
Abstract
Objectives
The associations between the neutrophil-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) with the responses of non-small cell lung cancer (NSCLC) patients receiving immune checkpoint inhibitors (ICI) and the NLR/PLR predictive potential were evaluated via meta-analysis.
Methods
A systematic review was conducted using the PubMed, Embase, and The Cochrane Library databases until October 2021. The relationship between NLR/PLR and overall survival (OS) and progression-free survival (PFS) was evaluated using pooled hazard ratios (HR). The relationship between NLR/PLR and overall response rate (ORR) and disease control rate (DCR) was assessed via pooled odds ratios (OR). Heterogeneity between studies, publication bias, subgroup and sensitivity analyses, trim and fill meta-analysis, and the contour-enhanced funnel plot were performed using the R software.
Results
A total of 44 (out of 875) studies met the eligibility criteria, providing a sample size of 4597 patients. Patients with a high NLR were statistically significantly associated with worse outcomes, including OS (pooled HR = 2.44; P < 0.001), PFS (pooled HR = 2.06; P < 0.001), DCR (pooled OR = 0.71; P < 0.001), and ORR (pooled OR = 0.33; P < 0.001). Similarly, a high PLR was associated with poorer outcomes in response to ICI drugs, including OS (pooled HR = 2.13; P < 0.001) and PFS (pooled HR = 1.61; P < 0.001).
Conclusion
High NLR and PLR were associated with a statistically significant reduction in the efficacy of ICI drugs in NSCLC patients. Thereby, it is possible to use NLR and PLR as potential and available biomarkers in the clinical practice to predict the outcome of ICI treatment in NSCLC patients.
Keywords
Introduction
Lung cancer is one of the most common cancers and the leading cause of cancer death worldwide, with the total number of new cases being 2.2 million and the number of deaths being 1.8 million in 2020,1,2 of which non-small cell lung cancer (NSCLC) accounts for about 85%. 2 The 5-year survival rate for the early stage is about 63%, and reduced to 35% for the locally advanced stage and only 7% for the metastasis stage. 2 Although surgery, radiation, and chemotherapy therapies have been significantly improved, the NSCLC survival prognosis remains low. 3 In recent years, immune checkpoint inhibitors (ICI) have significantly changed the treatment strategy of cancer in general and NSCLC in particular,4-9 especially in advanced stages.10,11 They are currently recommended as first-line treatment for cancer patients 12 and have become the mainstay of lung cancer treatment based on the improvement in survival.13-15 Though improved clinical outcomes, many patients are still poorly-responded. 16 Evaluating the efficiency of drugs before prescribing them is a crucial measure to reduce medical expenses, especially in developing nations with constrained budgets. Several validated prognostic biomarkers are available, such as PD-L1, tumor mutational burden, and the Mismatch repair systems.17-19 However, these markers had some limitations of invasive tests and the need to use histopathology or molecular genetic analysis.17-19 Therefore, finding non-invasive, effective, and low-cost markers to predict treatment outcomes is essential for the improvement of ICI therapeutic efficacy. Some index and scores have been evaluated for their diagnostic and prognostic value in NSCLC such as systemic immune-inflammation index (SII), lung immune prognostic index (LIPI) 20 and lung immune-oncology prognostic score (LIPS). 21
Several studies showed that two indicators namely neutrophil-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) which could be easily calculated through peripheral blood counts were related to cancer drug response.22-24 NLR and PLR dramatically increase in exitus patients and correlated to disease progression. 25 In particular, the associations between high NLR/PLR and poor treatment outcomes among NSCLC patients receiving ICI were reported in some studies with inconsistent results.26-28 A prior meta-analysis study was conducted by N. Zhang to solve this research gap, but the study systematically searched until 01/2020 and just focused on PD-1/PD-L1 inhibitors. 29
Hence, this comprehensive meta-analysis was conducted to assess the correlation between NLR/PLR and the effectiveness of ICIs in NSCLC patients. It also indirectly aimed to evaluate the predictive potential of these biomarkers.
Methods
Our research involved the secondary analysis of data collected from published studies and was not on human tissue/samples, so it does not need Ethics/Review board approval. This study was registered with INPLASY with the registration number INPLASY202470132. The study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement and completed PRISMA checklist (Supplemental PRISMA checklist).
Search Strategy
A systematic search was done until October 2021 on electronic databases including PubMed, The Cochrane Library, and EMBASE using the following search terms: (‘Lung cancer*’ OR ‘lung neoplasms*’OR ‘Non-Small-Cell Lung Carcinoma*’ OR ‘Non Small Cell Lung Carcinoma’ OR ‘Non-Small Cell Lung Carcinoma’ OR ‘Non-Small Cell Lung Cancer’ OR ‘Nonsmall Cell Lung Cancer’)
Inclusive and Exclusive Criteria
The studies were eligible for systematic review and meta-analysis if • NSCLC patients in the study were treated with ICI monotherapy; • The study explored the relationship between the pre-and/or post-treatment NLR/PLR with the ICI treatment outcomes (overall survival (OS), progression-free survival (PFS), overall response rate (ORR) and disease control rate (DCR)); • The relevant data for meta-analysis (the hazard ratio (HR), odds ratio (OR), and 95% confidence intervals (95% CI)) were reported or could be re-calculated; • The study design was cohort or case-control. • If two or more studies had the same population, the study with the largest sample size and the most current information would be selected.
The studies were excluded if they were • conference abstracts, case reports and case series, meta-analyses, or review articles; • non-human studies; • not written in English; • without full text.
Data Extraction and Study Quality Assessment
All data for the systematic review (the characteristics of studies) and meta-analysis (HR, OR, 95%CI, and data used to re-calculate) were obtained. The HR values calculated based on the univariate and multivariate analysis were collected, and HR values from multivariate analysis models were preferred.
The study quality assessment was done through the Newcastle-Ottawa Scale (the NOS scale) before being included in the meta-analysis based on three criteria: selectability (maximum 4 points), comparability (maximum 2 points), and output (maximum 3 points). Based on the NOS score, the article was divided into three quality criteria: poor quality (0-2), medium quality (3-5), and good quality (6-9). 30 The studies with NOS scores over six were included in the meta-analysis.
All processes of searching, screening, data extraction, and quality assessment were independently performed by two researchers (T.N.K.V. and C.T.T.N.). Any disparity was solved by a discussion with a third party (P.T.H.).
Data Collection and Statistics
A high NLR or PLR is a value that was higher than the cut-off value in each included study. A low NLR or PLR is a value that was lower than the cut-off value in each included study.
The associations between the NLR/PLR and OS and PFS were evaluated based on pooled HR and 95%CI; those of the NLR/PLR and ORR and DCR were evaluated based on pooled OR and 95%CI.
The heterogeneity between studies was assessed using the I2 and P-value of Cochran’s Q test. If there was no heterogeneity (I2 < 50% and Cochran’s Q test P-value >0.1), the fixed effects model would be applied; otherwise, the random effects model would be used.31,32
If there was heterogeneity between studies, a meta-regression analysis was performed to determine the cause of the heterogeneity. The analysis included variables such as study design, geographical area, sample size, time of NLR/PLR collection (time-point), NLR/PLR cut-off values, and HR origin (the univariate and multivariate analysis), from these, subgroup analysis was performed according to the likely sources of heterogeneity. 33
Publication bias was evaluated based on the asymmetry of the funnel plot and Egger’s linear regression test. 31 If there was an asymmetric funnel, the contour-enhanced funnel plot was used to determine the cause of the asymmetric. If publication bias was the cause, the trim and fill meta-analysis was done to identify publication bias and adjust results. 34
The leave-one-out analysis was performed to assess the effect of a single study by omitting one study each time and re-estimating pooled results. 35
Research using R version 4.2.3 software for analysis. A P-value <0.05 was considered statistically significant, except for the P-value of Cochran’s Q test.
Results
Study Selection and Characteristics
A total of 44/875 studies that met the inclusion and exclusion criteria were collected and analyzed. The screening process and reasons for exclusion are shown in Figure 1. PRISMA flowchart.
The characteristics of 44 studies are summarized in Supplemental Table 1. In general, studies evaluating the associations of NLR/PLR with the effectiveness of ICI treatment have been carried out and published since 2017, with most in Asia (n = 19), followed by Europe (n = 17) and America (n = 8). The mean age of NSCLC patients ranged from 57-71 years, with a high proportion diagnosed with nonsquamous carcinoma (52%–80%). The ICI drug evaluated in most studies was nivolumab (72%), followed by pembrolizumab (34%).
Regarding study design, ten were prospective studies, and 34 were retrospective studies. The sample size was relatively small, among which 26 studies with a sample size of less than 100 (59%) and 18 studies with a sample size greater than 100 (41%).
Thirty-nine studies provided HR values in the study, and five studies needed to re-calculate HR values from the reported data.36-39 Among eligible studies, 28 reported results relating to the NLR, 1 for the PLR, 40 and 14 reported results regarding both NLR and PLR. Concerning the time point of NLR collection, 41 studies collected the NLR pre-treatment, and seven post-treatment.37,41-46 Regarding the PLR, 13 studies recorded the PLR pre-treatment 47 and three with post-treatment data.42,45,46
The Association Between the NLR and the ICI Treatment Outcomes in NSCLC Patients
There were a total of 49 studies reporting the relationship between the NLR and the ICI treatment outcomes in NSCLC patients, in which the association between NLR and OS was reported in 35 studies, PFS in 26 studies, DCR in 6 studies, and ORR in 9 studies.
The Association Between the NLR and OS
Regarding the association between NLR and OS, the meta-analysis showed that NSCLC patients with high NLR had significantly worse OS (pooled HR = 2.44; 95% CI: 2.06-2.88; P < 0.001) (Figure 2A) compared to those with low NLR. Meta-analysis of the association between NLR and OS, (A) the forest plot; (B) the funnel plot; (C) the sensitivity analysis; (D) the contour-enhanced funnel plot; and (E) the trim and fill meta-analysis.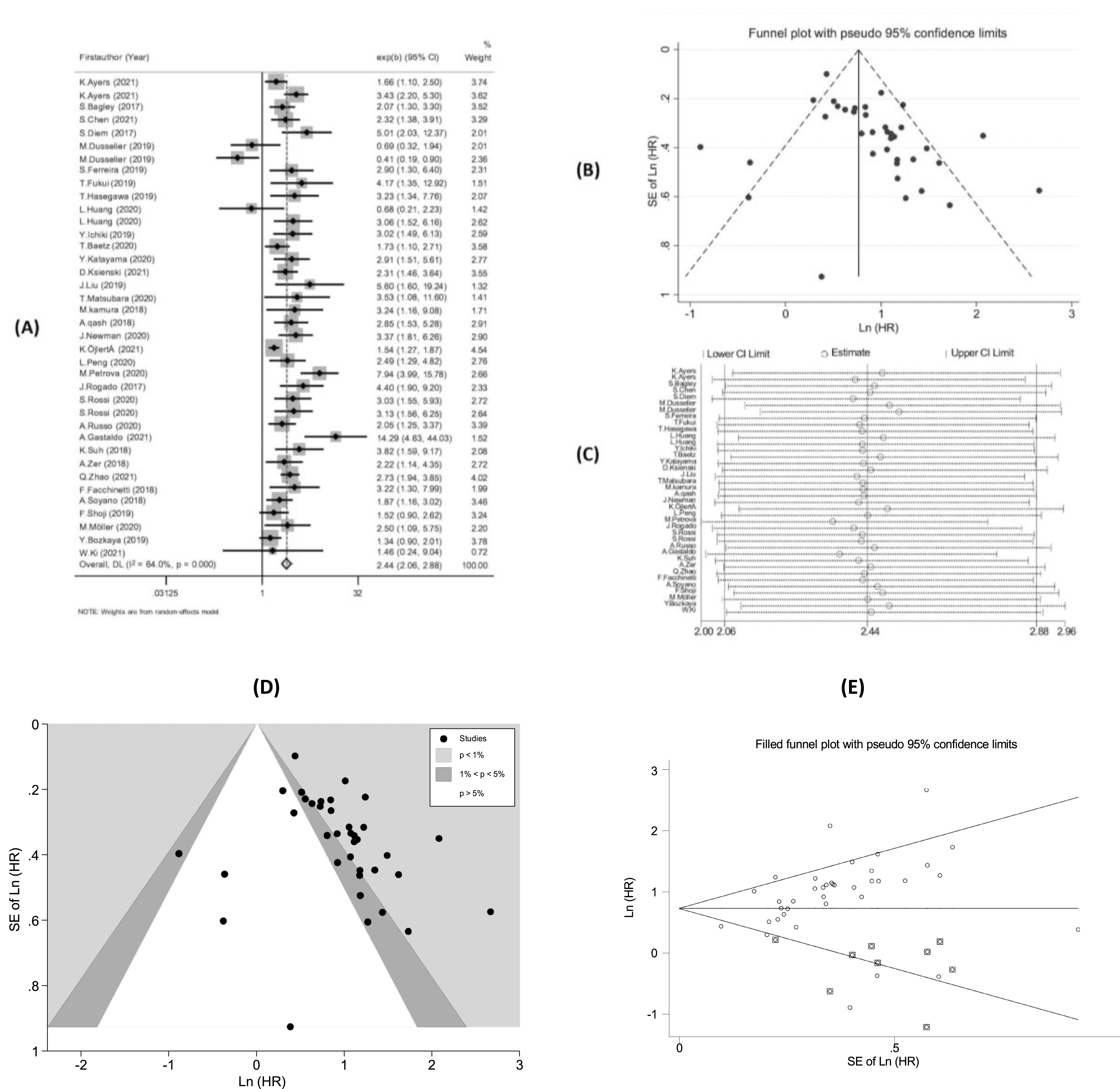
The studies had significant heterogeneity (I2 = 64.0%; P < 0.001) and had a high risk of publication bias (Figure 2B), (P-value of Egger’s test <0.001). The leave-one-out sensitivity analysis demonstrated that no study affected the baseline pooled result (Figure 2C). The contour-enhanced funnel plot (Figure 2D) indicated that the studies were distributed in all three areas but mainly right-skew, so the positive publication bias might be the leading cause. The trim and fill meta-analysis performed with the assumption of no publication bias (Figure 2E) showed that HR did not change compared to the baseline pooled HR (HR = 2.07; 95%CI: 1.75-2.45). The subgroup analysis showed statistically significant associations between NLR and OS in all groups (Supplemental Table 2).
The Association Between the NLR and PFS
Considering the association between NLR and PFS, the pooled result showed that NSCLC patients with high NLR had significantly poorer PFS (pooled HR = 2.06; 95% CI: 1.72 – 2.38; P < 0.001) (Figure 3A). Similarly, the studies had significant heterogeneity (I2 = 62.2%; P < 0.001) with a high risk of publication bias (Figure 3B, P-value of Egger’s test <0.001). The leave-one-out sensitivity analysis demonstrated that no study affected the baseline pooled result (Figure 3C). Meta-analysis of the association between NLR and PFS, (A) the forest plot; (B) the funnel plot; and (C) the sensitivity analysis.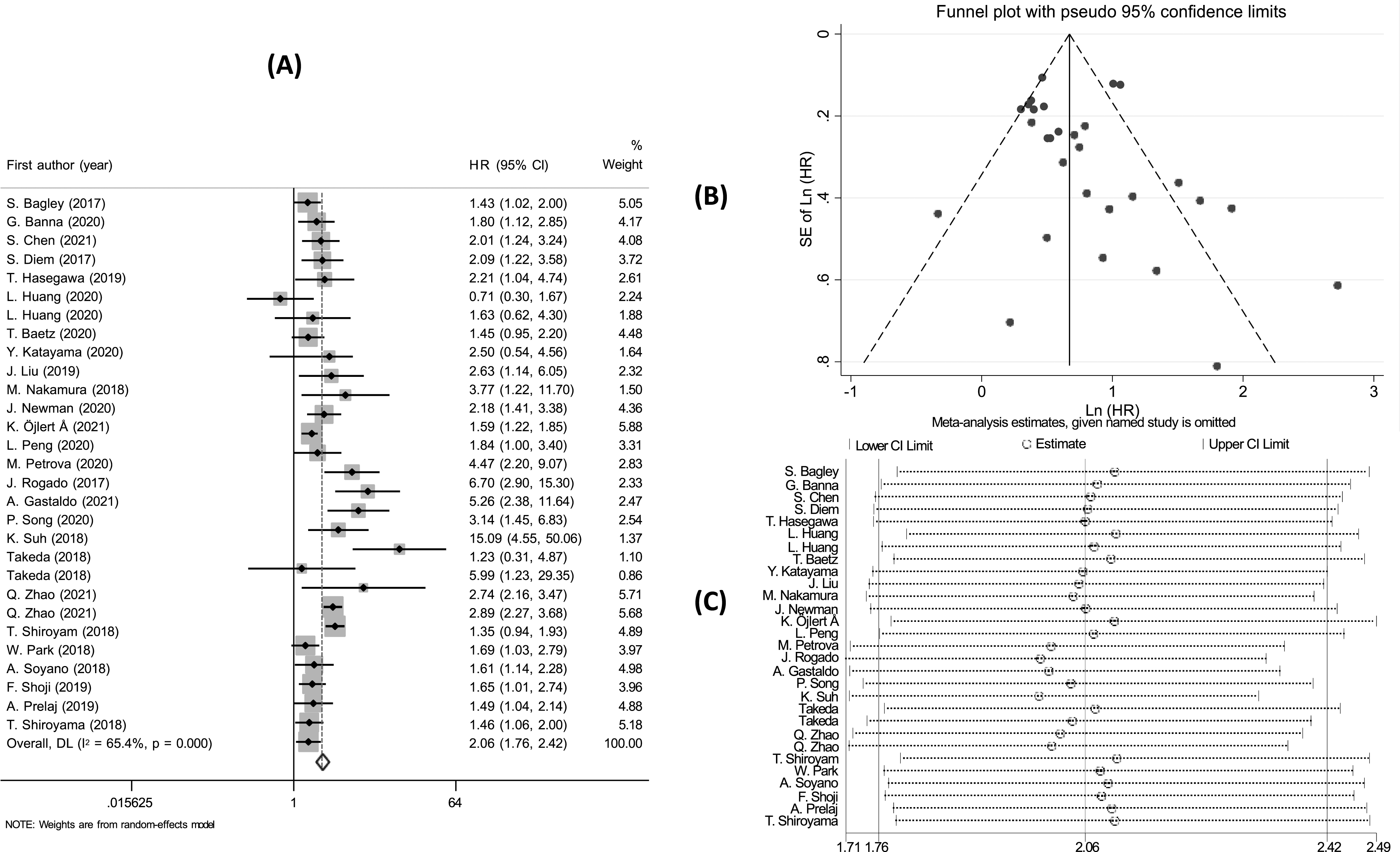
The cause might be publication bias (the studies were distributed in all three areas but mainly right-skew) (Supplemental Figure 1A). The HR did not change compared to the baseline pooled HR based on the trim and fill meta-analysis (Supplemental Figure 1B). The subgroup analysis indicated statistically significant associations in all subgroups (Supplemental Table 3).
The Association Between the NLR and DCR and ORR
The pooling analysis demonstrated that NSCLC patients with high NLR had lower DCR (OR = 0.33; 95%CI: 0.23-0.47; P < 0.001) (Figure 4A), and ORR (OR = 0.71; 95%CI: 0.57 – 0.89; P < 0.001) (Figure 4B). There was no heterogeneity between studies (I2 = 0.0%; P > 0.1) and no publication bias (P-value of Egger’s test >0.05). Sensitivity analysis indicated that no single study affected the results of the meta-analysis. Forest plot of the relationship between (A) NLR and DCR; (B) NLR and ORR.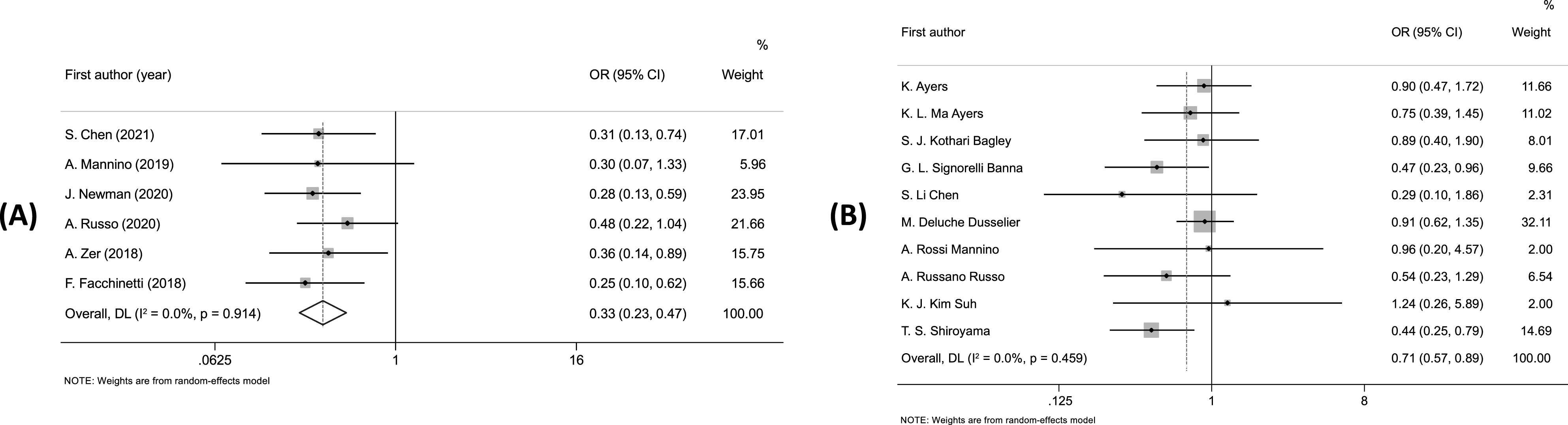
The Association Between the PLR and the ICI Treatment Outcomes in NSCLC Patients
A total of 23 studies assessed the relationship between PLR and the ICI treatment outcomes in NSCLC patients; in which an association between PLR and OS was reported in 13 studies, PFS in 10 studies. There was no association investigated between PLR with DCR and ORR.
The Association Between the PLR and OS
There was significant heterogeneity (I2 = 57.4%; P = 0.004), so the random effects model used with the pooling analysis showed that the high PLR led to significantly shorter OS (HR = 2.12; 95% CI: 1.62– 2.79; P = 0.002) (Figure 5A). The symmetric funnel plots (Figure 5B) and the P-value of Egger’s test over 0.05 indicated no publication bias. Sensitivity analysis revealed no study affected the pooled HR (Figure 5C). Meta-analysis of the association between PLR and OS, (A) the forest plot; (B) the funnel plot; (C) the sensitivity analysis; (D) the contour-enhanced funnel plot; and (E) the trim and fill meta-analysis.
The cause of publication bias (if available) might be from heterogeneity between studies (Figure 5D). The trim and fill meta-analysis assuming no publication bias, showed that HR did not change compared to the baseline pooled HR (HR = 2.12; 95%CI: 1.61-2.79) (Figure 5E).
The subgroup analysis showed statistically significant associations between PLR and OS in all subgroups, except for one with the time-point of post-treatment (HR = 1.22; 95%CI: 0.69-2.15) (Supplemental Table 4).
The Association Between the PLR and PFS
There was no heterogeneity between (I2 = 8.0%; P = 0.368), so the fixed effects model used with the pooled result showed that the patients with high PLR had a risk of poorer PFS (HR = 1.61;95% CI: 1.37 – 1.90; P < 0.001) (Figure 6A). The symmetrical funnel plots (Figure 6B) and the P-value of Egger’s test over 0.05 demonstrated no publication bias between studies. Sensitivity analysis revealed that no study affected the pooled result (Figure 6C). The subgroup analysis showed statistically significant associations between PLR and PFS in all subgroups, except for the time point of PLR measured in post-treatment (HR = 1.59; 95% CI: 0.93-2.74) (Supplemental Table 5). Meta-analysis of the association between PLR and PFS, (A) the forest plot; (B) the funnel plot; and (C) the sensitivity analysis.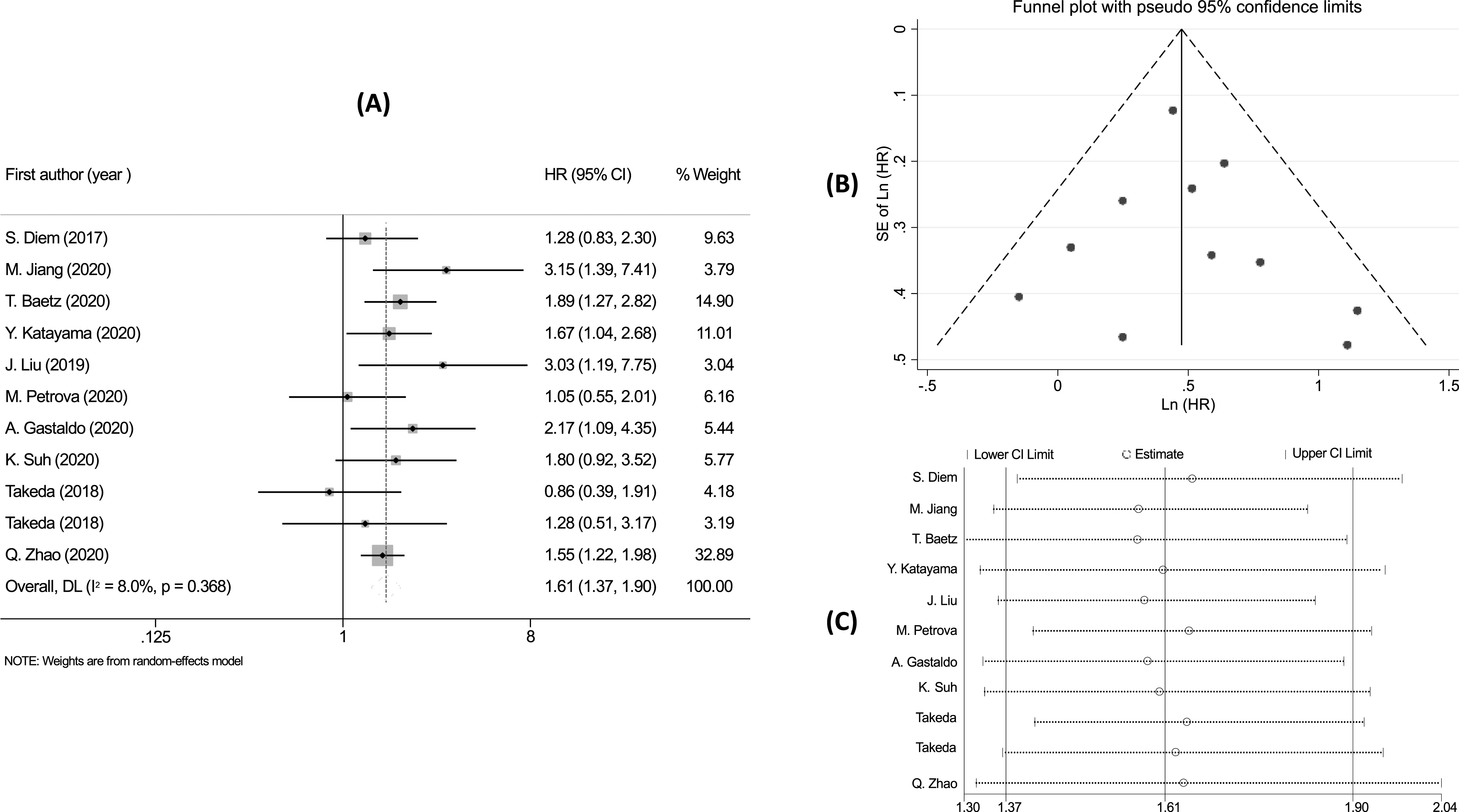
Discussion
NLR and PLR are known as novel biomarkers based on inflammation, which have been proposed as prognostic indicators for different cancers treated with ICI.22-24 However, the relationship between NLR/PLR and ICI treatment’s effectiveness in NSCLC patients remained inconsistent. The first meta-analysis study by N. Zhang investigating the prognostic role of NLR and PLR in NSCLC treated with ICI was done in 2020 but only mentioned PD-1/PD-L1 inhibitors in 1845 NSCLC patients from 21 studies. 48 Besides, the study of N. Zhang focused on just two outcome indexes, namely OS and PFS. 48 By extending the scope of research, this study synthesized the investigation results on the NLR of 4588 patients from 44 studies and that on the PLR of 1590 patients from 17 studies to analyze the relationship between NLR/PLR and ICI’s effectiveness in patients. Thus, our study included numerous studies and ICI drugs in the analysis, comprising CTLA-4 and PD-1/PD-L1 inhibitors. To our knowledge, this may be the first study to comprehensively report the association between NLR/PLR and the ICI’s effectiveness in treating NSCLC patients through the four outcomes (OS, PFS, ORR, and DCR).
The results of the meta-analysis showed that in the group of NSCLC patients receiving ICI drugs, high NLR related to poor treatment outcomes of ICI drugs, including a reduction in overall survival, progression-free survival, ORR, and DCR. Although there was heterogeneity in the studies, the meta-analysis results did not change much in the subgroup analysis. The results suggested that NLR might predict the outcome of ICI therapies in NSCLC patients.
Similarly, high PLR was associated with a significant reduction in OS and PFS in ICI-treated NSCLC patients. In addition, high PLR reduced ORR by 0.47 times and DCR by 0.35 times. In subgroup analysis, high PLR post-treatment was not strongly associated with poorer OS and PFS. The associations between PLR and ORR, and DCR were still limited and may be a potential topic for further studies. Thus, the pre-treatment PLR could play a predictive role in the ICI drugs’ effectiveness, thereby assisting in prescription decisions. However, due to the limited number of studies examining the connection between PLR and ORR and DCR outcomes, there is a need for additional research to establish more conclusive evidence.
There was much evidence that inflammation played an important role in affecting all steps in tumorigenesis, from tumor initiation to metastatic.49,50 It promotes tumor growth and activates oncogenic signaling pathways, 51 leading to poorer treatment outcomes in cancer patients. 52 Specifically, NLR is a marker reflecting the balance between two forces of the immune system, namely the innate immune response, which is responsible by neutrophils, and the adaptive immunity, which is functioned by lymphocytes. 53 An increase in NLR indicates a pro-inflammatory state with relative lymphocytopenia and leukocytosis, which reduces the ability of the body to prevent the local growth of tumors and their spread.54-56 These mechanisms indirectly suggested that patients were less likely to respond to the treatment. 57
Similarly, high PLR was associated with increased platelet counts and decreased lymphocyte counts. Interestingly, some studies showed that platelets can be educated by cancer cells to promote the secretion of cytokines and chemokines through surface proteins, including vascular endothelial growth factor, supporting tumor growth, angiogenesis, and metastasis. In addition, platelets protected tumors from immune surveillance and inhibited the activity of natural killer cells.58,59 Therefore, increased platelet counts as well as PLR were associated with resistance to cancer therapies such as chemotherapy or targeted therapy in various types of cancer. 60 The response of patients to Immune Checkpoint Inhibitors (ICIs) is heavily influenced by their immune and inflammatory statuses, thus showing significant correlation with NLR and PLR.
Our study provided evidence of the relationship between NLR/PLR and the effectiveness of ICI drugs in NSCLC patients and then proposed non-invasive, highly effective, and low-cost biomarkers to predict treatment outcomes. This information is particularly beneficial for clinicians in resource-limited treatment units, where patients may have limited access to molecular biomarkers. The essential point is determining the optimal cut-off value for each marker to be used in clinical settings. As shown in our systematic review in Supplemental Table 1, the cut-off value of around 5 is chosen for most of the included studies to predict poor responders. Meanwhile, regarding PLR, there was a diversity of cut-off values among studies, ranging from 119.2 to 441.8. Therefore, our study indicates that it would be easier to monitor the dynamic change of PLR during the therapy process for prognosis thereby enabling personalized medicine.
Our study had limitations similar to the prior meta-analysis study. 48 Firstly, the large-scale studies were retrospective and had unavoidable biases. Our findings showed a significant heterogeneity between studies. However, the random-effects model, where the studies had the same influence on the pooled analysis results, was used to report the final results. In addition, the leave-one-out and subgroup analysis were performed to calculate the actual influence of NLR/PLR on outcome indicators, and the results of these studies were consistent with the results of the previous pooled analysis. Secondly, differences in the characteristics of each study as well as differences in cut-off values of NLR, PLR, sampling time, and sampling method lead to high heterogeneity. Critical values used to define high and low NLR or PLR vary among included studies. Most studies (19/41) use an NLR cut-off of 5, but other studies employ values such as 2.8 or 6.5. Similarly, PLR cut-off values range from 144 to 400. Standardizing these critical values would enhance comparability of HR values across studies. Additionally, most of the studies collected focused on PD-1/PD-L1 checkpoint inhibitors (nivolumab, pembrolizumab, atezolizumab et al) so the relationship of NLR/PLR with the treatment outcome of NLR/PLR Other ICI drugs need to be further revealed.
Conclusion
Our study showed that high NLR/PLR were associated with a statistically significant reduction in the efficacy of ICI drugs in NSCLC patients. Thereby, it is possible to use NLR and PLR as potential and available biomarkers in clinical practice to predict the outcome of ICI treatment for NSCLC patients.
Supplemental Material
Supplemental Material - Predictability of NLR and PLR on the Effectiveness of Immune Checkpoint Inhibitors in Non-small Cell Lung Cancer patients: A Meta-Analysis
Supplemental Material for Predictability of NLR and PLR on the Effectiveness of Immune Checkpoint Inhibitors in Non-small Cell Lung Cancer patients: A Meta-Analysis by Cuc Thi Thu Nguyen, Tran Nguyen Khanh Van, and Phung Thanh Huong in Cancer Control.
Supplemental Material
Supplemental Material - Predictability of NLR and PLR on the Effectiveness of Immune Checkpoint Inhibitors in Non-small Cell Lung Cancer patients: A Meta-Analysis
Supplemental Material for Predictability of NLR and PLR on the Effectiveness of Immune Checkpoint Inhibitors in Non-small Cell Lung Cancer patients: A Meta-Analysis by Cuc Thi Thu Nguyen, Tran Nguyen Khanh Van, and Phung Thanh Huong in Cancer Control.
Footnotes
Author Contributions
All authors contributed to the study’s design and revised the manuscript; P.T.H supervised the study and revised the manuscript; T.N.K.V and C.T.T.N performed the data extraction and the statistical analysis, and drafted the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.