
Abstract
Background
The standard treatment for localized osteosarcoma is neoadjuvant chemotherapy before surgery, followed by adjuvant chemotherapy. Our aim was to report the rate of histopathological response to neoadjuvant chemotherapy for the treatment of extremity osteosarcoma in Vietnam.
Methods
We performed a retrospective study of stage II conventional osteosarcoma patients under 40 years-old who received MAP regimen as neoadjuvant chemotherapy at the Vietnam National Cancer Hospital between June 2019 and June 2022. Histopathological response was evaluated using the Huvos grading system, in which a good histopathological response was defined as a necrotic rate of 90% or more.
Results
Thirty-five eligible patients were included in the study. Male patients accounted for 65.7%, with a median age of 16 years (range, 8-38 years). Of the 35 cases, 31 were reported as stage IIB (88.6%). The femur and tibia were the most common sites in our study, accounting for 51.4% and 34.3%, respectively. The most common pathologic subtype was osteoblastic osteosarcoma (68.6%), followed by chondroblastic subtype (20%). After two cycles of MAP-regimen neoadjuvant chemotherapy, 28 of 35 patients (80%) underwent limb-sparing surgery. A good histopathological response was observed in 18 of 35 patients (51.4%). There were significant correlations between the duration of symptoms (P = 0.016), LDH (P = 0.001) serum levels at initial presentation, and ALP (P = 0.043) serum levels at initial presentation with histopathological response.
Conclusion
This retrospective study suggests a possible association between symptom duration, pre-treatment LDH levels, and pre-treatment ALP levels with histopathological response rates. Additional clinical investigations with long-term follow-up are needed to investigate survival outcomes in the Asian population.
Keywords
Introduction
Osteosarcoma is a common pediatric malignancy that occurs most commonly in children and young adults. It was considered a highly aggressive malignancy with a high incidence of micrometastases, accounting for more than 80% of patients at diagnosis.1,2 Neoadjuvant chemotherapy, radical surgery and adjuvant chemotherapy are standard treatments for advanced extremity osteosarcoma.3–5 The greatest advantage of neoadjuvant chemotherapy is the assessment of histopathological response to treatment, which is considered the strongest prognostic factor in sarcomas.6–8 When poor response to neoadjuvant chemotherapy in postoperative sample was reported (tumor necrosis of less than 90%), 9 the chemotherapy regimen for adjuvant therapy needs to be changed.10,11 However, there have been a few studies that have attempted to identify predictors of favorable histopathological response to neoadjuvant therapy.12,13 This has resulted in a lack of actual data on the effectiveness of neoadjuvant chemotherapy for osteosarcoma, particularly in the Vietnamese population. In developed countries, triple neoadjuvant chemotherapy combining high-dose methotrexate (HDMtx), doxorubicin, and cisplatin (MAP) is commonly used. However, due to the lack of experience with HDMtx and its toxicity in children, non-HDMtx-based therapies are widely used in our country. Recently, the concentration of plasma methotrexate has been tested in our hospital, the number of osteosarcoma patients receiving neoadjuvant MAP regimen has increased, but no published data have been found. Here, we performed a retrospective study to evaluate the histopathological response rate in Vietnamese patients with extremity osteosarcoma who received MAP regimen as neoadjuvant chemotherapy.
Patients and Methods
Patients and Treatment
Our retrospective study included consecutively selected patients with Enneking stage II osteosarcoma who were treated with neoadjuvant chemotherapy followed by surgery and adjuvant chemotherapy at Vietnam National Cancer Hospital from June 2019 to June 2022. The reporting of this study conforms to STROBE guidelines. 14 The inclusion criteria of patients in our study were: 1) Pathologically confirmed high-grade conventional osteosarcoma according to the WHO sarcoma classification 15 ; 2) Stage II according to the Enneking staging system for osteosarcoma 16 ; 3) Age ≤40 years; 4) Patients who underwent radical surgery after neoadjuvant chemotherapy and had their histopathological response evaluated according to Huvos grading system. 9 Exclusion criteria were: 1) Non-conventional subtypes of osteosarcoma, such as telangiectatic, fibroblastic, and small cell subtypes; 2) Prior chemotherapy and/or surgery; 3) Second cancer; 4) Allergic to any components of chemotherapy.
Clinical and paraclinical evaluations were performed before treatment, after two cycles of MAP neoadjuvant chemotherapy, after surgery, and after the addition of adjuvant chemotherapy. Clinical examination included a medical history, physical examination, and clinical symptoms. Baseline paraclinical tests included a complete blood cell count, liver and kidney function (ALT/AST, creatinine, and urea), serum LDH and ALP before and after neoadjuvant chemotherapy, and cardiac Doppler ultrasound. Primary tumor was evaluated on X-ray and magnetic resonance imaging (MRI). We used whole-body computed tomography (CT) scan to evaluate the stage. The size of the tumor in the greatest dimension and volume were measured with MRI at the time of diagnosis and before surgery.
All patients received neoadjuvant chemotherapy with the MAP regimen,
2
which includes cisplatin, doxorubicin, and methotrexate for 10 weeks, then had definitive surgery (Figure 1). On the weeks 1 and 6, cisplatin (60 mg/m2/day) was given over a 3-hour infusion on days 1 and 2; doxorubicin (37.5 mg/m2/day) was given on the first and second days. Additionally, pegfilgrastim was subcutaneously injected after 24 hours of chemotherapy. On the weeks 4, 5, 9, and 10, high-dose methotrexate (12 g/m2/day) was administered over a 4-hour infusion and intravenous leucovorin was started 24 hours after each methotrexate course at a dose of 15 mg/m2 every 6 hours, then leucovorin dose was altered based on the concentration of methotrexate on the following days until the concentration was less than 0.1 μM.17,18 Serum creatinine, urea, electrolytes, and plasma methotrexate concentration were evaluated at 24, 48, and 72 hours, or until the concentration was less than 0.1 μM. One week after the second cycle of neoadjuvant chemotherapy, the tumors were restaged using MRI. The patients then underwent definitive surgery. Surgical treatment was classified as either limb-sparing or amputation. The types of surgery were chosen based on the location of tumor and the disease extension, as well as the patient’s age. After surgery, patients were given four additional cycles of MAP adjuvant chemotherapy.
2
Protocol of treatment: MAP-regimen neoadjuvant chemotherapy followed by definitive surgery.
Outcomes and Evaluations
All patients were followed up until March 7th, 2024 with the primary endpoint being the assessment of the histopathological response to neoadjuvant therapy. The histopathological response was evaluated by an experienced pathologist (CVN), and was classified using the Huvos grading system, in which grades 1 and 2 corresponded to poor responses (<90% necrosis), and grades 3 and 4 corresponded to good responses (≥90% necrosis). 9 The secondary endpoints included the evaluation of disease-free survival, overall survival, changes of tumor volume using MRI, and the safety of chemotherapy. Disease-free survival (DFS) was defined as the time interval between the date of initiation of treatment and the date of the first replase at any site or death from any cause. Overall survival (OS) was defined as the time interval between the date of osteosarcoma diagnosis and the date of death from any cause or last follow-up. Tumor enlargement was defined as an increase by 4.5% or more compared to pretreatment tumor volume using MRI. 19 Adverse events (AEs) were graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events (version 4.03) (https://www.oncology.tv/SymptomManagement/NationalCancerInstituteUpdatesCTCAEtov403.aspx).
All patient details were de-identified. Information obtained from the medical records included patient characteristics (age, gender), time from symptom onset to initiation of neoadjuvant chemotherapy, clinical symptoms, tumor location, presence of pathological fracture, histopathology of the tumor at diagnosis, tumor characteristics (size and volume of tumor) on MRI at diagnosis and after chemotherapy, serum LDH, ALP levels, type of surgery, and histopathological respone to neoadjuvant therapy. Pre-treatment LDH levels >210 U/L were considered elevated. 20 Pre-treatment ALP levels >300 IU/L were considered elevated for patients aged <15 years, while levels >115.5 IU/L were considered elevated for patients aged ≥15 years. 21
Statistical Analysis
Data were managed and analyzed using the SPSS statistics software version 22.0 (IBM Corp., Armonk, New York). Categorical variables were represented as percentages and continuous variables were represented as a mean
Ethical Consideration
The study was approved by the Institutional Ethics Review Board of Hanoi Medical University (No.208/QD-DHYHN approval issued January 26, 2022) and Vietnam National Cancer Hospital (No.777/QD-BVK approval issued April 25, 2023). The study was evaluated by Hanoi Medical University under decision No.5314/QD-DHYHN dated November 03, 2022. The patient data were maintained with confidentiality, in compliance with the Declaration of Helsinki. Informed consent was waived because of the retrospective design of the study.
Results
Patients and Treatment
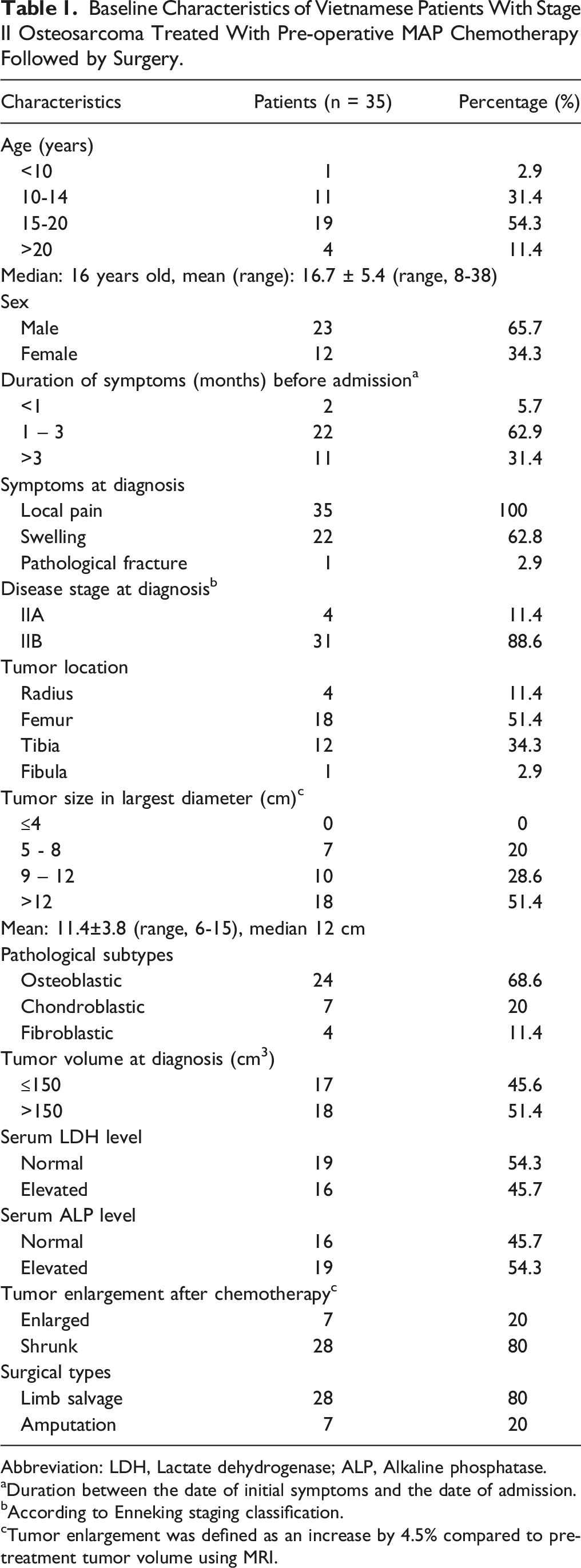
A total of 35 eligible patients under 40 years old with stage II osteosarcoma were included in our study from June 2019 to June 2022 at the National Cancer Hospital of Vietnam (Figure 2). The baseline characteristics, and treatment features are summarized in Table 1. Of the 35 patients in our study, the majority were male (65.7%) with a median age of 16 (range, 8-38 years). The pathological fracture was reported in one case. Stage IIB was reported in 31 of 35 cases (88.6%) according to Enneking classification. Femur and tibia were common sites of primary tumors in our study, accounting for 51.4% and 34.3%, respectively. Over a half (51.4%) of patients had tumor volume more than 150 cm3 with a median diameter of 12 cm. Osteoblastic osteosarcoma was reported in 68.6%, followed by chondroblastic subtype (20%). Elevated serum LDH and ALP levels at diagnosis were observed in 45.7% and 54.3%, respectively. Consort diagram of all newly diagnosed stage II osteosarcoma registered at the Vietnam National Cancer Hospital from June 2019 to June 2022. Baseline Characteristics of Vietnamese Patients With Stage II Osteosarcoma Treated With Pre-operative MAP Chemotherapy Followed by Surgery. Abbreviation: LDH, Lactate dehydrogenase; ALP, Alkaline phosphatase. aDuration between the date of initial symptoms and the date of admission. bAccording to Enneking staging classification. cTumor enlargement was defined as an increase by 4.5% compared to pretreatment tumor volume using MRI.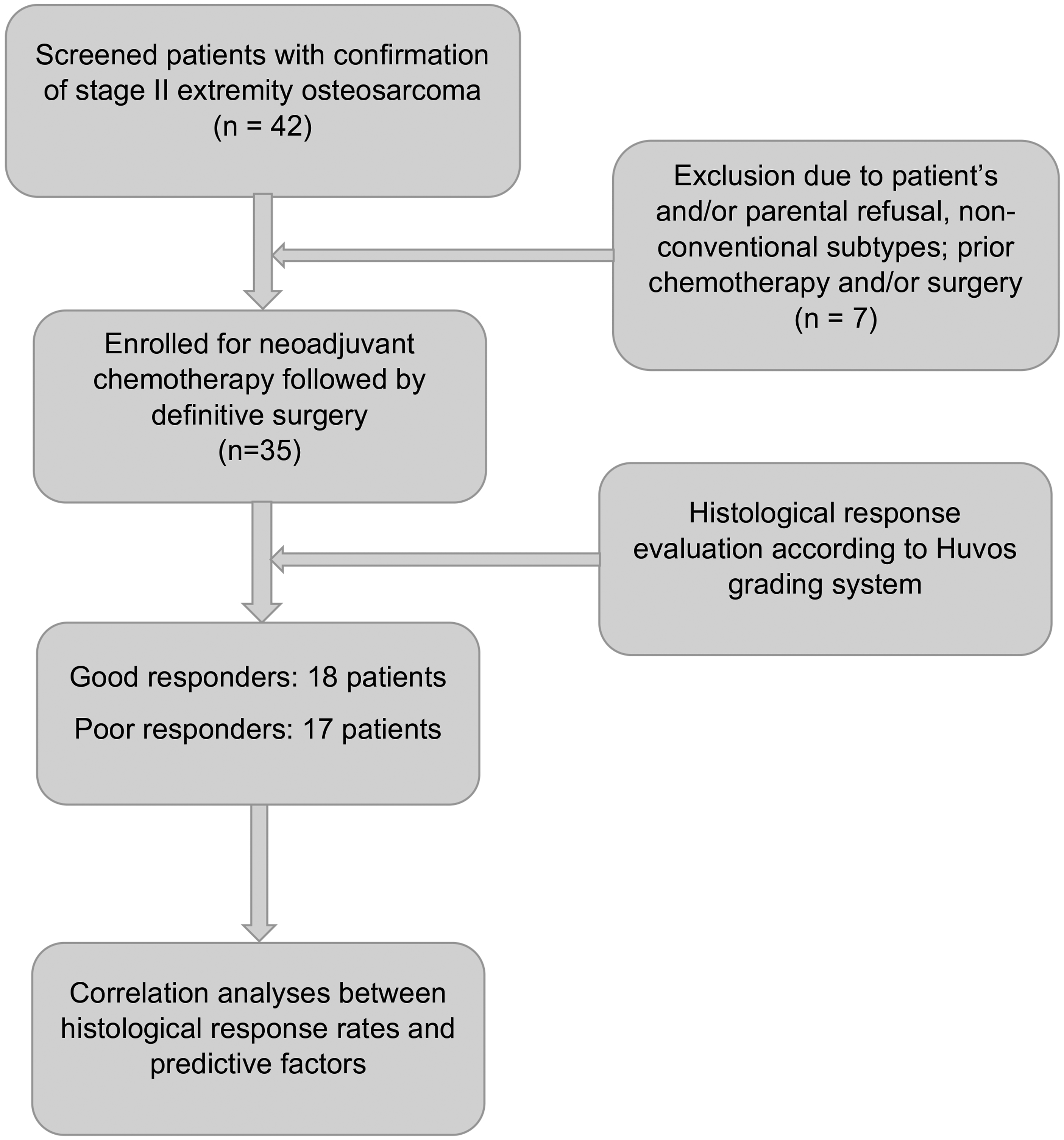
Efficacy Analysis
After completing two cycles of neoadjuvant chemotherapy, all patients underwent definitive surgery with clear surgical margins, and 28 of 35 patients (80%) underwent limb-sparing surgery. MRI revealed tumor enlargement in 7 of 35 patients after neoadjuvant chemotherapy. Our study showed that tumor volume decreased significantly after neoadjuvant chemotherapy, with a P-value of 0.001 (Supplemental Table 1). In the postoperative setting, all patients received four additional cycles of adjuvant chemotherapy.
Histological Response to Neoadjuvant Chemotherapy According to Huvos Classification.

Univariate Analysis of Huvos Response According to Clinical and Subclinical Features.
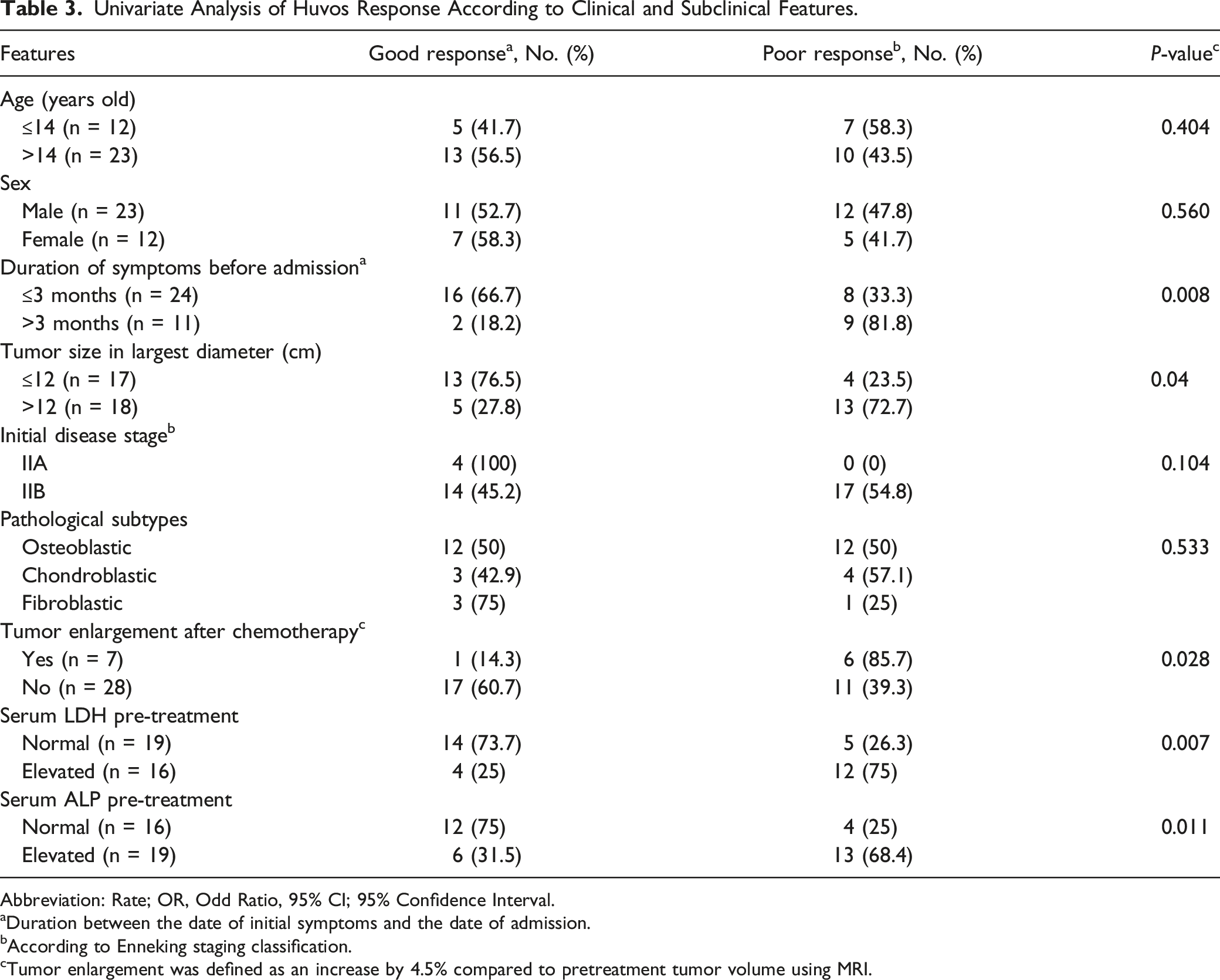
Abbreviation: Rate; OR, Odd Ratio, 95% CI; 95% Confidence Interval.
aDuration between the date of initial symptoms and the date of admission.
bAccording to Enneking staging classification.
cTumor enlargement was defined as an increase by 4.5% compared to pretreatment tumor volume using MRI.
Multivariate Analysis of Huvos Response According to Clinical and Subclinical Features Based on Logistic Regression Analysis Test.

Abbreviation: HR, Hazard ratio; CI, confident interval; LDH, Lactate dehydrogenase; ALP, Alkaline phosphatase.
aDuration between the date of initial symptoms and the date of admission.
At the last follow-up, there were seven relapses and four deaths in our study. The 3-year DFS and OS rates were 59.1% and 73.7%, respectively (Figure 3(A) and (B)). However, there was no statistically differences in terms of median DFS and OS between histopathological response subgroups (Figure 3(C) and (D)). Survival outcome of newly diagnosed stage II osteosarcoma registered at Vietnam National Cancer Hospital. (A) Disease-free survival (DFS); (B), Overall survival (OS); (C), Huvos subgroup according to DFS; D, Huvos subgroup according to OS.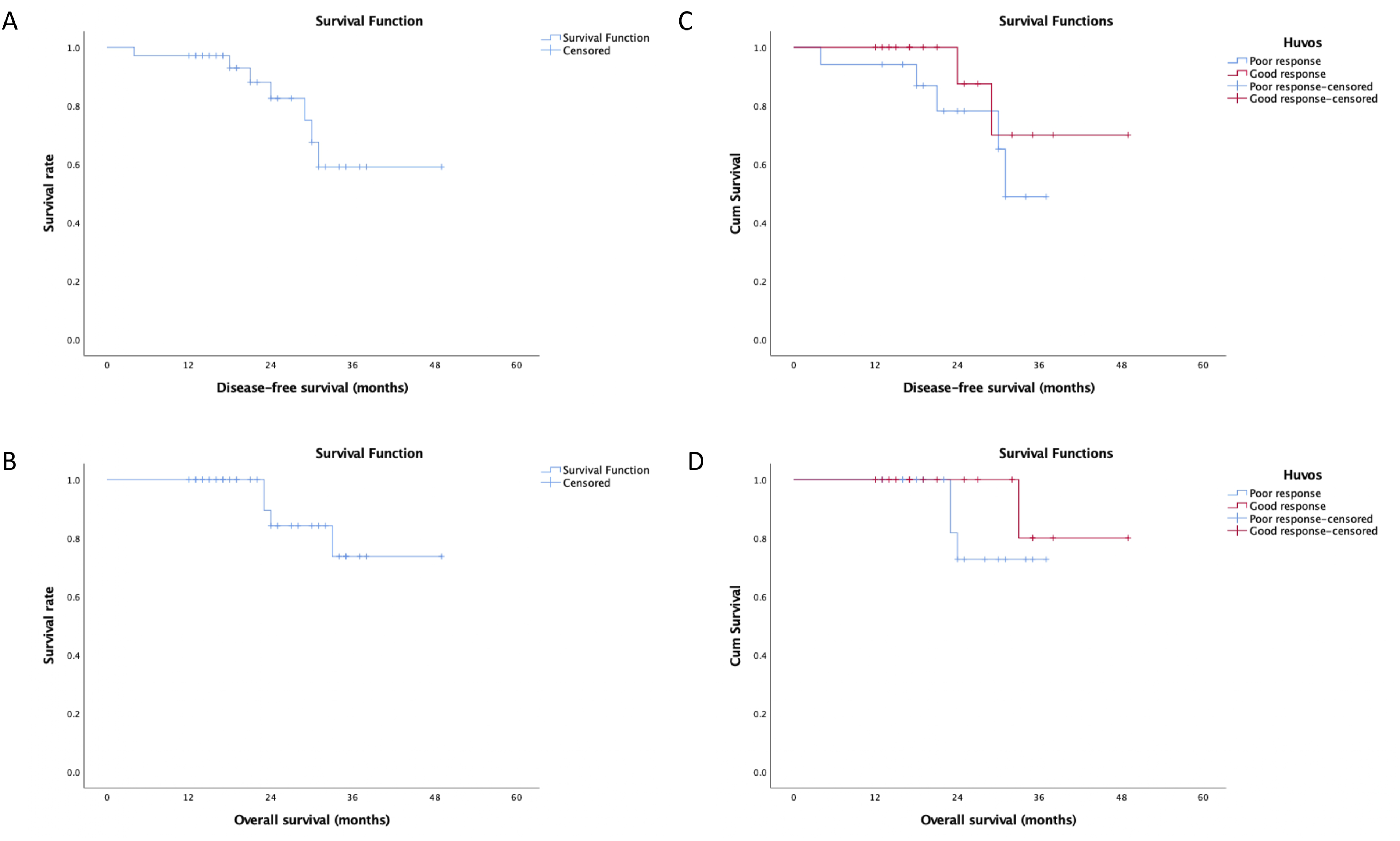
Toxicity
Adverse event (AE) profile of neoadjuvant MAP regimen presents in Supplemental Table 2. The frequent AEs of grades 3-4 were neutropenia (25.7%), followed by elevated liver enzymes (22.9%), mucositis (14.3%), and leucopenia (11.4%). None of the patients discontinued or were excluded due to unacceptable toxicity.
Discussion
In the past, amputation without reconstruction was the primary treatment modality of management of the extremity osteosarcoma in low- and middle-income countries due to lack of experience with the use of neoadjuvant chemotherapy and management of its toxicity in children. However, amputation caused physical and functional loss and decreased the quality of life, particularly psychological after surgery.22–24 One should keep in mind that osteosarcoma is one of malignant tumors with a high risk of micrometastases, accounted for over 80% in patients at the time of diagnosis.1,2 Neoadjuvant chemotherapy followed by local treatment has become standard strategies for many locally advanced malignancies.25,26 This is particularly true in osteosarcoma, the standard treatment is a combination of neoadjuvant chemotherapy, definitive surgery, and adjuvant chemotherapy.3–5 Neoadjuvant chemotherapy would control occult micrometastatic disease, tumor downstaging and increase opportunities of limb-salvage operation, particularly in difficult cases. The most important role of neoadjuvant chemotherapy was evaluating the histopathological respone to chemotherapy which was well-known as a strongest prognostic factor in sarcoma.6–8 Indeed, patients will receive different adjuvant regimens according to histopathological response.6,27 Several studies have demonstrated the effectiveness of neoadjuvant chemotherapy with various regimens in Asia populations. For instance, a study by J. Bajpai et al, 28 using a non-methotrexate-based regimen, reported a good response rate of 58% and the 5-year OS rate of 75%. Dharanikota A. et al Showed that survival was better among those who received neoadjuvant chemotherapy. 29
To our knowledge, this is the first retrospective study evaluating the histopathological response of neoadjuvant chemotherapy for the treatment of osteosarcoma in Vietnam, an Asian population not previously included in osteosarcoma trials. In our study, good responders were observed in 51.4%, particularly 3 patients (8.5%) had 100% of necrosis in postoperative samples. This result was similar to the report of EURAMOS – 1 study conducting 2260 osteosarcoma patients with a good response rate of 50%. 30 In the study by Bacci et al, 31 the group treated with triplet chemotherapy had a good response rate of 58.1%. A study by A. Suárez-Mattos et al conducted 41 osteosarcoma patients who received neoadjuvant MAP regimen, good response rate was only 36%, however, metastatic osteosarcoma was also included in this study.31,32 We noticed that good response rate tended to be higher in our study. It could be explained that our study conducted patients with stage II and conventional osteosarcoma subtypes only. Additionally, limb salvage was one of the main objective for the treatment of locally-advanced osteosarcoma of extremities as we mentioned above, 28 out of 35 patients (80%) underwent limb-salvage surgery in our study. This result is clinically meaningful and encouraging for our clinical practice.
Although histopathological response to neoadjuvant chemotherapy was considered as one of prognostic factors in many osetosarcoma studies, a few studies have been conducted to evaluate correlation between histopathological response and clinical features. In our study, the univariate analysis demonstrated that duration of symptom before admission (P = 0.008), tumor size (P = 0.04), tumor enlargement after neoadjuvant chemotherapy (P = 0.028), levels of pre-treatment LDH and ALP were associated with histopathological response rates in neoadjuvant setting. Prabowo Y reported that patients with complaints duration more than 3 months, tumor enlargment, and metastatic disease had a lower good response rate. There was non-significant difference in terms of tumor size at diagnosis, levels of pre-treatment LDH and ALP. However, using only doxorubicin/cisplatin regimen, this retrospective study also included mestastatic osteosarcoma patients, good responders were reported in 23.4%. 12
Conventional osteosarcoma, most common type of osteosarcoma, was divided to three subtypes based on histomorphologic features. 15 A study by Bacci et al included 1058 limb osteosarcoma patients, including 68.9% of osteoblastic subtype, 12.5% of chondroblastic subtype, and 9% of fibroblastic subtype. This study demonstrated that statistically higher good response rates in the osteoblastic subtype (relative risk: 2.3) and fibroblastic subtype (relative risk: 4.78), compared to the chrondroblastic osteosarcoma (P < 0.01). 31 In a study by Hauben et al, the highest rate of good responders was observed in the fibroblastic osteosarcoma patients (41%), followed by the osteoblastic group (29%), and chondroblastic group achieved only 9% good response (P = 0.01). In contrast with previous studies, our results showed a non-significant correlation between histologic subtypes and histopathological response rates. 33
Response Evaluation Criteria in Solid Tumours (RECIST) is often used for treatment response evaluation in oncology studies, 34 however, the use of this criteria in primary bone tumors was still controversial due to lack of association between radiologic response and histopathological response.35,36 Instead, tumor necrosis measured by MRI and maximum standard uptake value on positron emission tomography (PET) were more valuable in neoadjuvant setting. 37 Unfortunately, our study has a limitation that tumor necrosis evaluation on MRI was not reported. Indeed, there was no criteria for tumor change in radiologic images after neoadjuvant chemotherapy. A study by M. Hashimi et al 13 proposed a predictive scoring system including tumor change in size, in which no change was defined as ≤ 5 mm size change. A study by Seong-Hwan Moon et al, 19 tumor change, defined by a 4.5% change compared to pre-treatment tumor volume, was a prognostic factor of survival outcome. Our study showed a significant decrease of median tumor volume compared to pre-treatment volume with a P-value of 0.001. Additionally, tumor enlargement was significantly related to a lower good response rate in neoadjuvant setting (P = 0.028). Hashimi reported that tumor change was one of predictive factors for tumor necrosis in neoadjuvant setting, however, there was no results of further multivariate analysis.
Indeed, further multivariate analysis showed that there was a significant correlation between the duration of symptoms, serum levels of LDH and ALP at the time of the initial presentation with histopathological response in neoadjuvant setting. Our result was comparable to the study by Prabowo Y et al, in which gender, age, symptom duration, and tumor enlargement after chemotherapy were independent factors of histopathological response based on multivariate analysis. 12 There was a nonsignificant difference between histopathological response rates and level of serum LDH, and ALP at diagnosis. 12 Interestingly, our study first-time revealed the significant correlation between elevated levels of LDH and ALP at diagnosis and histopathological response rates. One should keep in mind that high pre-treatment LDH and ALP levels proved to be significantly correlating with poor OS and EFS in many studies.38–41
At the latest follow-up, 31/35 children were alive. There were 4 confirmed deaths and 7 relapses. Although in our study, 88.6% of patients were stage IIB, 51.4% were good responders with neoadjuvant chemotherapy, the 3-year DFS and OS reached 59.1% and 73.7%, respectively. We did not find any difference in survival outcomes between histopathological response groups (P > 0.05).
This study had some limitations. Firstly, the small sample size and retrospective nature of the study limited the power of the study and reduced the ability to compare the differences between subgroups by the statistical analysis. Further, our study showed the preliminary results of treatment response to neoadjuvant chemotherapy, and long-term survival outcomes have not been investigated. To reduce potential biases, we used rigorous selection criteria, focusing exclusively on patients diagnosed with Enneking stage II conventional osteosarcoma to enhance the homogeneity of our study population. In addition, all patients underwent evaluation and management discussions within a multidisciplinary team (MDT) setting to ensure comprehensive assessment and personalized treatment strategies for each patient. Further studies with more patients and long-term follow-up are needed to analyze prognostic factors in term of survival.
Conclusion
In conclusion, we observed comparable outcomes in patients with conventional osteosarcoma of extremities, compared to previous studies. This retrospective study suggests that there may be a correlation between symptom duration, levels of pre-treatment LDH, and ALP with histopathological response rates. Further clinical studies with a larger sample size are necessary to investigate long-term survival outcomes for the Asian population.
Supplemental Material
Supplemental Material - Histopathological Response to Neoadjuvant Chemotherapy in Patients With Enneking Stage II Conventional Osteosarcoma of Extremities: A Retrospective-Single Institution Study in Vietnam
Supplemental Material for Histopathological Response to Neoadjuvant Chemotherapy in Patients With Enneking Stage II Conventional Osteosarcoma of Extremities: A Retrospective-Single Institution Study in Vietnam by Kien Hung Do, Tai Van Nguyen, Trang Thu Hoang, Thanh Cam Do, Phuong Dac Phan, Chu Van Nguyen, Van Le Quang in Cancer Control
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.