
Abstract
Objectives
Neoadjuvant endocrine therapy (NET) has demonstrated efficacy in postmenopausal patients with hormone-responsive and HER2-negative breast cancer. However, few data are available on NET in premenopausal women. This trial was designed to compare the effectiveness of neoadjuvant chemotherapy (NCT) with NET in premenopausal patients with hormone-responsive, HER2-negative, and lymph node-negative breast cancer.
Methods
In this prospective, randomized study, premenopausal patients with hormone-responsive, HER2-negative, and lymph node-negative breast cancer were recruited. The enrolled patients were randomly assigned (1:1) to receive either NCT or NET with goserelin and tamoxifen, followed by goserelin and anastrozole. The primary purpose was to evaluate the non-inferiority of NET to NCT using a clinical response rate assessed by ultrasound.
Results
A total of 68 patients were assigned to receive either NCT (n = 31) or NET (n = 37). The clinical response rate was 16.1% for NCT and 35.1% for NET (estimated difference 19.0%, 95%CI: −1.1%-39.1%, non-inferior P = 0.002). The rates of breast-conserving surgery were not significantly different between the NCT and NET groups (90.3% vs 83.8%, P = 0.494).
Conclusions
A 35.1% clinical response rate was observed in premenopausal patients after NET. However, this study was underpowered to conclude the non-inferiority of NET to NCT because of its early closure.
Trial registration
ClinicalTrials.gov NCT02535221.
Keywords
Background
Several prospective randomized controlled trials have demonstrated that women undergoing breast-conserving therapy (BCT) for early-stage breast cancer have equivalent survival outcomes to those undergoing mastectomy.1-7 Some retrospective studies demonstrate that patients who undergo BCT have improved breast cancer-specific survival compared with patients who undergo mastectomy alone or mastectomy with radiation for early-stage invasive ductal carcinoma.8-10 This evidence has led to the widespread use of BCT as a treatment for early-stage breast cancer over the past two decades.
The key points of successful BCT include the resection of breast cancer and the maintenance of an aesthetically appropriate breast shape. Therefore, if the volume ratio of the tumor to the breast is too large, the opportunity for BCT decreases.
Compared to patients in European and American countries, those in China have relatively larger tumors and smaller breasts. Therefore, it is important for Chinese patients that tumors downsized by neoadjuvant treatment facilitate breast-conserving surgery.
Multiple studies on both chemotherapy and endocrine therapy have shown that neoadjuvant treatment can increase the likelihood of breast-conserving surgery(BCS).11-14 In several phase III neoadjuvant chemotherapy (NCT) studies, the conversion rate from BCS-ineligible to BCS-eligible patients ranged from 43.0% to 53.0%.13,15,16 Neoadjuvant endocrine therapy (NET) has been mostly studied for postmenopausal breast cancer patients in comparison with tamoxifen and aromatase inhibitors. The ASCO guidelines recommend neoadjuvant endocrine therapy with an aromatase inhibitor to increase locoregional treatment options for postmenopausal patients with HR-positive/HER2-negative disease. 17 However, about the premenopausal patients, there is no evidence that neoadjuvant endocrine therapy is suitable for this type of patient. Few clinical trials have compared NCT with NET in HR-positive/HER2-negative premenopausal patients with lymph node-negative breast cancer.
We hypothesized a non-inferior clinical response rate of NET compared with NCT. We reported a phase II clinical trial to compare the response between NCT and NET in premenopausal women with hormone-responsive, HER2-negative, and lymph node-negative breast cancer.
Methods
Study Design
This was a prospective, single-center, phase II randomized trial to test the hypothesis that neoadjuvant endocrine therapy is non-inferior to neoadjuvant chemotherapy in premenopausal patients with hormone-responsive, HER2-negative, lymph node-negative breast cancer. The research protocol was examined and approved by the Ethics Committee of Beijing Cancer Hospital (2015YJZ06) and conducted in accordance with the Declaration of Helsinki. This trial was registered at ClinicalTrials.gov (NCT02535221). The reporting of this study conforms to the CONSORT statements. 18
Patients
Eligible patients included premenopausal women aged 35-50 years with untreated, histologically confirmed, hormone-responsive, HER2-negative, and lymph node-negative primary invasive breast cancer (cT2-3N0M0), without other tumor or unstable complication or uncontrolled infection, no contradiction for the third-generation aromatase inhibitors, luteinizing hormone-releasing hormone analog, and chemotherapy. Lymph node negativity was confirmed using sentinel lymph node biopsy before the start of enrollment. Hormone response was defined as estrogen receptor-positive and/or progesterone receptor-positive, and ≥50% positive cells by immunohistochemistry staining. Exclusion criteria included prior chemotherapy or endocrine therapy, uncontrolled cardiac disease or infection, metastatic disease by pathological or radiological diagnosis, contraindication to neoadjuvant treatment, other malignant diseases (except cervical carcinoma treated in situ or adequately treated basal or squamous cell carcinoma of the skin), and other situations not suitable for the research: psychological disease, mental disorder, social problems. Premenopausal status was defined as having a regular vaginal bleeding history at the time of diagnosis. Written informed consent for participation in the trial should be obtained from all participants before enrollment.
Procedures
The random allocation sequence was generated by the computer (with a set number of seeds, the random sequence can be reproduced). Patients were randomly assigned (1:1) to receive either epirubicin and cyclophosphamide (100 mg/m2 epirubicin plus 600 mg/m2 cyclophosphamide intravenously) every 3 weeks for 4 cycles, or goserelin acetate 3.6 mg every 4 weeks with tamoxifen 20 mg daily for the first 4 weeks, followed by goserelin acetate 3.6 mg every 4 weeks with anastrozole 1 mg daily for 12-16 weeks. During treatment (every 6 weeks for the NCT group and every 4 weeks for the NET group), ultrasound measurement of the tumor size was performed.
The baseline examination before randomization included complete blood count, biochemical tests, chest radiography, and abdominal ultrasound. The primary breast lesions and axillary lymph nodes were evaluated by clinical examination, mammography, and ultrasound before enrollment.
Outcome
The primary outcome was the clinical response rate after neoadjuvant treatment, as determined by ultrasound measurements. A clinical response includes either a complete response (CR) or a partial response (PR), according to the WHO criteria. 19 The secondary endpoints were the pathological response by the Miller-Payne (MP) grading system and the rate of breast conservation surgery. 20
Statistical Analysis
The non-inferiority margin was defined as the lower limit of the two-sided 95% confidence interval (CI) for the difference in response rates between groups greater than −10%. Based on unpublished data from our center, the clinical response rate was 46.4% in the neoadjuvant chemotherapy group and 55.6% in the neoadjuvant endocrine treatment group. Using the PASS11 calculation, the minimum sample was 106 per treatment group to provide a power of 80% to demonstrate the non-inferiority of neoadjuvant endocrine therapy to neoadjuvant chemotherapy, allowing for a dropout rate of 10% in each group; Thus, a total of 234 patients were required in 3 years of enrolment.
The trial was closed early because of low accrual rates, and 68 patients were enrolled until March 10, 2022, the post-hoc power is 0.807. To compare the two groups, the t-test for mean differences and the chi-squared test for frequencies were used. A 2-sided P < .05 was considered statistically significant. All analyses were conducted using the SPSS software (version 22.0; IBM, Armonk, NY, USA).
AstraZeneca provided funding for this study. The funder of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the manuscript.
Results
Between July 2015 and March 2022, 68 patients were enrolled in our center. Thirty-seven patients were assigned to the NET group (with goserelin and tamoxifen, followed by goserelin and anastrozole) and 31 to the NCT group. Two patients who were randomized to receive chemotherapy did not receive chemotherapy but received neoadjuvant endocrine treatment. Another two patients in the NCT group received neoadjuvant endocrine treatment after chemotherapy because of the COVID-19 pandemic (the operation room was unavailable for months) (Figure 1). All the patients were included in the Intention-To-Treat (ITT) analysis of the primary endpoint. The baseline characteristics were generally balanced between the treatment groups. The median age of the patients in both treatment groups was 43 years (range, 36-50 years). All the patients were premenopausal (Table 1). CONSORT Diagram. Patients Baseline Tumor Characteristics. MRI, Magnetic Resonance Imaging.

Summary of Ultrasound Clinical Response.

CR complete response, PR partial response, SD stable disease, PD progressive disease.
The Breast Surgery and MP Grading System.
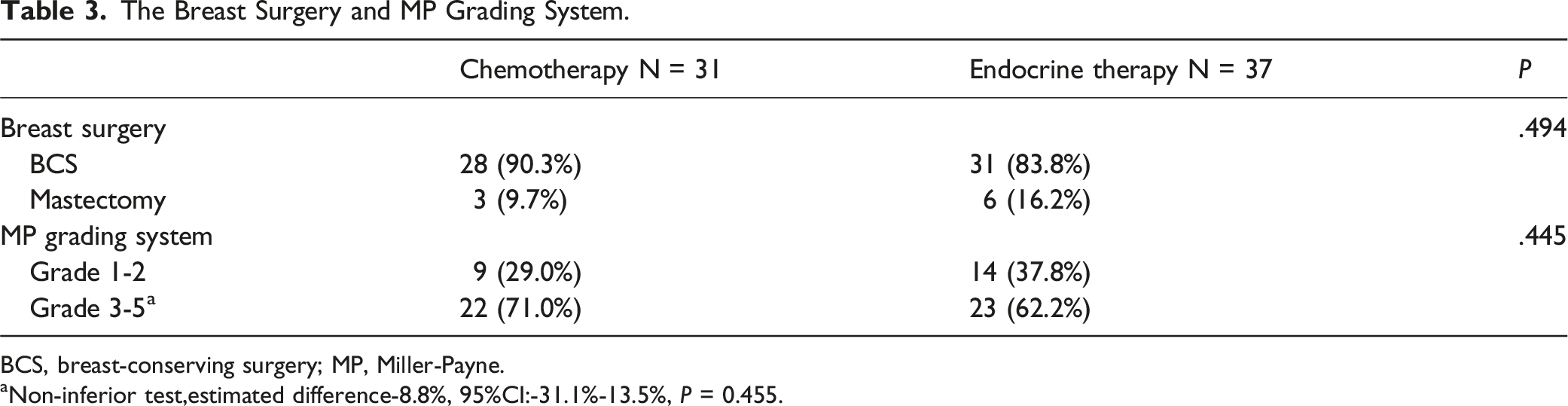
BCS, breast-conserving surgery; MP, Miller-Payne.
aNon-inferior test,estimated difference-8.8%, 95%CI:-31.1%-13.5%, P = 0.455.
The Success Rate of BCS.

BCS, breast-conserving surgery.
Discussion
This trial showed a 35.1% clinical response rate of NET (with goserelin and tamoxifen, followed by goserelin and anastrozole) in premenopausal patients with hormone-responsive, HER2-negative, lymph node-negative breast cancer. This suggests that NET in premenopausal women has an activity by downstaging tumors. Because of early closure, the non-inferiority of NET to NCT is underpowered.
For hormone-responsive, HER2-negative breast cancer, pCR, which is the definite response criterion in neoadjuvant therapy, is low and is not a surrogate endpoint for survival. 21 Only two (6.5%) patients in the NCT group showed breast pCR in our study. The data were 5.7% in another randomized phase III study after 24 weeks of NCT. 22 The MP grading system is an alternative method for assessing pathological responses after NCT. Our study showed no significant difference in grading 3-5 responses between the NCT and NET groups.
The most important role of neoadjuvant systemic therapy in hormone-responsive HER2-negative breast cancer is to increase the likelihood of breast-conserving surgery. 23 In our study, the BCS rate did not differ between the two groups. This finding is consistent with previously reported data from other prospective studies that compared NET with NCT.22,24
Most NET studies on breast cancer have focused on postmenopausal women with hormone-responsive, HER2-negative breast cancer.25-27 The ASCO guidelines recommend that neoadjuvant endocrine therapy with an aromatase inhibitor in postmenopausal women has similar activity to chemotherapy and can be considered for larger tumors for which tumor downstaging is desired. 17 Few data are available on NET in premenopausal women. The STAGE study demonstrated that 6 months of ovarian suppression plus aromatase inhibitors in NET was more effective in reducing tumor size than tamoxifen for premenopausal women. 28 A randomized phase III study (KBCSG-012) compared 24 weeks of neoadjuvant chemotherapy with neoadjuvant endocrine therapy using tamoxifen and goserelin. In contrast, the response rate was significantly higher in patients who received chemotherapy using both caliper measurements (83.9% vs 71.3%, P = .046) and MRI (83.7% vs 52.9%, P < .001). 22 Several differences exist between KBCSG-012 and our study, which may explain their discordant outcomes. First, the measurement method was caliper and MRI in the KBCSG-012 trial, but ultrasound in this study; second, the study populations were lymph node-positive and negative, respectively; third, the procedure durations were different. Our finding indicates that NET can be recommended in clinical practice in HR-positive/HER2-negative breast cancer and for patients with large tumors where BCS is not feasible.
This study had some limitations. First, the small sample size, which did not satisfy the predefined number, was included. Although the post-hoc power was 0.087, uncertainty and bias existed because of the small size. This study was underpowered to conclude the non-inferiority of NET to NCT. Second, two patients randomized to chemotherapy did not receive chemotherapy but received NET, and this crossover may have narrowed the difference between the groups. Third, multigene assays were not evaluated.
Conclusion
This trial has shown a good clinical response rate of NET in premenopausal patients with hormone-responsive, HER2-negative, lymph node-negative breast cancer. Because of early closure, this study is underpowered for drawing conclusions about the non-inferiority of NET to NCT. Meanwhile, the breast conservation rates were not statistically different. Neoadjuvant endocrine therapy with goserelin acetate plus an aromatase inhibitor in premenopausal women with hormone-responsive, HER2-negative, lymph node-negative breast cancer may be considered for larger tumors for which tumor downstaging is needed. However, we need more robust data before making definitive clinical recommendations.
Footnotes
Acknowledgements
The authors acknowledge Tao Ouyang for his assistance with the study design. We appreciate Yingjian He, who worked on statistics.
Ethical Statement
Ethical Approval
The research protocol was approved by the Ethics Committee of Beijing Cancer Hospital (2015YJZ06). All participant recruitment and data analysis in this study were carried out in accordance with Helsinki Declaration guidelines.
Informed Consent
Informed consent has been obtained from all participants.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: AstraZeneca participated provided funding for this study. The funder of the study had no role in the study design, data collection, data analysis, data interpretation, or writing of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are not publicly available due to their containing information that could compromise the privacy of research participants, but are available from the corresponding author upon reasonable request.