
Abstract
Objective
A high number of Non-Small Cell Lung Cancer (NSCLC) patients with brain metastasis who have not had surgery often have a negative outlook. Radiotherapy remains a most common and effective method. Nomograms were developed to forecast the cancer-specific survival (CSS) and overall survival (OS) in NSCLC individuals with nonoperative brain metastases who underwent radiotherapy.
Methods
Information was gathered from the Surveillance, Epidemiology, and End Results (SEER) database about patients diagnosed with NSCLC who had brain metastases not suitable for surgery. Nomograms were created and tested using multivariate Cox regression models to forecast CSS and OS at intervals of 1, 2, and 3 years.
Results
The research involved 3413 individuals diagnosed with NSCLC brain metastases who had undergone radiotherapy but had not experienced surgery. These participants were randomly divided into two categories. The analysis revealed that gender, age, ethnicity, marital status, tumor location, tumor laterality, tumor grade, histology, T stage, N stage, chemotherapy, tumor size, lung metastasis, bone metastasis, and liver metastasis were significant independent predictors for OS and CSS. The C-index for the training set for predicting OS was .709 (95% CI, .697-.721), and for the validation set, it was .705 (95% CI, .686-.723), respectively. The C-index for predicting CSS was .710 (95% CI, .697-.722) in the training set and .703 (95% CI, .684-.722) in the validation set, respectively. The nomograms model, as suggested by the impressive C-index, exhibits outstanding differentiation ability. Moreover, the ROC and calibration curves reveal its commendable precision and distinguishing potential.
Conclusions
For the first time, highly accurate and reliable nomograms were developed to predict OS and CSS in NSCLC patients with non-surgical brain metastases, who have undergone radiotherapy treatment. The nomograms may assist in tailoring counseling strategies and choosing the most effective treatment method.
Keywords
Introduction
In China, non-small cell lung cancer (NSCLC) accounts for a substantial proportion of both incidence and mortality in the realm of malignant tumors. 1 At the time of initial diagnosis, a majority of patients with NSCLC discover that distant metastases have already occurred in areas such as the brain, liver, and bones. As a result, the chance for surgical intervention is typically forfeited for the majority of advanced-stage NSCLC patients. Around 25 to 40 percent of patients with NSCLC develop brain metastases at some point in the progression of their illness. 2 The traditional standard treatment for advanced-stage NSCLC is chemotherapy with a combination of platinum-based drugs. However, the 5-year survival rate for metastatic NSCLC is low, standing at only 7%. 3 In clinical practice, the primary approaches for treating brain metastases in NSCLC without surgery typically involve radiotherapy, chemotherapy, targeted therapy, and immunotherapy. Radiotherapy, being the most conventional and effective treatment method, continues to play a crucial role in the management of NSCLC. Over 70% of advanced-stage NSCLC patients require radiotherapy,4,5 with a high effective rate of up to 60%. Nevertheless, NSCLC may still experience recurrence or metastasis following radiotherapy due to the presence of radiotherapy resistance and various other factors.6,7 Hence, prompt monitoring and treatment of non-surgical brain metastases in NSCLC patients who have undergone radiotherapy is of utmost importance for physicians. There has been limited research on the prognostic indicators for the inoperable brain metastases in NSCLC patients who underwent radiotherapy. Hence, it is imperative to develop a succinct, pragmatic, and all-encompassing framework for forecasting the overall survival (OS) and cancer-specific survival (CSS) of these patients.
A nomogram integrates multiple continuous or categorical variables to predict an individual’s prognosis. The primary foundation of this is primarily built upon commonly used statistical techniques like Cox regression or logistic regression.8,9 In comparison to conventional staging methods, the nomogram proves beneficial for clinical decision-making, offering enhanced accuracy and intuitive prognostic evaluations. Nevertheless, the majority of research is constrained by insufficient sample sizes and only a handful of predictive variables are recognized.10-13 Furthermore, there have been limited investigations that have developed nomograms for forecasting the survival rates of individuals diagnosed with NSCLC and nonsurgical brain metastases who have undergone radiotherapy.
Hence, we chose prevalent clinical risk factors from the Surveillance, Epidemiology, and End Results (SEER) database, which encompasses clinical data for about 30% of cancer individuals in the US, in order to gain deeper insights into the predictive elements affecting OS and CSS of NSCLC individuals with radiotherapy and inoperable brain metastases. The objective of our research is to develop prognostic nomograms for the survival rates at 1-year, 2-year, and 3-year intervals for patients with NSCLC who have inoperable brain metastases and have undergone radiotherapy.
Methods and Participants
Source of Data and Extraction of Data
Between 2010 and 2019, information was gathered from the SEER database regarding patients diagnosed with NSCLC who had brain metastases that were not suitable for surgery. The SEER database, while not directly defining criteria for non-suitability for surgery, provided extensive data regarding diagnoses, treatments, and patient characteristics. Our study leveraged this comprehensive data to support our determinations, meticulously designing criteria to identify patients for whom surgical intervention was infeasible or non-beneficial. These criteria encompassed factors such as the extent of metastatic disease, the patient’s overall health status, and the presence of multiple metastases. As the SEER database holds de-identified and openly accessible patient information, there was no need for ethical approval or informed consent. Our research methodology adhered to the guidelines published by SEER.
We collected clinicopathological information for NSCLC patients, including sex, age, race, site, marital status, histological tumor grade, laterality, TNM stage, surgery, radiotherapy, chemotherapy, metastatic site, tumor size. 14 Patient follow-up results, including survival status, cause of death, and survival time, were also available from the SEER database. Additionally, the SEER database provided patient follow-up outcomes, which encompassed information on the patient’s survival status. The reporting of this study conforms to TRIPOD guidelines. 15
For the purpose of our study, patients were identified and included at the point where brain metastases were diagnosed, categorized as M1 according to the TNM system, signifying an advanced stage of the disease. This precise determination of the disease stage at the diagnosis of brain metastases is paramount. It not only facilitates a more accurate prognostic assessment but also significantly influences the selection of the most appropriate therapeutic strategy. By focusing our analysis on patients with confirmed M1 stage at the time of brain metastasis diagnosis, we aim to develop survival predictive nomograms that accurately reflect the prognosis for this specific patient cohort.
The criteria for inclusion consisted of (1) primary location in the lung and bronchus; (2) histology/behavior, specifically malignant NSCLC (including 8004, 8012, 8013, 8014, 8022, 8031, 8035, 8046, 8050, 8052, 8071, 8075, 8082, 8084, 8123, 8200, 8240, 8244, 8245, 8249, 8250e8255, 8260, 8290, 8310, 8323, 8333, 8430, 8480, 8481, 8490, 8507, 8550, 8560, 8562, 8570, 8571, 8574, 8576, 8980); (3) diagnosis made between 2010 and 2019; and (4) complete survival data available with a minimum of 1 day of survival. (5) suffering from non-surgical brain metastases;
Exclusion criteria: (1) the M staging is M0 or unknown; (2) the brain metastasis is No or unknown; (3) the Surgery is yes or unknown; (4) the Marital is unknown; (5) the T staging is T0\Tx; (6) the N staging is Nx; (7) the size is unknown; (8) the bone metastasis is unknown; (9) the liver metastasis is unknown; (10) the lung metastasis is unknown; (11) survival time less than 1 month or unknown. Figure 1 displays the flowchart outlining the criteria for patient inclusion and exclusion. The flowchart below shows how patients with inoperable brain metastases from NSCLC are included and excluded.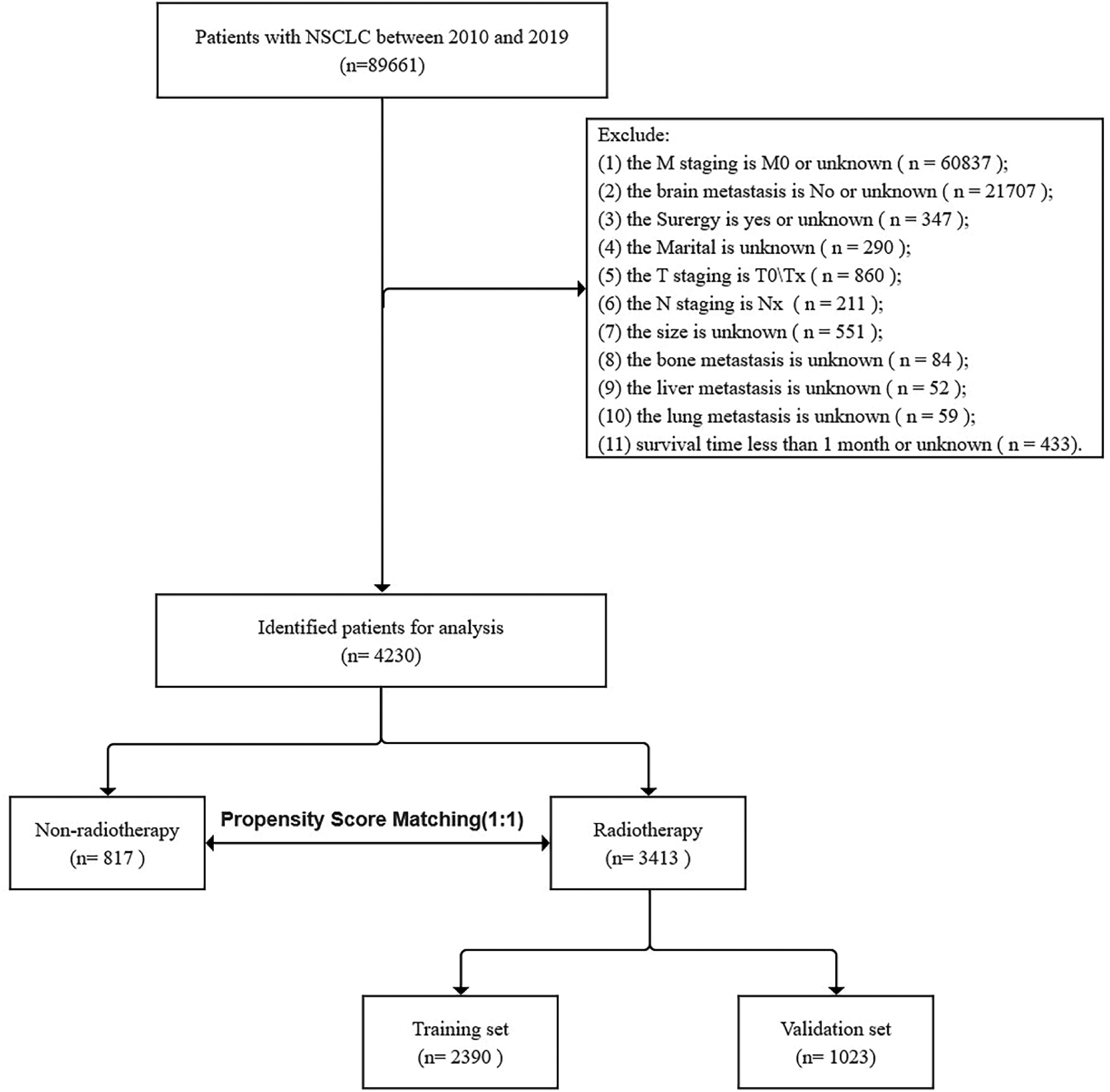
Creation of the Nomograms
Initially, we divide the patient data into a training set, which accounts for 70%, and a validation set, which accounts for the remaining 30%. Then, In the training set, univariate and multivariate Cox proportional regression models were employed to identify independent risk factors affecting patient prognosis. Based on the multivariate Cox regression model, we developed nomograms for predicting cancer-specific survival (CSS) and overall survival (OS) at 1-, 2-, and 3-year intervals.
Verification of the Nomograms
To evaluate the accuracy of the nomogram, a standard curve of 1000 samples was employed using bootstrap methodology. In addition, we evaluated the precision and specificity of the model by measuring the c-index and the area under the receiver operating characteristic curve (AUC). 16 Then, we employed decision analysis curves (DCA) and projected time spans of 1 year to assess the practicality of our nomograms on CSS and OS in comparison to the TNM staging system. Furthermore, we calculated patient risks using time-dependent receiver operating characteristic (ROC) curves, categorizing them into high-risk or low-risk groups based on a cutoff value. By adjusting variable critical values to determine sensitivity and specificity, we plotted these against 1-specificity to create the ROC curve, examining the nonlinear relationship between risk scores and CSS/OS. The optimal cutoff was determined as the risk score nearest to a hazard ratio (HR) of 1. Survival differences between risk groups were analyzed using Log-rank tests and Kaplan-Meier (K-M) curves.
Analysis of Statistics
The comparison between groups was conducted using either the chi-square test or the non-parametric U-test. Frequency was used to express other categorical variables, and a chi-square test was employed for comparison. R software version 4.1.0 was utilized for statistical analyses.
To ensure comparability between target and control groups, Propensity Score Matching (PSM) was applied using the “MatchIt” package for 1:1 nearest-neighbor matching with a .05 caliper. The “rms” package facilitated nomogram construction, and Cox regression was performed with “survival.” ROC curves were generated via “survivalROC,” and Kaplan–Meier curves were visualized using “ggplot2.” Additionally, the “ggDCA” package enabled DCA, enhancing the evaluation of prognostic model benefits.
Results
Clinical Characteristics and Survival Differences Between Non-Radiation and Radiation Non-Surgical Brain Metastasis NSCLC Patients
Demographics and Clinicopathological Characteristics of the Training and Validation Cohort.


The Kaplan-Meier curves of non-radiotherapy and radiotherapy patients. Before (A) and after (C) PSM analysis, the OS rate of the non-radiotherapy group was significantly lower than that of the radiotherapy group based on the K-M curve. As shown by the K-M curve, the CSS rate of the non-radiotherapy group was significantly lower than that of the radiotherapy group both before and after PSM analysis (B, D)
Next, a PSM analysis was conducted comparing the groups that received radiotherapy and those that did not receive radiation treatment. Following the implementation of PSM, a statistically significant disparity was observed in the variables, including chemotherapy, between the radiation therapy cohort (n = 810) and the non-radiation therapy cohort (n = 810). After performing PSM, we proceeded to compare the disparities in OS and CSS among the two cohorts. The K-M curve indicated a notable decrease in both OS and CSS within the non-radiotherapy group (Figure 2C and D).
Radiotherapy was Administered to NSCLC Patients With Non-Surgical Brain Metastasis, Exhibiting Clinical Characteristics
A total of 3413 individuals diagnosed with non-surgical brain metastases in NSCLC were divided into two groups: a training cohort consisting of 2390 patients and a validation cohort consisting of 1023 patients. No statistically significant differences were observed between the two groups regarding gender, age, race, location, laterality, grading, histology, chemotherapy, and other analysis variables (Table 1).
Analysis of Cox Regression Using Both Univariate and Multivariate Methods
Univariate and Multivariate Analyses of OS in Training Cohort.

Univariate and Multivariate Analyses of CSS in Training Cohort.

The Creation and Verification of Column Line Graphs for OS and CSS Over a Period of 1, 2, and 3 years
In order to forecast the OS and CSS after 1, 2, and 3 years in NSCLC individuals with radiotherapy and inoperable brain metastases, we developed histograms using multivariate Cox regression models (Figure 3). According to Figure 3, the histograms indicated that OS-specific histograms were most influenced by chemotherapy, with histology following closely behind. Chemotherapy was also a major predictor of CSS in the CSS histogram, followed by histology. NSCLC patients with nonsurgical brain metastases treated with radiotherapy can be predicted according to the following nomograms: 1-, 2-, 3-year CSS and OS. (A) The nomogram for predicting OS. (B) Nomogram for predicting CSS.
The c-index for the training sets of the OS and CSS histograms were .709 (95% CI, .697-.721) and .710 (95% CI, .697-.722), respectively. As for the validation sets of the OS and CSS bar chart, the c-indices were .705 (95% CI, .686-.723) and .703 (95% CI, .684-.722), respectively. These results indicate that the prognostic model exhibits superior discriminatory capability.
The calibration curves in both the training and validation sets demonstrate a strong correspondence between the predicted values of the OS and CSS histograms and the actual observed values (Figure 4), suggesting a high level of accuracy in the histogram fitting. Figure 5 illustrates the outcomes of the AUC values for years 1, 2, and 3 in both the validation and training sets of OS and CSS. The results indicate a notable differentiation between the histograms, suggesting a statistically significant contrast. The calibration curve of the nomograms for predicting 1-,2-,3-year OS and CSS in NSCLC patients with nonsurgical brain metastases treated with radiotherapy. (A, B) Calibration curve of the nomograms for predicting 1-,2-,3-year OS in the training set and validation set. (C, D) In the training and validation set, the calibration curve of the nomograms was calculated for predicting 1-,2-,3-year CSS. AUC for predicting 1-, 2-, and 3-year OS and CSS NSCLC patients with nonsurgical brain metastases treated with radiotherapy. (A, B) The AUC at 1-, 2-, and 3-year for OS in the training and validation set. (C, D) The AUC at 1-, 2- and 3-year for CSS in the training and validation set.

Clinical Application of the Column Line Charts
DCA demonstrated the clinical significance of column line charts in the OS and CSS training and validation sets (Figure 6). According to DCA, the column line charts specific to the operating system and CSS demonstrate superior clinical usefulness compared to the conventional TNM staging. Using ROC curves, we derived the risk values and optimal cutoff values for individual patients by analyzing the column line charts. To predict OS, patients were divided into high-risk (with a total score of 219.13 or higher) and low-risk (with a total score below 219.13) groups. Similarly, for predicting CSS, patients were categorized into high-risk (with a total score of 213.99 or higher) and low-risk (with a total score below 184.88) groups. Figure 7 displayed the K-M plot indicating that patients in the high-risk category experienced notably reduced OS and CSS compared to those in the low-risk category, in both the training and validation datasets. DCA of the nomograms for predicting OS and CSS in patients with nonsurgical brain metastases treated with radiotherapy. (A, B) In both the training and validation sets, the nomogram for OS at 1-,2-,3-year showed the best application potential, followed by D′ Amico risk stratification and TNM staging. (C, D) In both the training and validation sets, CSS at 1-, 2-, 3-year showed the greatest application potential, followed by D′ Amico risk stratification and TNM staging. A comparison of Kaplan-Meier curves for patients at low and high risk groups. In both the training (A) and validation sets (B), both the K-M curves showed that the OS rate for the high-risk patients was significantly lower than for the low-risk patients. In both the training (C) and validation sets (D), both the K-M curves showed that the CSS rate for the high-risk patients was significantly lower than for the low-risk patients.

Discussion
In this study, various clinical pathological factors were analyzed to determine the factors linked to the survival of NSCLC individuals with radiotherapy and inoperable brain metastases. The nomograms we created by combining the mentioned factors were utilized for predicting OS and CSS of study population, for durations of 1 year, 2 years, and 3 years. These nomograms exhibited excellent discriminatory capability, as evidenced by the C-index, calibration curve, and AUC. Moreover, the analysis of DCA demonstrated that the developed nomograms provided greater clinical advantages compared to TNM staging. The nomograms aids in monitoring the clinical prognosis and developing personalized treatment strategies for NSCLC individuals with radiotherapy and inoperable brain metastases.
The effectiveness of radiation therapy in stage IV NSCLC patients is still a subject of debate, with ongoing concerns regarding the potential for radiation toxicity and other negative occurrences.17-19 Research has indicated that brain metastasis patients who do not receive treatment have a very bleak outlook, with an average lifespan of 1-2 months. However, this can be extended to 4-6 months by undergoing whole-brain radiation therapy (WBRT), making WBRT the established approach for patients with multiple brain metastases.18,19 In recent times, there has been evidence suggesting that stereotactic radiosurgery (SRS) is superior to WBRT for individuals with fewer brain metastases due to the potential risks and negative impact on neurofunction associated with WBRT. According to a retrospective study conducted at multiple centers, it was found that patients with NSCLC who had fewer than 4 brain metastases and underwent stereotactic radiosurgery (SRS) as their first treatment had a greater chance of survival compared to those who received WBRT, even after adjusting for propensity scores. 20 Furthermore, a potential observational investigation demonstrated that individuals with 5-10 and 2-4 brain metastases experienced comparable survival rates when subjected to SRS as their primary therapy. 21 Several studies conducted in the past have indicated that SRS is equally secure and efficient when treating 10 or more lesions compared to a smaller number of lesions.22-24
After conducting PSM, we examined the disparities in OS and CSS between two cohorts. The analysis of the Kaplan-Meier curve indicated a significant decrease in both OS and CSS within the non-radiotherapy cohort compared to the radiotherapy cohort. Hence, it is imperative to examine prognostic indicators associated with the survival of patients with inoperable brain metastases from NSCLC who are undergoing radiotherapy. Additionally, it is crucial to develop a succinct, pragmatic, and all-encompassing framework for forecasting the OS and CSS of these individuals. In this extensive population research, we discovered that gender, age group, ethnicity, academic level, tissue type, N stage, tumor dimension, chemotherapy treatment, bone spread, and liver spread were all separate elements affecting OS and CSS. The majority of these factors align with the risk factors for brain metastases in NSCLC identified in prior research.25-27 Nevertheless, prior studies have not established numerous predictive factors for NSCLC individuals with radiotherapy and inoperable brain metastases.
The authors Peng and colleagues created a nomogram model that includes 12 separate predictive factors to forecast the occurrence of brain metastases in NSCLC patients. 13 According to Wang and colleagues, a survival model was created that consisted of 16 clinical factors to forecast OS in individuals diagnosed with metastatic NSCLC. 28 In addition, Zeng and colleagues created a nomogram to forecast os in surgically treated NSCLC patients who are undergoing chemotherapy. 29 While the development of the prognostic nomograms represents significant advancements in forecasting outcomes for NSCLC patients, these models notably lack inclusion of variables specifically related to radiation therapy, a key treatment modality for patients with brain metastases. Hence, the primary emphasis of this research is on individuals with inoperable brain metastases who have been diagnosed with NSCLC and are undergoing radiotherapy.
Our prognostic model, developed using the SEER database, is designed to identify key factors influencing the survival outcomes of NSCLC patients with brain metastases treated with radiotherapy. Unlike the Graded Prognostic Assessment (GPA), Lung-molGPA, and the modified Recursive Partitioning Analysis (mRPA) models,30-32 which incorporate specific molecular markers and detailed clinical characteristics, our model utilizes a broader set of variables available within the SEER database. This distinction allows our model to be applied across a wider range of clinical settings, particularly where detailed molecular data may not be readily accessible.
While the GPA, Lung-molGPA, and mRPA models offer valuable insights into the prognosis of NSCLC patients with brain metastases, they also present limitations, primarily the requirement for comprehensive molecular profiling. Our approach seeks to complement these models by providing a prognostic tool that remains informative and applicable even in the absence of extensive molecular data. It is important to acknowledge that the methodological differences between our model and the aforementioned models may influence their relative performance and applicability. Our model aims to strike a balance by offering prognostic insights based on a broader set of variables, thus maintaining relevance across various healthcare settings.
Based solely on clinical features, this is the first and largest effective nomogram. While our nomogram indeed provided accurate predictions for overall survival OS and CSS rates in nonsurgical brain metastasis patients with NSCLC who underwent radiotherapy, it is important to acknowledge that the study does have certain limitations. Our retrospective analysis inherently introduces selection bias and challenges in accurately assessing pathological findings, primarily due to reliance on biopsy specimens from metastatic NSCLC cases. A critical limitation is the absence of molecular and genetic information, pivotal for prognostication and the tailoring of treatments in the era of precision medicine. Our model’s focus on conventional treatment approaches, without distinct consideration for advanced treatments such as targeted therapy and immunotherapy, omits their significant impact on survival outcomes. Additionally, by pooling various radiotherapy techniques, including stereotactic radiosurgery (SRS) and whole-brain radiation therapy (WBRT), into a broader category of radiotherapy technologies, we may not fully capture the nuanced effects of these distinct treatments. This summary underscores the necessity for future research to integrate comprehensive clinical, molecular, and treatment-specific data to enhance prognostic models and therapeutic strategies for NSCLC patients with brain metastases.
Conclusion
We have created the nomograms for accurate prognosis of the OS and CSS in NSCLC patients with brain metastases who underwent radiotherapy. Furthermore, the validations demonstrated the precision and discriminatory nature of the nomograms. The nomograms may assist in tailoring counseling strategies and choosing the most effective treatment method.
Data availability
Publicly available datasets were analyzed in this study. This data can be found at: https://seer.cancer.gov/data-software/.
Footnotes
Author Contributions
PL and XG designed the study. PL, JL, and ZZ collected and analyzed the data. PL and JL drafted the initial manuscript. LM, AZ and XG reviewed and edited the article. PL, XG and WC revised and proofread the article. All authors approved the final manuscript. All authors contributed to the article and approved the submitted version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Shanghai Municipal Health Commission (202140256), Shanghai Science and Technology Innovation Action Plan (20Y11913600), Shanghai Natural Science Foundation (21ZR1453300), Shanghai Pulmonary Hospital Backbone Program (fkgg1808), Shanghai Talents Development Fund Project (2021071), Clinical Research fundation of Shanghai Pulmonary Hospital (SKPY20211006).