
Abstract
Objective
To investigate the relationship between the neutrophil-to-lymphocyte ratio (NLR) of patients with non-small cell lung cancer (NSCLC) and their risk of developing brain metastases after adjusting for confounding factors.
Methods
A retrospective observational study of the general data of patients with NSCLC diagnosed from January 2016 to December 2020. Multivariate logistic regression was used to calculate the dominance ratio (OR) with 95% confidence interval (CI) for NLR and NSCLC brain metastases with subgroup analysis. Generalized summation models and smoothed curve fitting were used to identify whether there was a nonlinear relationship between them.
Results
In all 3 models, NLR levels were positively correlated with NSCLC brain metastasis (model 1: OR: 1.12, 95% CI: 1.01-1.23, P = .025; model 2: OR: 1.16, 95% CI: 1.04-1.29, P = .007; model 3: OR: 1.20, 95% CI: 1.05-1.37, P = .006). Stratified analysis showed that this positive correlation was present in patients with adenocarcinoma (LUAD) and female patients (LUAD: OR: 1.30, 95% CI: 1.10-1.54, P = .002; female: OR: 1.52, 95% CI: 1.05-2.20, P = .026), while there was no significant correlation in patients with squamous carcinoma (LUSC) and male patients (LUSC: OR:0.76,95% CI:0.38- 1.53, P = .443; male: OR:1.13, 95% CI:0.95-1.33, P = .159).
Conclusion
This study showed that elevated levels of NLR were independently associated with an increased risk of developing brain metastases in patients with NSCLC, and that this correlation varied by TYPE and SEX, with a significant correlation in female patients and patients with LUAD.
Keywords
Introduction
Lung cancer is one of the most common fatal tumors in the world, 1 among which non-small cell lung cancer (NSCLC) accounts for 85% of all lung cancers, and the main pathological types (TYPE) are adenocarcinoma (LUAD) and squamous carcinoma (LUSC). Most NSCLC patients have metastatic disease, and brain metastasis is one of the most common metastatic sites, accounting for 20%. 2 Some studies have shown that patients with brain metastases from NSCLC have a poor prognosis, and even with whole brain radiotherapy, the overall survival of patients is only 3-6 months. 3 Currently, there is no clinical method for early detection of brain metastases in NSCLC, so finding a reliable and easily accessible marker for early identification of patients most likely to have brain metastases from NSCLC is important to prolong the survival of patients.
Chronic inflammation has a promotional effect on the development of tumors, either directly or indirectly through angiogenesis, cell proliferation, and metastasis, thus promoting the progression of lung cancer. 4 Neutrophils are the most abundant type of leukocytes in peripheral blood and play an important role in the body’s defense system. A study by Lehman et al. 5 pointed out that neutrophils play different roles in the tumor microenvironment, and activated neutrophils can both rely on cytotoxic effects to kill tumor cells and promote tumor progression and metastasis by stimulating angiogenesis and other pathways. Tumor-associated neutrophils (TANs) are associated with the recurrence and prognosis of many tumors and are negatively correlated with tumor prognosis and survival.6,7 Lymphocytes are the immune response cells of the body, which can directly participate in the body’s anti-cancer response and can inhibit the progression of malignant tumors by stimulating anti-tumor immune activity, and treatment-related lymphocytopenia is associated with poor prognosis of cancer. 8 Tumors are able to produce a large number of cell adhesion molecules (including integrin family and selectin family) causing intercellular or cell-extracellular matrix contact and binding, promoting lymphocyte extravasation, while chemokines recruit lymphocytes to the site of inflammation and play an important role in the immune response. 9 Hanahan et al. 10 showed that CD8+ cytotoxic T lymphocytes (CTLs), CD4+ Th1 helper T cells or NK cells with defective development or function can lead to a significant increase in tumor incidence.
Neutrophil-to-lymphocyte ratio (NLR) is an indicator of inflammation level that can be obtained from complete blood counts. NLR reflects the balance of the body’s inflammatory and immune responses, and its imbalance drives tumor progression and metastasis. When NLR is elevated, the neutrophil count is relatively increased and the lymphocyte count is relatively decreased, and the equilibrium is disrupted, thus promoting tumor progression. Tomita et al. 11 found in a retrospective study of 284 patients with NSCLC that patients with high NLR had a significantly lower 5-year overall survival compared to those with low NLR (47.06 vs 67.84%, P <.0001). Although a large number of studies have reported12-14 the role of NLR in the development of NSCLC, studies on the relationship between NLR and NSCLC brain metastasis are limited, and most of them did not consider the effect of confounding factors, did not do further subgroup analysis, and smooth curve fitting was also not done to explore whether there is a nonlinear relationship between the 2. The aim of this study was to investigate the relationship between NLR levels and NSCLC brain metastasis and to adjust for multiple potential confounding factors.
Methods
Study Population: A retrospective study was conducted on NSCLC patients who attended the Cancer Hospital of Anhui University of Science and Technology from January 2016 to December 2021. Inclusion criteria: 1. Clear diagnosis of NSCLC by histopathology or cytology and no previous history of other malignant tumors; 2. Diagnostic criteria for bone metastases: whole-body bone imaging was performed and confirmed by CT or MRI with typical imaging manifestations of bone metastases; 3. Diagnostic criteria for brain metastases: brain metastases were diagnosed by imaging (CT or MRI); 4. Patients had not received any treatment (note:radiotherapy, chemotherapy, targeted therapy, surgery, etc.) within the previous 15 days at the time of laboratory data collection. Exclusion criteria: 1. Those with incomplete clinical information, including AGE, SEX, TYPE, T, and N stage; 2. Pathological types other than LUAD and LUSC; 3. Patients with ≥2 sites of metastasis. Finally, 210 NSCLC patients were included, including 108 patients with non-metastasis, 56 patients with brain metastasis, and 46 patients with bone metastasis. In this retrospective study, we evaluated the study according to the principles of the Declaration of Helsinki and received approval from the Ethics Committee of Anhui University of Science and Technology (approval number: 201916). We obtained verbal consent from the patients themselves before collecting their information, and the data were anonymized and the patients’ personal data were protected. This study was reported in accordance with the STROBE guidelines. 15
Study Variables: A complete blood count was obtained on admission, with NLR as neutrophil-to-lymphocyte ratio, PLR as platelet-to-lymphocyte ratio, and LMR as lymphocyte-to-monocyte ratio. Age, SEX, TYPE, T, and N stage were considered as potential confounders and were adjusted in the analytical model.
Statistical Analysis: Continuous and categorical variables were expressed as mean ± standard deviation and percentage, respectively. Multivariate logistic regression was used to establish a model to detect the correlation between NLR levels and NSCLC brain metastasis. Model 1 does not adjust any variables; Model 2 adjusts for SEX and AGE; Model 3 adjusts for all potential confounders, including AGE, SEX, TYPE, T, and N stage. Further subgroup analyses were performed to investigate the relationship between the two in different populations. A weighted generalized summation model and a smoothed curve fitting method were used to explore the nonlinear relationships. All analyses were performed using the R package (version 3.4.3, http://www.Rproject.org) and EmpowerStats software (http://www. empowerstats.com). P<.05 was considered a statistically significant difference.
Results
Description of the Study Population.
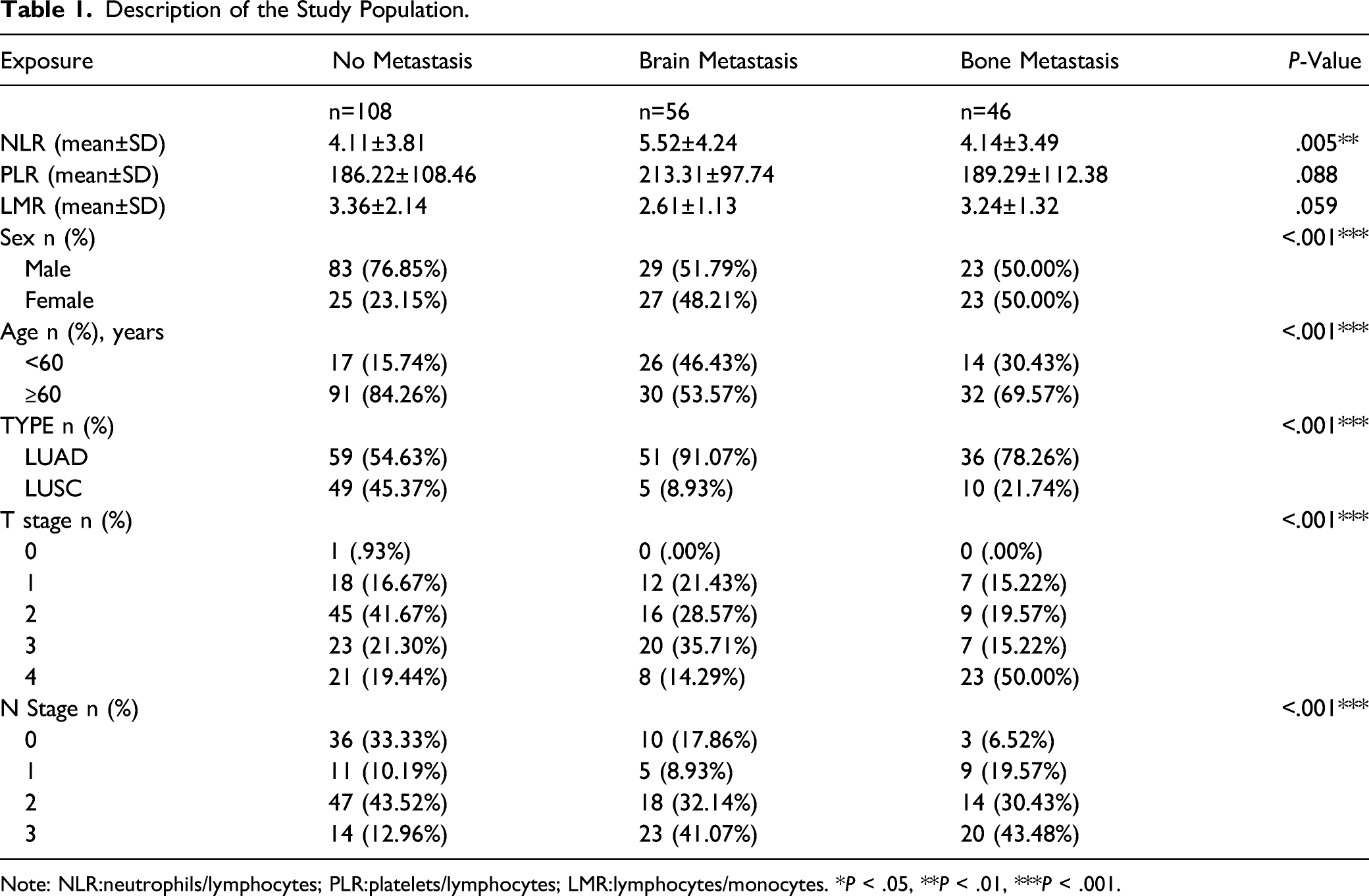
Note: NLR:neutrophils/lymphocytes; PLR:platelets/lymphocytes; LMR:lymphocytes/monocytes. *P < .05, **P < .01, ***P < .001.

Distribution of NLR in different groups. Note: *P < .05, **P < .01, ***P < .001, ns no significant difference.
Univariate Analysis of Risk Factors for Brain Metastasis in NSCLC.

Note: NLR:neutrophils/lymphocytes; PLR:platelets/lymphocytes; LMR:lymphocytes/monocytes. *P < .05, **P < .01, ***P < .001.
Relationship Between NLR Levels and Brain Metastasis of NSCLC.

Note: Model 1:no covariates were adjusted; Model 2: AGE and SEX were adjusted; Model 3: AGE, SEX, TYPE, T and N were adjusted. *P < .05, **P < .01, ***P < .001.
Subgroup Analysis of the Correlation Between NLR Levels and NSCLC Brain Metastasis.

Note: Model 1:no covariates were adjusted; Model 2: AGE and SEX were adjusted; Model 3: AGE, SEX, TYPE, T and N were adjusted. In the subgroup analysis stratified by SEX, AGE, TYPE, the model is not adjusted for the stratification variable itself. *P < .05, **P < .01, ***P < .001.

Relationship between NLR levels and brain metastasis in NSCLC. A. Each black dot represents a sample. The vertical coordinate .0 represents NSCLC unmetastasis, 1.0 represents NSCLC brain metastasis, and the solid line represents the distribution of NLR corresponding to each sample. B. Solid lines represent smoothed curve fits between variables, and the blue bars represent fitted 95% confidence intervals. Adjusted for AGE, SEX, TYPE, T, and N stage.

A. Relationship between NLR and NSCLC brain metastases, stratified by SEX. Adjustment for AGE, TYPE, T, N. B. Relationship between NLR and NSCLC brain metastases, stratified by TYPE. Adjustment for SEX, AGE, T, N.
Discussion
The main objective of this study was to investigate the relationship between NLR levels and brain metastasis in NSCLC. The results of the study showed that elevated NLR levels were significantly associated with NSCLC brain metastasis after adjusting for potential risk factors for the development of NSCLC brain metastasis (OR: 1.20, 95% CI: 1.05-1.37, P = .006). And further subgroup analysis showed that this positive association was statistically significant in patients with pathological type LUAD (OR: 1.30, 95% CI: 1.10-1.54, P = .002) and in female patients (OR: 1.52, 95% CI: 1.05-2.20, P = .026).
The occurrence of brain metastasis is a highly selective and multi-step process. Stephen Paget proposed the “seed-soil” theory in 1889, which suggested that tumor cells are the “seeds” leading to metastasis, while the microenvironment of metastatic organs is the “soil” leading to metastasis. The brain microenvironment includes stromal cells such as astrocytes, cytokines, vascular network, and some metabolic components, which can both promote and inhibit the occurrence and development of brain metastasis.16-18 The blood–brain barrier strictly controls the homeostasis of the internal environment of the central nervous system, and the presence of its tight junctions prevents most tumor cells from crossing the blood–brain barrier, but a small proportion of tumor cells and stromal cells accompanying tumor cells can destabilize the tight junctions through human vascular endothelial growth factor (VEGF) and matrix metalloproteinase (MMP), promoting the occurrence of tumor brain metastasis.19,20 Adequate blood supply is necessary for the formation of metastases by tumor cells crossing the blood–brain barrier, and tumor cells can obtain blood supply in the brain through many different mechanisms, such as lung cancer cells through angiogenic mechanisms. 21
Inflammation can serve as a potential biomarker, which can also contribute to alterations in the tumor microenvironment by altering the stromal cell renewal rate and the immunosuppressive capacity of polarized immune cells. 22 Neutrophils play a role in the distant metastasis of various malignancies, and in a mouse model of breast cancer, neutrophil depletion resulted in a significant reduction in lung and lymph node metastasis, and neutrophil depletion reduced early but not late multi-organ metastasis, suggesting that neutrophils promote multi-organ metastasis in the early stages of the metastatic cascade response. With neutrophil depletion, the CD8+ T cell effector phenotype was significantly enhanced, suggesting that neutrophils are able to promote metastatic spread of cancer cells by suppressing CD8+ T cells. 23 A study by Sung Jin Huh et al. 24 found that the presence of neutrophils was able to increase the number of melanoma cells retained in the lung, and that metastatic melanoma cells in the lung secreted IL-8 to attract neutrophils, which then interacted with melanoma cells to promote shear-resistant retention within the pulmonary circulation to enhance extravasation and subsequent development of metastasis under flow conditions. The decrease in lymphocytes may lead to a weakened immune response to tumors, thus promoting tumor progression and metastasis. 25 Inflammatory metrics and immune metrics based on neutrophil and lymphocyte counts have been used to predict the prognosis of various malignancies, including NSCLC. Ha H et al. 26 showed that low NLR was associated with better PFS, pre-treatment NLR was associated with poorer overall survival in non-small cell lung cancer, and post-treatment NLR was associated with poorer survival and recurrence rates in non-small cell lung cancer. This study showed that NLR levels were positively correlated with the risk of developing brain metastases in NSCLC patients (OR: 1.20, 95% CI: 1.05-1.37, P = .006), and in further subgroup analysis, each unit increase in NLR levels in LUAD patients was associated with a 30% increase in the risk of developing brain metastases in NSCLC patients. This may potentially be causally related to the fact that neutrophil depletion reduces matrix metalloproteinase 9 (MMP9) expression and decreases damage to the blood–brain barrier, and when NLR is elevated, neutrophils increase and release MMP9, oxygen radicals and other inflammatory mediators, which exacerbate blood–brain barrier damage and further increase blood–brain barrier permeability. 27
Female patients are more likely to develop LUAD, and it has been shown that gender is an independent prognostic factor for brain metastases from lung cancer. 28 In this study, a subgroup analysis with SEX stratification showed that in female patients, each unit increase in NLR was associated with a 52% increased risk of brain metastases, while there was no significant correlation in men. Similarly, it has been reported that 17beta-Estradiol induces vasodilation to increase tumor blood flow for brain metastasis by rapidly activating nitric oxide synthase (eNOS) via Src kinase in human endothelial cells and promoting nitric oxide (NO) release from endothelial cells via PI3K/Akt pathway. 29 On the other hand, estrogen can reduce the permeability of the blood–brain barrier by directly regulating the expression of the tight junction protein claudin-5. 30 There may be a potential synergistic effect between the 3 factors of altered tumor blood flow and blood–brain barrier permeability and brain metastatic lesions, resulting in mutual effects that promote the metastasis of tumor cells, the mechanisms of which may need to be explored in more basic and clinical experiments.
Compared with previous studies, the strength of the present study is that adjusting for more potential confounders (AGE, SEX, TYPE, T, and N stage), it was able to show more clearly the potential association between NLR and NSCLC brain metastasis. Stratified analysis was also performed to explore the correlation between NLR and NSCLC brain metastasis in different populations, and smoothing curve fitting was performed. However, there are some limitations of our study: 1. This study is a retrospective study and some selection bias may exist. 2. The findings need to be confirmed by prospective studies in the future. 3. The possibility of bias caused by other potential confounders that we did not adjust for remains.
Conclusion
Our findings suggest that elevated NLR levels are positively associated with NSCLC brain metastasis and that this association varies by SEX and TYPE, with significant correlation in female patients and LUAD patients. Our findings could improve our understanding of the relationship between NLR levels and NSCLC brain metastasis.
Footnotes
Author Contributions
HD and WJ: conception and design, and study supervision. HC, LY, ZJ, WW, WX, GJ, WQ, ZX, and LD: development of methodology, analysis and interpretation of data, and writing of the article. XJ, DX, and XY: review of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Natural Science Foundation of China (No. 81971483), the Collaborative Innovation Project of Colleges and Universities of Anhui Province (GXXT-2020-058) and Graduate Innovation Foundation of AUST (2020CX2083, 2020CX2084, 2021CX2124, 2021CX2125, 2021CX2126).
Ethical approval
This study was approved by the medical ethics committee of Anhui University of Science and Technology (NO.201916).