
Abstract
Background
This study aimed to develop a novel predictive nomogram to identify specific stage IB non-small cell lung cancer (NSCLC) populations who could benefit from adjuvant chemotherapy (ACT).
Method
Stage IB NSCLC patients were included in the Surveillance, Epidemiology, and End Results (SEER) database and divided into the ACT and non-ACT groups. Then the methods of Kaplan-Meier analysis, propensity score matching (PSM), Least absolute shrink and selection operator (LASSO) regression, and multivariate logistic regression analyses were implemented. Finally, the predictive nomogram was constructed and validated.
Results
9055 stage IB NSCLC patients were enrolled from the SEER database while 47 patients from Hangzhou TCM Hospital Affiliated to Zhejiang Chinese Medical University were identified as the external validation cohort. Of these patients, 1334 cases underwent ACT while the other 7721 patients didn’t receive ACT. After PSM, the patients in the ACT group presented longer median overall survival (100 vs 82 months, P < .001). Among the ACT group, 482 (49.6%) patients achieving more prolonged overall survival than 82 months were regarded as the beneficiary population. Then the LASSO regression and multivariate logistic regression analyses were implemented. Finally, 8 predictors were selected for model construction, including age, gender, marital status, laterality, pathology, tumor size, regional nodes examined, and tumor size. The predictive nomogram demonstrated good discrimination in the training cohort (AUC = .781), internal validation cohort (AUC = .772), and external validation cohort (AUC = .851). And calibration curves indicated ideal consistency between the predicted and observed probabilities. Decision curve analysis presented a clinically useful model.
Conclusion
The practical nomogram could guide treatment decision-making and select optimal ACT candidates among stage IB NSCLC patients.
Introduction
Lung cancer is the leading cause of cancer mortality among malignant tumors. 1 Non-small cell lung cancer (NSCLC) is the most frequent subtype, 2 with a 5-year relative survival rate to be 12-15%. 3 The curative-intent anatomic operation is the best therapeutic method for early-stage NSCLC, providing the greatest long-term survival opportunity. However, 18-32% of stage IB NSCLC patients died from tumor recurrence within 5 years following operation.4,5 Adjuvant chemotherapy (ACT), a comprehensive therapy, can decrease the onset of recurrence and distant metastases. It has been regarded as the standard therapy for stage II and III NSCLC patients after operation, with an approximately 5% improvement in 5-year survival.6-8
However, whether postoperative ACT is required among stage IB NSCLC patients remains controversial. The National Comprehensive Cancer Network guideline recommends postoperative ACT for high-risk patients with characteristics of poor differentiation grade, unspecified N stage, and visceral pleural invasion. 9 But according to the American Society of Clinical Oncology guidelines, there is no adequate evidence supporting ACT in stage IB NSCLC patients. 10
There is no consensus on the role of ACT in stage IB NSCLC patients. Numerous research demonstrated that ACT could prolong overall survival (OS) in these patients.11-13 Jang et al.’s study enrolled 328 stage IB patients, observing that ACT could significantly prolong the 5-year recurrence-free survival (RFS) and OS compared to the non-ACT patients. 11 Another study found that postoperative stage IB NSCLC patients could benefit from ACT regardless of tumor size. 12 Conversely, several studies indicated that survival did not differ significantly by ACT.6,14,15 Despite the controversial role of ACT, it’s clear that a specific group of these patients can obtain more prolonged survival after ACT. Identifying candidates who could gain potential benefits from ACT is an urgent issue that needs to be addressed.
The retrospective research aimed to use the Surveillance, Epidemiology, and End Results (SEER) database to construct an effective model to identify specific stage IB NSCLC populations who could benefit from ACT.
Materials and Methods
Data Source and Patient Selection
The records of NSCLC patients between 2010 and 2015 were extracted from the SEER database using SEER*Sat software (Version 8.3.5). And the external validation data was extracted from Hangzhou TCM Hospital Affiliated to Zhejiang Chinese Medical University from January 2012 to December 2016. The inclusion criteria were as follows: (1) age over 18 years; (2) NSCLC as the only histologically confirmed primary tumor; (3) patients underwent lobectomy, sublobar resection, or pneumonectomy; (4) pathological diagnosis as stage IB according to the eighth edition of the AJCC Staging Manual; (5) no lymph nodes or distant metastasis. The exclusion criteria were as follows: (1) patients who survived less than 1 month; (2) patients who received radiotherapy; (3) patients without complete clinicopathologic features, demographic data, and survival information. The workflow of the research is presented in Figure 1. The project involving human participants was reviewed and approved by the Ethics Committee of Hangzhou TCM Hospital Affiliated to Zhejiang Chinese Medical University. The workflow of the patient selection process.
Clinicopathological Variables
Demographic data (age, gender, race, marital status), features of tumors (size, laterality, grade, primary site, and pathological subtype), treatment information (chemotherapy, surgical type, regional nodes examined), and follow-up details (survival status and survival time) were retrieved from the SEER database. The stage IB patients were reclassified according to the eighth edition TNM (tumor node metastasis) classification based on the sixth edition recorded in the SEER database. The ACT patients who presented longer OS than the median OS in the non-ACT cohort were regarded as the benefit population.
Statistical Analysis
The chi-square test was used for categorical data. Then the subgroup analysis was performed using a univariate Cox proportional hazard model. Hazard ratios (HRs) and 95% confidential intervals (CIs) in each subgroup were recorded in the forest plots. To adjust for the potential imbalance between groups, a propensity score matching (PSM) method was applied. 16 Cases in both cohorts were one-to-one matched by the nearest-neighbor algorithm. Standardized difference (SD) was used to assess the alternation of variables before and after PSM. Then the ACT cohort was randomly separated into a training set (70%, n = 680) and a validation set (30%, n = 291) for further analysis.
Least absolute shrink and selection operator (LASSO) regression, a method used to identify independent risk factors, could remarkably prevent redundancy or overfitting of the multifactor models. 17 After selecting significant variables by LASSO regression, a multivariable logistic regression model was constructed on the training set. Then a predictive nomogram was developed to identify potential ACT-beneficial cases. In the model, a vertical line was drawn to each parameter’s “points” line, and the sum of every point corresponds to the benefit probability.
The discrimination of the predictive model was assessed by receiver operating characteristics (ROC) curves and the area under the curves (AUC). AUC with a higher value indicated that the prediction power was greater. The calibration curve was used to measure if the predicted and observed survival probabilities were consistent. To further evaluate the benefits and advantages of the nomogram, the decision curve analysis (DCA) was performed. It could estimate the practicability of the nomogram by plotting net benefit (NB) at a range of clinically reasonable risk thresholds. 18 The entire evaluation procedure was repeated 1000 times using bootstrapping.
R software (version 4.0.3) was employed for the statistical analyses and visualizations. It was determined that a P-value <.05 (2-sided) was statistically significant.
Results
Clinicopathological Characteristics
9055 patients were enrolled in the SEER database from 2004 to 2015. And 47 patients from Hangzhou TCM Hospital Affiliated to Zhejiang Chinese Medical University were identified as the external validation cohort. Of these patients, 1334 cases underwent ACT while the other 7721 patients didn’t receive ACT. There were significant dissimilarities between the 2 cohorts in the characteristics, including age, marital status, grade, pathology, and tumor size. The patients who underwent ACT tended to present a higher proportion of marital status (61.7% vs 57.4%), grade III (43.6% vs 37.0%), grade IV (3.4% vs 1.9%), and tumor size over 3 cm (84.0% vs 79.9%). The non-ACT group presented more percentage of squamous cell carcinoma (35.6% vs 27.7%) than the patients in the ACT group.
The Characteristics of Stage IB NSCLC Patients Before and After PSM.

Survival Analysis
In the Kaplan-Meier analysis, significant differences in OS were found. Before PSM, the patients who underwent ACT presented longer median OS than the non-ACT cohort (100 vs 72 months, P < .001) (Figure 2(A)). After PSM, a similar result was observed (100 vs 82 months, P < .001) (Figure 2(B)). Then the subgroup analysis of pathology was performed, indicating that the ACT group present better OS in adenocarcinoma (P < .001), but not in squamous carcinoma (P > .05) (Figure 2(C)-(D)). In the forest plots, HRs in most subgroups were less than 1 before and after PSM, indicating that stage IB patients could benefit from ACT in most subgroups (Figure 3). Then 358 ACT patients diagnosed between 2013 and 2015 (longest follow-up time as 71 months) were excluded from further study because we couldn’t specify if these patients occurred the event of interest. Overall survival curves in the ACT group and non-ACT group. (A) Before PSM. (B) After PSM. (C) Patients with adenocarcinoma. (D) Patients with squamous cell carcinoma. Forest plot of hazard ratios (HRs) for overall survival in the 2 groups. Diamonds represent effect size, calculated separately in different subgroups, and error bars indicate 95% CIs. (A) Before PSM. (B) After PSM.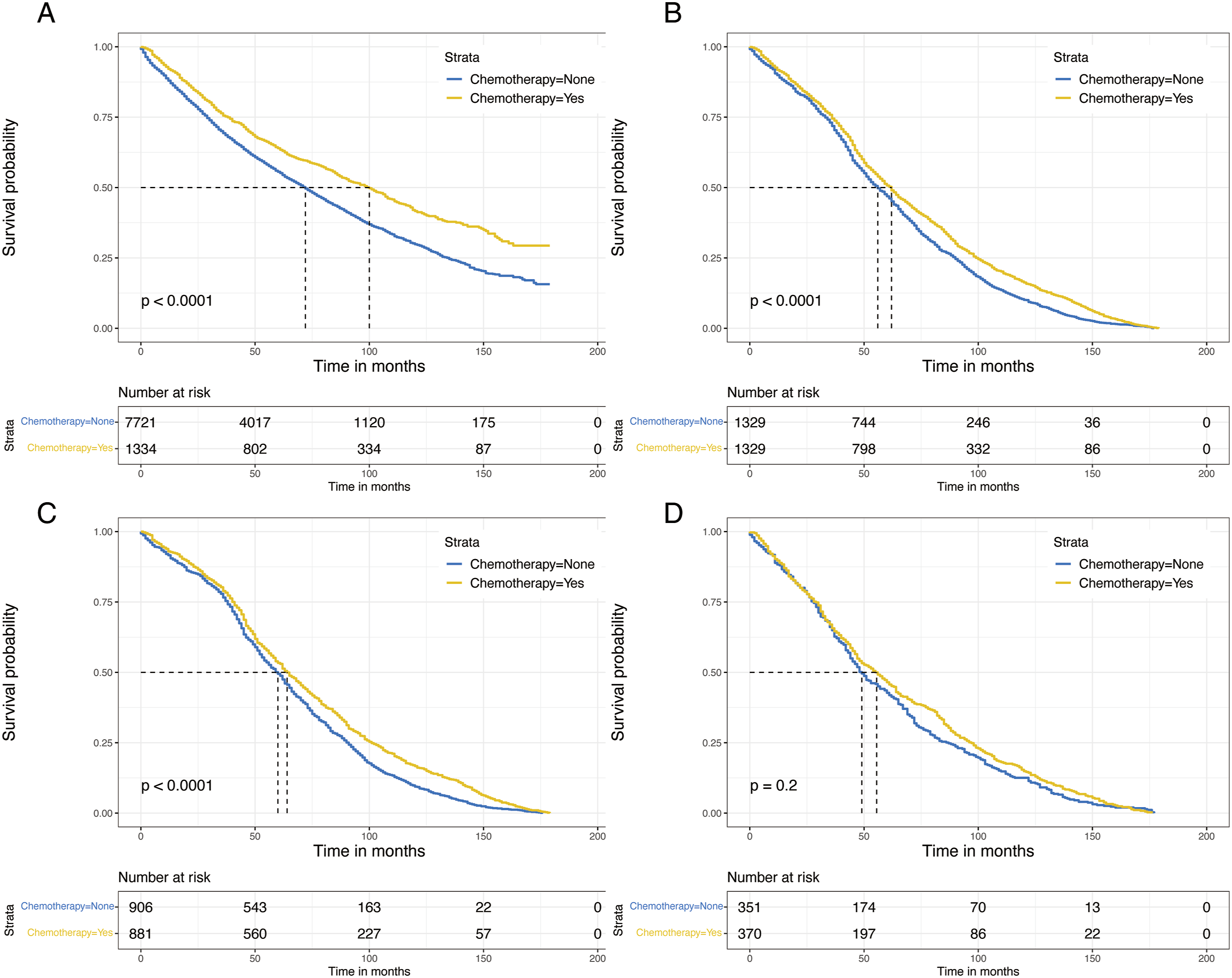

Independent Prognostic Factors Selection
The patients in the ACT cohort were used for further analysis and randomly divided into a training group (70%, n = 680) and an internal validation group (30%, n = 291). The essential characteristics of the 2 groups are shown in Table S1. A total of 11 variables were included in the LASSO logistic regression based on the training group to prevent overfitting. Finally, 8 predictors were selected for multivariate logistic regression and model construction, including age, gender, marital status, laterality, pathology, tumor size, regional nodes examined, and tumor size (Figure 4, Table 2). Feature selection using the LASSO logistic regression. (A) Profiles of LASSO coefficient for clinical and pathological features. (B) Selection of tuning parameter (lambda) in the LASSO regression using 5-fold cross-validation. Logistic Regression Analysis of the Significant Factors for ACT Benefit.

Constructing and Verifying the Nomogram
A predictive nomogram was constructed to identify potential ACT-beneficial cases based on the variables selected by LASSO analysis (Figure 5). The total points were calculated by adding the score in each row of variables, which was used to assess the likelihood of ACT-beneficial probability in stage IB NSCLC patients. The nomogram to identify candidates among stage IB NSCLC patients who could obtain survival benefits from ACT. The calculated points correspond to a benefit probability.
The AUC value assessed the discrimination ability of the model in the training cohort (AUC = .781), internal validation cohort (AUC = .772), and external validation group (AUC = .851), which presented good discriminatory power (Figure 6(A), (D), and (G)). The calibration plots showed ideal consistency between the predicted and observed probabilities (Figure 6(B), (E), and (H)). Then the DCA curves demonstrated the good clinical practical utility of the predictive model in the 3 sets (Figure 6(C), (F), and (I)). Thus, the nomogram exhibited powerful predictive performance and accurate predictive efficacy. ROC curves, calibration curves, and DCA curves of the nomogram in the training, internal validation, and external validation cohorts. (A-C) Training cohort. (D-F) Internal validation cohort. (G-I) External validation cohort.
Discussion
Some studies had investigated the survival of postoperative stage IB NSCLC patients and constructed prognostic stratification models.19,20 However, these prognostic models only presented the prognosis at a specific point in time. And the role of ACT wasn’t deeply expatiated. When clinicians made decisions, selecting appropriate patients for ACT was an important issue. This study discovered that stage IB NSCLC patients who underwent ACT presented a better prognosis than those who did not. A predictive nomogram was constructed to identify the patients who could benefit from postoperative ACT. The nomogram incorporating age, gender, pathology, regional nodes examined, surgery, and radiation presented potential clinical applicability. To the best of our knowledge, this was the first study to establish a novel nomogram to identify stage IB NSCLC patients who might benefit from ACT.
Previous research had revealed that stage IB NSCLC patients could obtain survival benefits from ACT.19,21-25 Jang et al and a meta-analysis observed that stage IB NSCLC patients who received ACT significantly prolonged the 5-year RFS and OS compared to the non-ACT patients after radical operation.11,26 Tu et al. also discovered that stage IB NSCLC patients who underwent ACT had a considerably longer OS than those who were not. 19 Furthermore, 2 studies based on the National Cancer Data Base found that patients with node-negative and diameter less than 4 cm tumors could also benefit from ACT.27,28 However, several studies proposed the opposite view. A meta-analysis suggested that patients with stage IB did not present a clear benefit from ACT. 15 A study by Moon Y et al involving 211 stage IB NSCLC patients, also showed that ACT did not improve OS. 29 However, only 20 patients received ACT in the study, so the conclusions should be cautiously taken. CALBG 9633 trial, the only randomized controlled study (RCT) primarily focused on individuals with stage IB NSCLC, failed to reveal an OS benefit with ACT. 14 The small sample size (only 344 participants) and low event occurrence rate might partly explain the disappointing results.
Despite these conflicting results, it was clear that a specific population of stage IB NSCLC could benefit from ACT. A recent study classified the entire cohort of stage IB NSCLC patients into low-risk, intermediate-risk, and high-risk groups according to the recurrence-free survival (RFS), revealing that the high-risk patients could most benefit from ACT. 30 In our study, among the total patients who underwent ACT, 571 patients obtained longer OS than the median OS of the non-ACT group, which was regarded as the beneficiary population. This better survival in the ACT group could be partially attributed to decreased local recurrence and distant metastasis.31,32 It might be interpreted that the value of postoperative adjuvant chemotherapy could reduce the chances of recessive micrometastases. 33
In our visualized nomogram, age, gender, marital status, laterality, pathology, tumor size, regional nodes examined, and tumor size were primary predictive variables, providing individualized estimates of whether stage IB NSCLC patients could benefit from ACT. These factors were confirmed to be related to prognosis in previous research. Xu et al indicated that ACT improved survival in eighth edition stage IB NSCLC patients. Age, grade, lymph nodes examined, visceral pleural invasion, surgical method, and radiotherapy were significant factors. 25 Tu et al identified gender, age, grade, pathological subtype, visceral pleural invasion, tumor size, surgical procedure, and regional nodes examined as independent prognostic factors in stage IB NSCLC patients. 19 Previous research found an association between the examined lymph node count with survival.34-37 One reason could be that removing more lymph nodes would increase the likelihood of detecting metastatic lymph nodes and contribute to improved nodal staging accuracy. Some patients with the N0 stage might have a node-positive condition. This group of patients was less likely to receive ACT due to the underestimated tumor stage. The analysis also presented that the adenocarcinoma subtype and younger age could increase the benefit probability. Two recent studies observed that stage IB patients with adenocarcinoma subtype and more youthful age cohorts achieved better long-term prognoses compared with other pathological subtypes and older populations, which was in line with our research.19,25 Moreover, our research indicated that patients undergoing lobectomy could gain more benefit probability of ACT than sublobar resection. Lobectomy was associated with more lymph node excision during surgery, and thus, survival benefits might result from the extensive lymph node resection and the more chance of ACT.38,39
The model was assessed in the training and validation sets. The results of AUCs (.781, .772, and .851) and calibration curves presented reliable discrimination and calibration ability. Moreover, the DCA analysis indicated the good clinical value of the model. Certain individual conditions were crucial to selecting optimal candidates for ACT among stage IB patients. The combination of multiple predicting factors could provide a more reliable prediction than any simple single indicator. Thus, this exploratory study built an individualized prediction nomogram to identify ACT benefit candidates, which could assist clinicians in decision-making.
Limitation
Several limitations in the research should be concerned. First, detailed chemotherapy regimens weren’t recorded in the SEER database, so we couldn’t compare the effect among different chemotherapy regimens. Second, the lack of recurrence data prevented further comparison with other investigations. Also, the external validation cohort was relatively small and further external multicenter prospective validations were required.
Conclusion
Our research indicated that stage-IB NSCLC patients who underwent ACT presented longer median OS than the non-ACT cohort. The high-performing nomogram could guide decision-making and selecting optimal candidates for the ACT. But this conclusion came from American data, so external validation in other countries is required to verify the conclusion further.
Supplemental Material
Supplemental Material - A Novel Nomogram for Identifying Candidates for Adjuvant Chemotherapy in Patients With Stage IB Non-small Cell Lung Cancer
Supplemental Material for A Novel Nomogram for Identifying Candidates for Adjuvant Chemotherapy in Patients With Stage IB Non-small Cell Lung Cancer by Xue Song, Yangyang Xie, Haoran Deng, Fei Yu, Shiqiang Wang, and Yafang Lou in Cancer Control
Footnotes
Author Contributions
1. Study design: Xue Song, Yafang Lou.
2. Data collection: Xue Song, Yangyang Xie.
3. Statistical analysis: Xue Song, Haoran Deng.
4. Data interpretation: Xue Song, Fei Yu.
5. Literature search: Xue Song, Shiqiang Wang.
6. Manuscript writing: Xue Song, Yangyang Xie.
7. Final approval of manuscript: Yafang Lou.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The patient’s data acquired from the SEER database can be accessed publicly, so no ethical approval was needed. The project involving human participants was reviewed and approved by the Ethics Committee of Hangzhou TCM Hospital Affiliated to Zhejiang Chinese Medical University. In compliance with national law and institutional standards, written informed permission was not needed for participation in this study.
Data Availability
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.