (OLN) were found in 18 (20.7%) of the specimens.
After 2010, systemic Para-Aortic and Pelvic Lymphadenectomy (PAPLN) was performed in 58 patients (38.2%) and metastases were found in 31 (58.5%) of them. Metastatic Large Bowel Lymph Nodes (LBLN) were found in 77 (51.3%) patients. Metastatic Small Bowel Lymph Nodes (SBLN) were identified in 15/29 (50%) patients with segmental small intestinal resection. Also, metastatic Distal Lymph Nodes (DLN), above the level of the left renal vein (hepato-duodenal ligament, celiac artery, splenic vessels), were found in 13/20 (65%) cases.
Survival
Statistical Analysis of Survival Variables (P < .05 in bold italics).

aHazard Ratio (95% Confidence Interval).
bIndicates reference category.

Kaplan-Meier curve for overall survival.

Cumulative survival according to Large Bowel Muscularis Invasion (LBMI).

Recurrence-free survival according to Large Bowel Lymph Node (LBLN) invasion.

Cumulative survival according to performing a systemic Para-aortic and Pelvic Lymphadenectomy (PAPLN), when taking in consideration the en-block excision of involved bowel and its associated Large Bowel Lymph Nodes (LBLN).
Recurrence
Statistical Analysis of Recurrences Variables (P < .05 in bold italics).
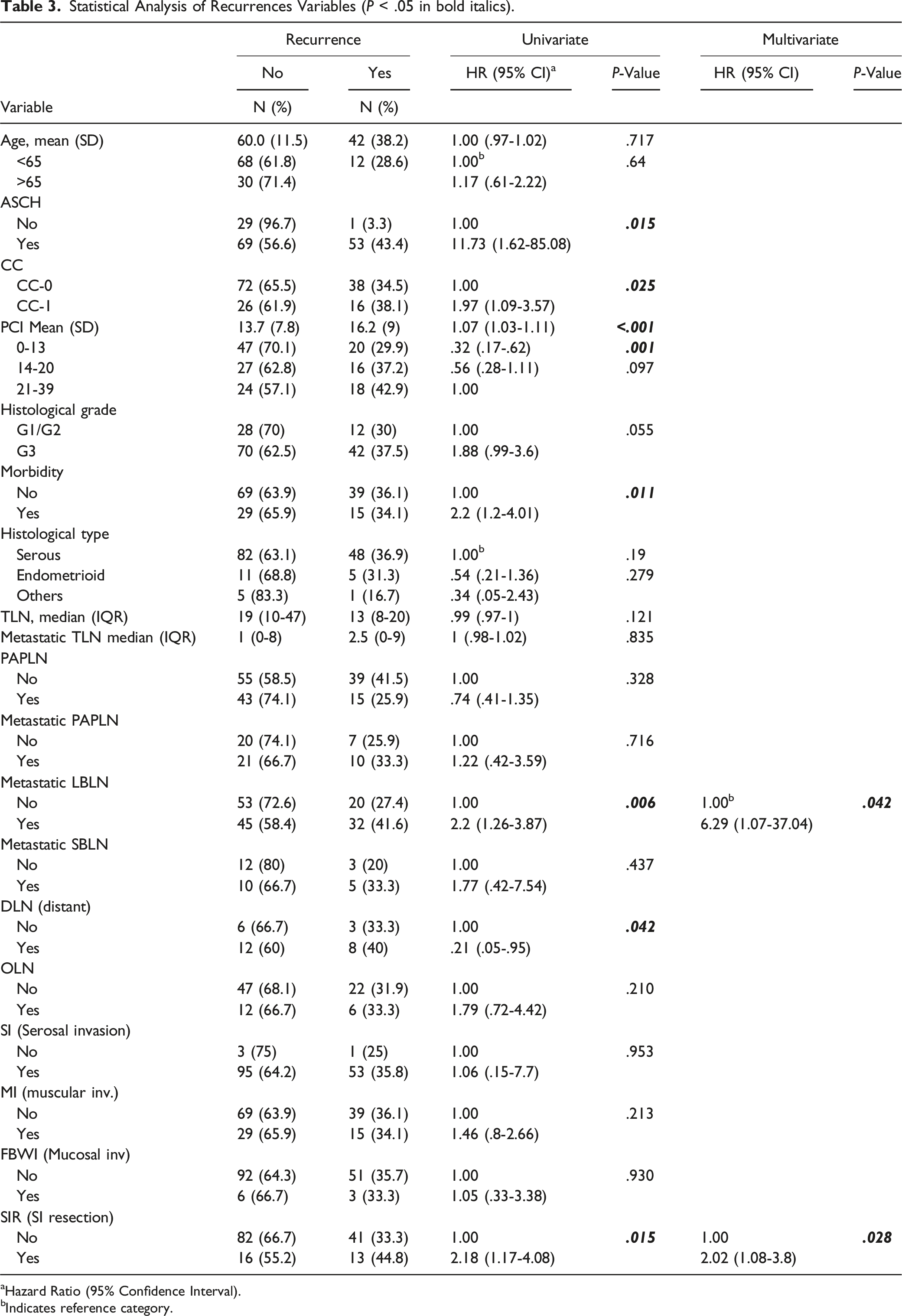
aHazard Ratio (95% Confidence Interval).
bIndicates reference category.
Abbreviation List.

Discussion
With more than 60% of patients diagnosed at FIGO stage III and IV, the aim of surgery is to remove all macroscopic peritoneal carcinomatous lesions, as it is widely accepted that complete cytoreduction, along with response to chemotherapy, is the most influential factor of survival.26,27
The discussion on the need and the extent of lymphadenectomy in advanced ovarian cancer has focused on systemic PAPLN, but only a few studies have pointed to the importance of the LBLN. 28
The need for PAPLN has been widely debated in ovarian cancer, although in serous carcinomas the rate of involvement is quite high (55-75%). 29 In early stages, the involvement ranges from 12-25%, and in advanced stages in 46-76%. In 1 prospective randomized trial, the disease-free survival was significantly improved with systemic PAPLN, but overall survival was the same in both arms. 14 The LION study did not show any survival benefit for patients undergoing complete PAPLN in the absence of bulky nodes, although micrometastases were identified in 56% in the lymphadenectomy group. In addition to considerable morbidity in the lymphadenectomy group, the authors concluded that routine extensive lymphadenectomy is not required. 15 In the present study, where Large Bowel Lymphnodes was also assessed, metastatic PAPLN were found in 58.7% of cases and a systemic PAPLN appeared to confer a survival benefit (HR: .47).
In peritoneal carcinomatosis due to ovarian cancer, the peritoneum is generally the first line of defense. 30 However, metastases can also occur through the lymphatic channels of the invaded intraperitoneal organs. It is well documented that LBLN may be involved even if only the bowel serosa has been invaded. Thus, the disease may follow the route of dissemination as if the primary site were a large bowel carcinoma.16-18 In our study, although the serosa of the large bowel was invaded in almost all resected specimens (95.8%), the muscular layers of the large bowel were involved in, approximately, one third (29.4%) of the specimens, while full bowel wall invasion was found only in 4.9% of the specimens. However, 51.3% of LBLN were metastatic and this was a strong indicator for disease recurrence.
Recto-sigmoid resection is the most frequently performed colonic resection when pelvic peritonectomy is involved. 31 The incidence of LBLN involvement varies greatly in the literature from 38%-73%. It has been suggested that LBLN invasion is an alternative metastatic pathway of ovarian carcinoma.16,32 According to the results of the present study, such a high incidence of metastatic LBLN (52%) may imply that a standard peritonectomy procedure is required for the surgical treatment of locally advanced ovarian cancer, which involves the en-block radical resection of the large bowel, with its whole mesentery. Data about the significance of bowel wall invasion are conflicting. FBWI has been identified as a prognostic indicator of survival and certain authors have identified a significant relation to survival.16,32 Bowel Muscularis Invasion (MI) has been shown to be an unfavorable prognostic indicator of survival in our study. Nevertheless, the contribution of the depth of the invasion of the large bowel and the nodal disease to overall survival still remains poorly defined and needs more investigation.
Metastatic LBLN have been shown to be a prognostic indicator of recurrence, implying that they may play a crucial role in the natural course of the disease. On the other hand, Bowel Muscularis Invasion (MI) has been identified as a prognostic indicator of survival. This confirms that, if the entire tumor load is not resected, the probability of recurrence is high. In locally advanced ovarian cancer, the pelvic peritoneum and the rectosigmoid are most frequently involved at initial diagnosis. At recurrence, the most frequently involved sites are the vaginal stump and the lower pole of the primary incision. 28 It has been reported that PAPLN may be infiltrated in continuity by the infiltrated LBLN. So, except for the direct metastases to the para-aortic and pelvic lymph nodes, through the anatomic lymphangio-vascular ovarian network, it is plausible that PAPLN metastases can occur through the metastatic LBLN. Therefore, in either case, the entire abdominal lymphatic network including the PAPLN and LBLN may need to be removed. The metastatic involvement of the lymph nodes of the hepatoduodenal ligament and the celiac axis is no longer considered a contraindication for cytoreduction. However, in such cases the survival appears poor, even if a complete cytoreduction can be achieved.20,29
The advanced patients’ age, extent of peritoneal carcinomatosis, completeness of cytoreduction and poor histological differentiation have all been identified in other similar studies, with or without HIPEC, as adverse factors for recurrence and survival.2,5,9,24
The administration of intraperitoneal chemotherapy remains a contentious issue, although it is well documented the direct cytotoxic effect and the increased drug concentration on the peritoneal surface. Despite the promising results of 3 prospective randomized trials with normothermic intraperitoneal chemotherapy and 1 prospective trial with HIPEC, the results of 10 more randomized HIPEC trials are eagerly awaited.6-8,13 A recent meta-analysis of 13 studies found that overall survival and progression-free survival in ovarian cancer patients having HIPEC were better compared to those that they did not have HIPEC (HR = .54 and .45, respectively). 33 There was criticism, though, because of the retrospective data, cohort imbalances, no uniform protocols and no consideration of the BRCA mutation status. As most of relevant studies on HIPEC have been conducted on patients treated at interval or secondary debulking, the results of an on-going randomized trial (OVHIPEC-2) on HIPEC at primary cytoreduction are eagerly awaited. The first results are awaited in 2026 and, in total, 538 patients are expected to be enrolled. The randomization will take place in the operating room and the regime will comprise of only cisplatin at 40-41°C for 90 min and at a dose of 100 mg/m2. 34
The morbidity of cytoreductive surgery is higher in elderly women, where the effects of age and the number of radical procedures have an additive effect on complication rates. Our in-hospital mortality and morbidity rates are comparable to previous publications.35-37 It is well established that delay of adjuvant chemotherapy, because of peri-operative morbidity, could adversely affect survival. 38 Our data confirm that older age, serious morbidity, and missing adjuvant chemotherapy may have a detrimental survival effect.
Although this is a retrospective study, its major strength is that all surgical procedures were performed by the same surgical team and in a standard fashion. The role of a dedicated team has been confirmed as a significant variable for improved survival with decreased morbidity.39-41 Certainly, ovarian cancer patients should be treated in high-volume dedicated centres.42,43 Finally, we confirm that our study conforms to the 302 STROBE guidelines. 44
Conclusion
The importance of involved bowel on disease recurrence and survival is clearly demonstrated in our series. Therefore, in all cases of macroscopically disseminated ovarian cancer in the pelvis, we believe that the en-block resection of the involved rectosigmoid bowel is mandatory.
Although, the recent LION study failed to demonstrate a survival benefit for patients undergoing a systemic lymphadenectomy, our data indicate that the Large Bowel Lymph Nodes frequently harbor metastatic disease, even when only the bowel serosa is infiltrated by tumor, and may play a crucial role in disease recurrence. Therefore, a radical excision of the involved bowel, with its whole mesentery and associated lymph nodes may confer a significant survival benefit for patients undergoing radical surgery for advanced ovarian cancer.
Supplemental Material
Supplemental Material - Prognostic Value of En-Block Radical Bowel Resection in Advanced Ovarian Cancer Surgery With HIPEC
Supplemental Material for Prognostic Value of En-Block Radical Bowel Resection in Advanced Ovarian Cancer Surgery With HIPEC by T. Panoskaltsis, C. Papadimitriou, N. Pallas, C. Karamveri, D. Kyziridis, C. Hristakis, V. Kiriakopoulos, A. Kalakonas, D. Vaikos, C. Tzavara and A. A. Tentes in Cancer Control
Footnotes
Author Contributions
TP and AT co-wrote the initial draft and final version of manuscript. Being in charge of the care of all patients, AT conceived and designed the study. NP, CK, DK, CH, VK, AK, and DV retrieved data from the patients’ files. CT performed the statistical analysis and interpretation of data. CP contributed to the medical care of patients and writing of the manuscript. All authors participated in the care of patients, critically revised and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability
Ethical Approval
The Ethics and Compliances Committee of Aretaieion Hospital approved the above study.
Informed Consent
All patients had signed an informed consent form for the use of their personal clinical details anonymously for scientific purposes.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.