
Abstract
Background:
Metaplastic breast cancer (MetBC) represents a therapeutic challenge. We evaluated the impact of clinicopathological characteristics and treatment modalities on outcomes among MetBC patients treated at our center.
Methods:
Women with stage I-III MetBC were reviewed from our database from 2005-2018. Kaplan-Meier method was used to calculate locoregional-failure-free survival (LRFFS), overall-survival (OS) and distant-metastases-free survival (DMFS). We assessed associations with survival outcomes by log-rank tests. Multivariate Cox proportional-hazards models were used to identify independent predictors of LRFFS, OS and DMFS.
Results:
81 patients were eligible for the study. Median age at diagnosis was 48 years. 90.1% had G-III tumors, 64.2% were pathologically node negative and lympho-vascular invasion (LVI) was absent in 72.8%. 67.8% were triple negative, and 7.4% were HER2-neu positive. Most (66.7%) patients underwent mastectomy. Free margins were achieved in the entire cohort, however, 17.3% had close margin (<2 mm). Almost all patients received chemotherapy. 75.3% received radiotherapy, 23.5% received hormonal therapy and 6.2% received Trastuzumab. With a median follow-up of 54 months, 18.5% developed loco-regional recurrence and 34.6% relapsed distally. Five-year OS was 66.0%. On multivariate analysis: adjuvant radiotherapy correlated with better OS (P < .0001), and tumor size >5 cm, nodal involvement and LVI correlated with worse OS, (P = .019, P = .021, P = .028, respectively). There were no survival differences with respect to age, triple negativity, and morphologic subtype.
Conclusion:
We report the largest single institutional series on MetBC in the Middle East region. MetBC confers worse survival outcomes, and more aggressive local and systemic treatment strategies should be investigated.
Keywords
Introduction
Metaplastic breast carcinoma (MetBC) is a rare heterogeneous histologic subtype of breast cancer accounting for less than 1% of all breast cancers. 1 Therefore, data on this specific subtype is limited and retrospective. This rare entity encompasses various combinations of non-glandular epithelial (e.g., squamous) or mesenchymal components (e.g., osseous and chondroid). 2 These elements of MetBC can either present purely on pathology specimens or be admixed with adenocarcinoma. 2,3 It was first introduced by the World Health Organization (WHO) as a distinct pathologic category in 2000, and the 2012 WHO report identified 7 morphologic subtypes: low-grade adenosquamous, fibromatosis-like, mixed metaplastic carcinoma, spindle cell carcinoma, squamous cell carcinoma (SCC), metaplastic carcinoma with mesenchymal differentiation, and myoepithelial carcinoma. 4
Most MetBC are characterized as triple-negative with a higher propensity for both local relapse and distant metastases. 5,6 It poorly responds to standard treatment strategies and is particularly resistant to the conventional systemic regimens. 6,7 Furthermore, it tends to disseminate via the hematogenous route rather than the lymphatic route. 5,6 The relationship between the poor outcome of the disease and its triple negativity is still vague. However, the National Cancer Data Base (NCDB) reviewed MetBC patients’ outcomes and compared it with non-MetBC patients. They demonstrated that regardless of receptor status, MetBC patients had a worse overall survival (OS) (5-year OS for triple-negative breast cancer subset was 71% for MetBC and 78% for non-MetBC). 5
The optimal treatment paradigm for MetBC is insufficient, and the practice patterns are similar to those of invasive ductal carcinoma (IDC). 5,7 The previously mentioned NCDB has indicated that patients more frequently underwent mastectomy than breast-conserving surgery (BCS). The majority of patients received chemotherapy due to the higher tendency to present at advanced stages. 5 It also identified chemotherapy and adjuvant radiation as predictors of improved OS in MetBC. 5 In accordance with these results, adjuvant radiotherapy was associated with improved outcomes in other retrospective analyses. 7,8
Given the rarity of this type of breast cancer, clinical trials were difficult to conduct. To better understand the disease, a retrospective review of MetBC at a tertiary cancer center was conducted. The study aimed to review the clinicopathological characteristics and treatment modalities involved in MetBC and evaluate their impact on disease outcomes.
Methods
Women, ≥ 18 years old, with stage I-III metaplastic breast cancer, treated with curative intent at our center, were eligible to participate. The Institutional Review Board approved the study. We searched the breast cancers’ pathology database, using the keywords “metaplastic,” “squamous,” “spindle,” “fibromatosis,” “chondroid,” “osseous,” and “breast,” at King Hussein Cancer Center (KHCC) from 1st Jan 2005 to 31st Nov 2018. The following data were recorded from patients’ medical charts: age at diagnosis, pathologic tumor size, pathologic nodal status, presence of ductal carcinoma in situ (DCIS) component, margin status, hormonal and HER2-neu receptor status, and local and systemic treatment approaches. The Ki-67 proliferative index was not reported as it was not part of our routine testing in breast cancers. In patients who received neoadjuvant chemotherapy (NAC), clinical response was assessed using both clinical examination and radiologic (using RECIST criteria) assessment. Pathologic complete response (pCR) was defined as a lack of invasive components in both the primary and nodal disease.
Statistical Analysis
Loco-regional failure-free survival (LRFFS) was defined as the interval from diagnosis to the development of local or regional recurrence or last follow-up. Distant metastasis-free survival (DMFS) was defined as the interval from diagnosis to the development of distant metastases or last follow-up. Overall survival was defined as the interval from diagnosis to death from any cause or last follow-up.
Kaplan-Meier survival curves were analyzed with respect to the following variables: age at diagnosis (≥ 50 vs. < 50), pathologic tumor size (≤ 5 cm vs. > 5 cm), pathologic nodal status (positive vs. negative), margin status (≥ 2 mm vs. < 2 mm), lymphovascular invasion (LVI) (present vs. absent), hormonal receptor (HR) status, HER2-neu status, triple-negative subtype, type of breast surgery (mastectomy vs. breast-conserving), adjuvant radiotherapy (yes vs. no), and morphologic subtype.
Log-rank tests were conducted for univariate analysis to study the associations of the above-mentioned variables with LRFFS, OS, and DMFS. Only variables with statistically significant associations on the univariate analysis, were used in Cox proportional-hazards models for multivariate analysis. We reported hazard ratios (HRs) and 95% confidence intervals (CIs) with two-tailed P-values. P-values less than .05 were considered significant. All analyses were performed using SAS software version 9.4 (SAS Institute Inc., Cary, NC).
Results
A total of 124 cases were identified from the breast cancer database of 9106 cases (1.3%). Forty-three patients were excluded. Among these, 28 cases were submitted for pathology consultation only and were not treated at our center. Two patients had concomitant primary tumors (renal cell carcinoma and pelvic leiomyosarcoma), one was diagnosed with recurrent MetBC, and 12 patients presented with de novo metastatic disease.
A total of 81 patients were eligible for the study. Among them, 6 patients were lost to follow-up. The whole cohort (81 patients) was included in the descriptive analysis. However, those lost to follow-up were excluded in the univariate and multivariate analyses.
Patients and Tumor Characteristics and Treatment
The patients’ (no = 81) demographics and tumor characteristics are available in Table 1. The median age at diagnosis was 48 years old (range, 29-78 years). Seventy-one patients (90.1%) had G-III. 64.2% of patients were node-negative (n = 52), and 67.9% (n = 55) had triple-negative disease. 24.7% (n = 20) were HR-positive/HER2-neu negative, and 7.4% (n = 6) were HER2-neu positive. The median pathologic tumor size was 4 cm (range 0-15).
Patient Demographics and Tumor Characteristics.

Abbreviations: ADC, adenocarcinoma; DCIS, ductal carcinoma in-situ; HR, hormone receptor (either ER or PR or both); LIQ, lower inner quadrant; LOQ, lower outer quadrant; LVI, lymphovascular invasion; NOS, not otherwise specified; UIQ, upper inner quadrant; UOQ, upper outer quadrant.
The majority of patients (66.7%, n = 54) underwent mastectomy while the rest underwent BCS. Free margins (defined as no ink on tumor) were achieved in the entire cohort. However, 17.3% had close margins (<2 mm). Fifty-two patients (64.2%) underwent axillary dissection, and 28 patients (34.6%) underwent sentinel lymph node biopsy. One patient did not undergo axillary surgery. Fifty-two patients (64.2%) had tumor sizes measuring ≤5 cm. Fifty-nine patients (72.8%) had no LVI, and 49 patients (60.5%) had no DCIS component.
All patients except 5 received chemotherapy. Neoadjuvant chemotherapy was administered to 33 patients while the remaining 43 received adjuvant chemotherapy. NAC was administered according to the NSABP-B27 protocol (anthracycline- and taxane-based; 4 cycles each, every 21 days).
The predominant adjuvant chemotherapy regimen consisted of 5-Fluorouracil, epirubicin, and cyclophosphamide (FEC), followed by docetaxel (3 cycles each, every 21 days). Other regimens included adriamycin/cyclophosphamide (AC) with taxane; AC alone; and 5-Fluorouracil, adriamycin, and cyclophosphamide (FAC). Sixty-one patients (75.3%) received adjuvant radiotherapy. 82.6% of the patients with positive hormonal receptor status (n = 19/23) received hormonal therapy, and 83.3% of patients with HER-2neu positive receptors (n = 5/6) received trastuzumab (in 2 patients, it was part of neoadjuvant therapy).
Patients Diagnosed With Metastatic Disease at Presentation
Twelve patients were diagnosed with denovo metastatic MetBC. All patients had clinical G-III disease. Eight patients (66.7%) were triple-negative, and 4 patients (33%) were HER2-neu positive. In total, 66.7% had tumor size >5 cm, and 75% had clinical nodal involvement. Visceral metastases were the most common (66.7%), followed by bone (58.3%) and the brain (33.3%). Eight of the 12 patients died within 2 years of diagnosis. Only 1 patient survived after 3 years.
Disease Response to Neoadjuvant Chemotherapy
Most patients had either stable or progressive disease toward the end of NAC (Table 2). Upon surgical resection and pathological assessment, 19 patients (57.6%) had minimal to no response (defined as > 90% tumor viability). Twelve patients (36.4%) exhibited partial treatment effects, and 2 patients (6.0%) achieved pCR.
Patient Outcomes.

Abbreviations: CR, complete response; DP, disease progression; NAC, neoadjuvant therapy; PR, partial response; SD, stable disease.
Survival and Disease Control Analysis
The median follow-up period was 53.8 months (range 16-166 months). Fifteen patients (18.5%) had locoregional recurrence (LRR), and 28 patients (34.6%) developed distant relapse (Table 2). Five-year OS, LRFFS, and DMFS were 66.0%, 77.7%, and 64.8%, respectively. Kaplan-Meier estimates of survival curves are illustrated in Figure 1.

Kaplan-Meier estimates of survival outcomes (A) 5-year overall survival = 66.0%, (B) 5-year loco-regional failure-free survival = 77.7%, (C) 5-year distant metastases-free survival = 64.8%.
Loco-Regional Failure-Free Survival
On univariate analysis, close margin (<2 mm) and tumor size > 5 cm were associated with a higher risk of locoregional recurrence (P = .019 and P = .01, respectively) (Table 3). However, on multivariate analysis, only tumor size > 5 cm correlated with worse LRFFS (HR = 3.168) (Table 4).
Univariate Analysis.
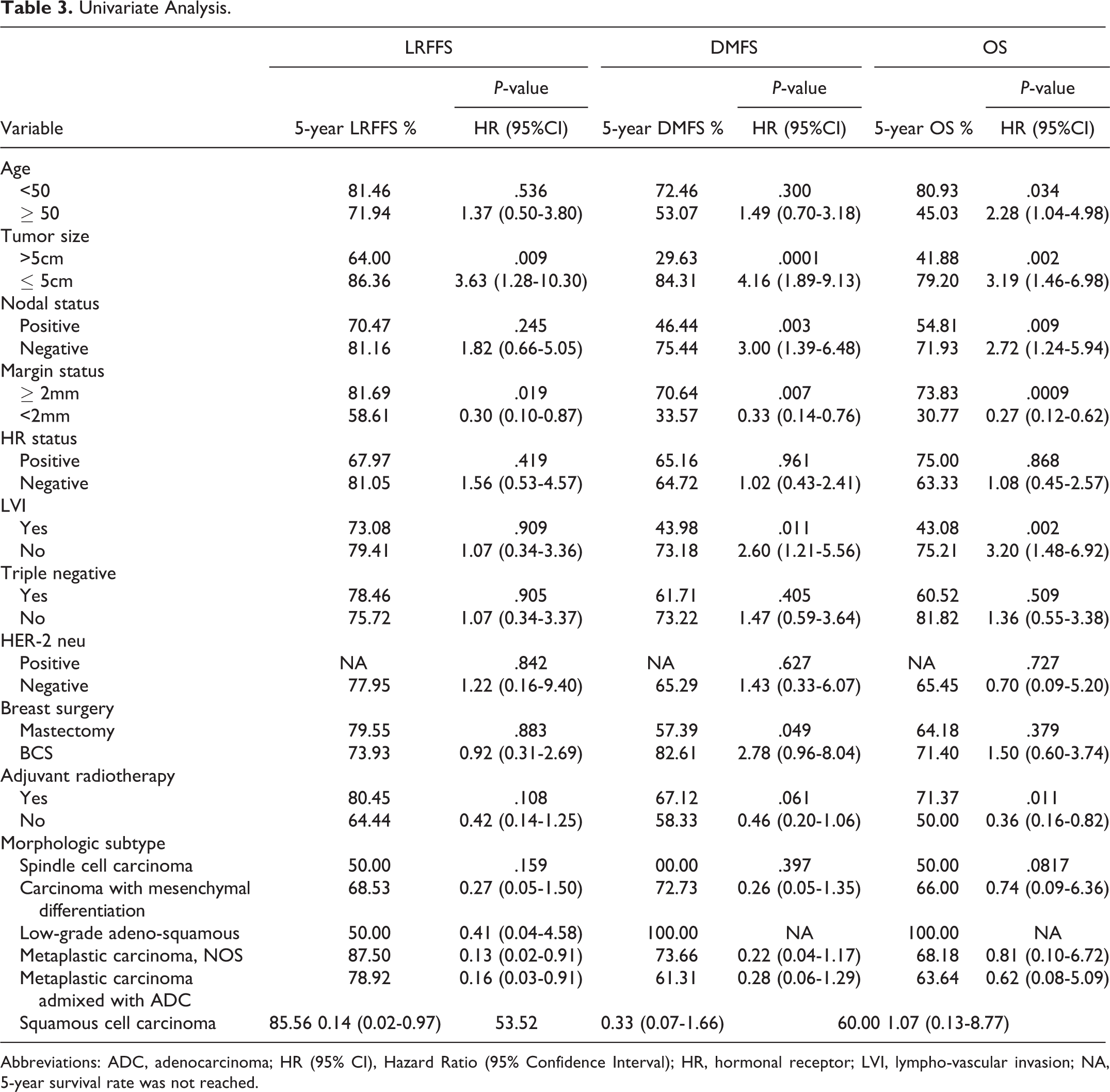
Abbreviations: ADC, adenocarcinoma; HR (95% CI), Hazard Ratio (95% Confidence Interval); HR, hormonal receptor; LVI, lympho-vascular invasion; NA, 5-year survival rate was not reached.
Multivariate Analysis.

Abbreviations: BCS, Breast-conserving surgery; CI, Confidence Interval; HR, Hazard Ratio; LVI, lympho-vascular invasion.
Distant Metastases-Free Survival
The following variables were correlated with a higher probability of distant metastases on univariate analysis: close margin (P = .007), tumor size > 5 cm (P = .0001), positive nodal status (P = .003), LVI (P = .01), and mastectomy (P = .049) (Table 3). On Cox regression, only tumor size (> 5 cm) remained statistically significant (P = .005) (Table 4).
Among the 28 patients who developed distant metastases, the lung was the most common site (75%). The second most common sites of metastases were the bone and brain (39% for each). Ten patients (36%) developed liver metastases. One patient developed soft tissue, brachial plexus, and adrenal metastases, in addition to liver and pulmonary metastases.
Overall Survival (OS)
Adjuvant radiotherapy, tumor size ≤ 5 cm, node-negative disease, age < 50 years, resection margins ≥ 2 mm, and LVI absence were associated with a significantly better OS on univariate analysis (Table 3). Only adjuvant radiotherapy, tumor size ≤ 5 cm, node-negative disease, and LVI absence remained statistically significant on multivariate analysis as independent predictors of improved OS (Table 4).
Discussion
One hundred twenty-four patients with MetBC were identified from our database from the past 13 years. Almost half of the patients were diagnosed in the last 4 years, reflecting the increased awareness of the pathologic diagnosis of this rare breast cancer subtype. To our knowledge, this cohort is the largest in the Middle East region. Due to their complex morphologic subtypes, metaplastic carcinomas pose a diagnostic dilemma. The differential diagnoses may overlap with those of breast sarcomas and phyllodes tumors. As an institutional policy, pathology specimens are reassessed in a peer-review meeting to agree on the diagnosis. Therefore, accurate immunohistochemistry stains are warranted because these disease entities differ in prognosis and treatment approach. MetBC overexpresses p63 in 90% of cases and is typically positive for cytokeratin 5/6 (CK 5/6). Additionally, it overexpresses epidermal growth factor receptor (EGFR). 4 There is insufficient data on the impact of the morphologic subtype on the prognosis of MetBC.
Women were diagnosed at a younger age (median = 48 years) compared to the metaplastic cohorts reported in the literature. 3,5,9 This was in line with the results of a recently published study from our institution, indicating that breast cancer was diagnosed at a younger age in our patient population (median = 51 years). 10 This analysis also evaluated the outcomes of 4561 breast cancer patients treated between 2006 and 2017 at our institution. The 5-year OS rates for stages I, II, III, and IV were 96.0%, 91.3%, 75.5%, and 31.5%, respectively. This confirmed that MetBC had a poorer OS compared to other subtypes. We reported a 5-year OS of 66.0% and 0% among stages I-III and IV, respectively.
The clinicopathologic characteristics and practice patterns of MetBC in our cohort were consistent with those reported in the literature. They tended to be high-grade, node-negative, and triple-negative, without LVI. Moreover, the DCIS component was present in only 40% of our MetBC cohort. On the other hand, 80% of breast invasive ductal carcinomas are associated with DCIS. 4 Mastectomy was the most common surgical approach, and almost all patients received chemotherapy.
MetBC is often negative for hormonal receptors and lacks HER2-neu gene amplification. The pCR rates in triple-negative IDC exceed 40% after NAC. 11 Treating MetBC is challenging due to its poor responsiveness to NAC. 12 Studies evaluating its response to NAC are limited. A recently published series involving MetBC patients (n = 18), who received NAC, demonstrated disease progression (DP) in 28% and pCR rate of 11%. 13 Han et al reported that in 29 MetBC patients (30%) who received NAC, only 5 patients (17%) achieved pCR. 3 We reported the largest single institutional series evaluating the outcomes of MetBC patients receiving NAC. Thirty-three of 81 patients (40.7%) received NAC. Among them, 22 (66.7%) were operable upon presentation. Fourteen patients (42.4%) had DP despite having a triple-negative disease in two-thirds (9 patients). Moreover, almost half (6/14) of patients who developed DP had pure SCC. Eight of these 14 patients had resectable disease upon presentation. NAC was administered either to allow BCS or due to its biologic subtype (triple-negative or HER2-neu positive). Only 2 out of 33 patients (6.0%) achieved pCR. One had metaplastic carcinoma with mesenchymal differentiation, and the other had metaplastic carcinoma admixed with adenocarcinoma. Among the 14 patients who progressed with NAC, eight died of the disease, one developed visceral metastasis, and 5 remained disease-free during the follow-up period. These results emphasized that the aggressive nature of MetBC was related to its complex pathologic subtypes, rather than triple negativity. Until new chemotherapeutic regimens or novel targeted agents are available, our study recommends immediate surgery for non-metastatic operable MetBC (especially with pure SCC histology), even in those exhibiting triple-negative disease or HER2-neu positivity.
Compared to the 20% of other breast cancer types, MetBC rarely overexpresses the HER2-neu gene. In a Surveillance, Epidemiology, and End Results (SEER) analysis, 5.2% (79/1516) of MetBC were HER2-neu positive. 14 This report also showed that HER2-neu positive MetBC was associated with better OS. In our study, 7.4% (6/81) had HER2-neu overexpression. However, it was not associated with a survival benefit, possibly due to the small sample size.
In our cohort, the 5-year OS was 66%. Han et al reported a similar OS rate. However, the median follow-up in our study was longer (54 months versus 39 months). 3 This contradicted the findings of a retrospective study of 42 patients from Pakistan, which obtained a higher OS (76%). However, the characteristics of this cohort differed from ours. Almost half were HR-positive and had nodal involvement. 15
Consistent with prior reports, our results indicated that tumor size ≤ 5 cm and absent nodal involvement were significant predictors of improved OS. 3,16 In addition, adjuvant radiotherapy was strongly correlated with better OS, but most patients in our cohort underwent a mastectomy. Sixty-one patients (75%) received adjuvant radiotherapy, while 38 patients received it following mastectomy. The rest received it as part of breast-conserving therapy. Notably, adjuvant radiotherapy did not confer significant LRFFS. However, it tended to benefit DMFS. Our data are consistent with a Chinese study that revealed significant survival benefit from adjuvant radiotherapy in MetBC. 17 This supports more aggressive local treatment for MetBC, even in its early stages.
This study was the first to show that tumors with close margins (defined as < 2 mm) had a higher probability for LRR and distant metastases and worse OS. Although not statistically significant on multivariate analysis, a trend toward significance was observed in terms of LRR (P = .07). This may be clinically relevant and may be explained by the presence of a sarcomatous component. In addition, it raises the question of obtaining wider margins in this entity. Further prospective data are warranted to validate this finding.
As for patterns of distant relapse, lung metastases were the most common, occurring in 75% (21 patients) of patients. IDC most commonly metastasizes to the bone, while MetBC mainly metastasizes to the lungs. 16,18,19 Moreover, the rate of lung metastases in MetBC exceeds that of triple-negative IDC, as reported by many series (60% vs. 40%, respectively). 16,19,20 This may be attributed to the presence of a sarcomatous component in MetBC and the aggressive nature of its triple-negative subtype. Based on this, routine chest imaging may be considered when monitoring these patients to detect early recurrences. This may have implications in offering early salvage ablative treatments like Stereotactic Body Radiotherapy (SBRT) that showed favorable outcomes in oligometastases. 21
Conclusion
Although this study was limited by its retrospective nature, a small number of patients, and involving only a single institution, it described new findings that gave a better understanding of metaplastic breast cancer. These results can pave the way for further multi-institutional prospective studies for further validation.
Footnotes
Abbreviations
Authors’ Note
This research was approved by KHCC IRB (Approval number/ID: 18KHCC156). This is a retrospective study where no experimental procedures were conducted. The data were collected through retrospective chart review so the need for informed consent was waived.
Acknowledgment
The authors would like to thank Ms. Ayat Taqash from the Office of Scientific Affairs and Research for performing the statistical analysis of the data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.