
Abstract
Aim
Previous studies have provided evidence that primary site surgery can improve the prognosis of rectal cancer patients, even in those with advanced age and distant metastasis, though results have been inconsistent. The current study aims to determine if all rectal cancer patients are likely to benefit from surgery in terms of overall survival.
Methods
This study examined the impact of primary site surgery on the prognosis of rectal cancer patients diagnosed between 2010 and 2019 using multivariable Cox regression analysis. The study also stratified patients by age group, M stage, chemotherapy, radiotherapy, and number of distant metastatic organs. The propensity score matching method was used to balance observed covariates between patients who received and did not receive surgery. The Kaplan–Meier method was used to analyze the data, and the log-rank test was used to determine differences between patients who did and did not undergo surgery.
Results
The study included 76,941 rectal cancer patients, with a median survival of 81.0 months (95% CI: 79.2–82.8 months). Of these patients, 52,360 (68.1%) received primary site surgery, and they tended to be younger, have higher differentiated grade, earlier T, N, M stage, and lower rates of bone, brain, lung, and liver metastasis, chemotherapy, and radiotherapy than those without surgery. Multivariable Cox regression analysis revealed that surgery had a protective effect on the prognosis of rectal cancer patients, including those with advanced age, distant metastasis, and multiple organ metastasis, but not in patients with four organ metastases. The results were also confirmed using propensity score matching.
Conclusion
Not all rectal cancer patients could benefit from the surgery on the primary site, especially the patients with more than four distant metastases. The results could help the clinicians to tailor targeted treatment regimens and provide a guideline for making surgical decisions.
Introduction
Colorectal cancer is a prevalent cancer type and a leading cause of cancer-related deaths in the United States, with an estimated 147,950 new cases and 53,200 deaths in 2020. 1 Among these cases, rectal cancer accounts for approximately 30%, and the 5-year survival rate varies based on tumor stage. 2 The 5-year survival may decrease to about 20% when rectal cancer progresses to distant metastasis.3–5
Surgery is acknowledged as the cornerstone of rectal cancer treatment.6,7 A series of studies have suggested the improved prognosis of rectal cancer after surgery, even in patients with stage IV, including the increased overall survival rate, decreased distant recurrence rate, and prevention of complications.5,8,9 However, due to the relatively lower sample size incorporated into the studies, results were not so consistent.10,11 Moreover, due to the heterogeneity distribution of the clinical characteristics, furthermore, certain patient subgroups, such as those with advanced age or multiple organ metastases, may not benefit from surgery. But few studies have been published to systematically validate surgery’s effect on these patients.
National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) program, established in 1973, is an authoritative source of information on cancer incidence and survival in the United States. 12 The SEER database comprises approximately 30% of the US population, which routinely collect data on patient demographics, primary tumor site, tumor morphology and stage at diagnosis, the first course of treatment, and follow-up for vital status. It provides the basis for validating the associations between surgery and the prognosis in rectal cancer patients with relatively larger sample size and higher stability and reliability.
This study aims to examine whether surgery benefits all rectal cancer patients, including those with advanced age and multiple organ metastases, in order to develop individualized treatment strategies for rectal cancer.
Material and Methods
Study Population
International Classification of Diseases for Oncology, 3rd edition (ICD-O-3) codes confirmed malignant rectal cancer patients in this study were retrieved from the US National Cancer Institute (NCI) open public database, SEER database. The patients diagnosed between 2010 and 2019 with definite distant metastasis information were included. The data for metastatic organs such as bone, brain, liver, and lung started in 2010, and the latest data up to date was on December 31, 2019. SEER*Stat Software version 8.4.0.1 (https://seer.cancer.gov/seerstat/) (Information Management Service, Inc. Calverton, MD, USA) was used to generate the case listing.
Ethics Statement
Cancer is a reportable disease in the United States. The data in the SEER database does not require informed patient consent. This study used previously collected deidentified data, which was deemed exempt from review by the Ethics Board of the Ethics Committee of West China Fourth Hospital and West China School of Public Health, Sichuan University.
Statistical Analysis
Quantitative data were described as Mean ± standard deviation (SD). Categorical data were depicted as the number and the percentage (N, %), and the difference between groups with and without surgery was tested by chi-square or sum-rank test. Surgery on the primary site was defined as any type of rectal cancer resection, including partial colectomy, total colectomy, proctocolectomy, or proctectomy of the primary tumor. The primary outcome of our study was overall survival (OS), which was defined as the time from the diagnosis of rectal cancer to the date of all-cause death. The surgery trend and the year of diagnosis were assessed with the Cochran-Armitage trend test. 13 The multivariable Cox regression model was conducted to determine the associations between surgery and prognosis of the rectal cancer patients adjusted by age, sex, race, differentiated grade, T stage, N stage, M stage, chemotherapy and radiotherapy, the adjusted hazard ratios (HR), along with 95% confidence intervals (CIs) for describing the likelihood of surgery associated with OS. Stratified analysis was also conducted when stratified by age (≤60 years vs 61-80 years vs >80 years), M stage (M0 vs M1), chemotherapy (with vs without), radiotherapy (with vs without), and the metastatic organ numbers (1 site to 4 sites).
We used the propensity score matching (PSM) method to balance the covariables of age, sex, race, differentiated grade, T stage, N stage, M stage, chemotherapy, and radiotherapy between the subjects with and without surgery. 14 The propensity score distribution was plotted before and after PSM matching to verify the matching effectiveness. Overall survival was estimated using the Kaplan–Meier method, and the log-rank test compared the statistically significant differences between groups.
The IBM Statistical Package conducted statistical analyses for the Social Sciences (SPSS) version 23.0 software package for Windows (SPSS, Inc., Chicago, IL, USA). All ROC curves were conducted by MedCalc 18.2.1. Statistically significant levels were two-tailed and set at P < .05.
Results
Demographic and Clinical Characteristics
A total of 76,941 rectal cancer patients were finally included in the present study; the flow-chart of the population selection procedure is shown in Figure 1. Of these patients, 45,610 (59.3%) were males, and 31,331 (40.7%) were females; the mean age was 62.91 ± 13.24 years. A majority of the patients were White (N = 63,785, 76.1%), followed by Black (N = 8,943, 10.7%), Asian or Pacific Islander (N = 8,760, 10.5%), and American Indian/Alaska Native (N = 823, 1.0%). About 17.5% (N = 13,447) of the patients harbor distant metastasis. Of them, 1194 (1.6%) metastasis to bone metastasis, 203 (.3%) metastases to the brain, 9503 (12.4%) metastases to the liver, and 4760 (6.2%) were diagnosed with lung metastasis. 56.8% patients received chemotherapy and 48.3% received radiotherapy. The median survival of the patients was 81.0 months (95% CI: 79.2–82.8 months), 1-year, 3-year, and 5-year survival were 83.9%, 66.6%, and 56.2%, respectively. Flow-chart of the participant selection.
The Factors Associated With Surgery
For the included 76941 rectal cancer patients, about 68.1% underwent surgery on the primary site. Most racial groups were treated surgically, and Asian or Pacific Islander patients had a higher proportion of surgery (72.6%). In comparison, the Black harbor had the lowest surgery frequency (64.7%) (P for difference <.001). The frequency in patients with stage IV was relatively lower than in others (27.7% vs 77.4%; chi-square = 23692.30; P < .001). From 2010 to 2019, the frequency of the surgery significantly decreased with the year, and the decreasing trend was consistent when stratified by the M stage (chi-square = 162.85; P for trend <.001; Figure 2). The annual number of rectal cancer patients increased by about 2.5%, but the percentage of surgery decreased by about 10%. The surgery frequency and diagnostic year plot in the total population stratified by the M stage.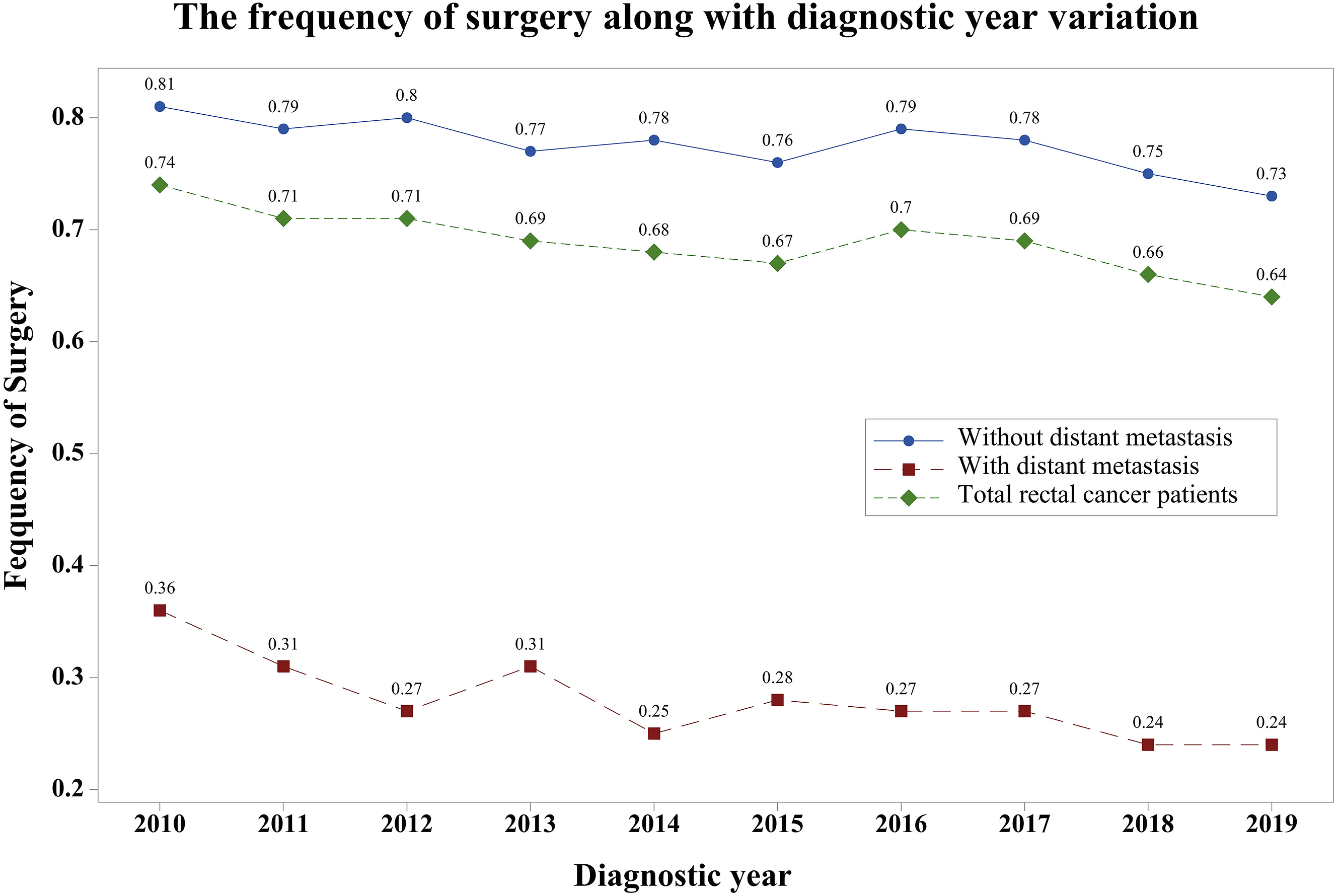
Differences in the Demographic and Clinical Characteristics Between the Rectal Cancer Patients with and Without Surgery in this Study.

The Effect of the Surgery on the Prognosis
The Associations Between Surgery and Prognosis of Rectal Cancer Patients in Total and Stratified by Different Metastatic Organ Number Subgroups.

aAdjusted by age, sex, race, differentiated grade, T stage, N stage, M stage, Chemotherapy and Radiotherapy.
When stratified by the age of the participants, the patients all identified to have significantly higher survival than the patients without surgery in the ≤60 age group (median survival: 27.00 months with surgery; P < .001); 61–80 age group (median survival: 114.00 months with surgery vs 19 months without surgery, P < .001) and >80 age groups (median survival: 45 months with surgery vs 10 months without surgery, P < .001). Multivariable Cox regression confirms the negative associations between the surgery and the death risk in all of these groups.
The results were consistent when stratified by the patients with M1 stage (HR = .47; 95% CI: .45–.50; P < .001) M0 stage (HR = .31; 95% CI: .30–.32; P < .001), with chemotherapy (HR = .31; 95% CI: .30–.32; P < .001), without chemotherapy (HR = .20; 95% CI: .20–.21; P < .001), with radiotherapy (HR = .32; 95% CI: .31–.34; P < .001), and without radiotherapy (HR = .20; 95% CI: .19–.21; P < .001).
For the patients with distant organ metastasis, surgery could significantly improve the prognosis for metastatic rectal cancer patients with less than three metastatic organs. (P < .001) Interestingly, for the metastatic rectal cancer patients with four organ metastases, multivariable Cox regression showed no significant associations between surgery and the mortality risk (median survival: 2 months with surgery vs 5 months without surgery, P = .95; HR = .12; 95% CI: .02–9.67; P = .12). (Table 2)
Propensity Score Matching suggested that the overall propensity score distribution in patients with and without surgery was comparable in all subgroups after matching. The distribution of the propensity before and after matching in total rectal cancer patients and stratified by age, metastatic status, and number of the metastatic organs are listed in the Online Appendix file. Results showed rectal cancer patients with surgery exhibited a better OS than those who did not receive surgery (chi-square = 6231.21; P < .001) (Figure 3A). When further stratified by the age group, M stage, and the number of metastatic organs, results suggested all of the patients could benefit from the surgery (Figure 3B-I), but not the patients with four metastatic organs (chi-square = 1.50; P = .221) (Figure 3J). Survival plot for testing the difference in the prognosis in patients with and without surgery after PSM matching in the total population (A), patients with ≤60 years (B), patients with 61–80 years (C), patients with >80 years (D), patients with M0 stage (E), patients with M1 stage (F), patients with one organ metastasis (G), patients with two organs metastases (H), patients with three organ metastases (I), patients with four organs metastases (J).
Discussion
The present study used the SEER database to investigate the effect of the surgery on the prognosis of rectal cancer. The results found that surgery on the primary could prolong the survival of rectal cancer patients, no matter in patients with advanced ages and with three or fewer organ metastasis. However, rectal cancer patients with four organ metastases could not benefit from the surgery. The results could provide a precise surgical treatment strategy for rectal cancer patients.
Results suggested the rectal cancer patients underwent surgery present to be diagnosed with relatively earlier year. The diagnosed age distribution may play an important role. In this study, the diagnosed age of the patients were significantly increased with year (P < .001). As it is reported that, the elderly patients may have decreased odds of receiving cancer directed surgery.15,16 The reason was not clear yet. The inadequate preoperative evaluation and perceived increased operative risk for these elder patients may partly explain the results.15,16
The study was based on a retrospective real-world study; we inevitably encounter the problem of controlling confounding factors. The present study suggested the distribution of the age, differentiated grade, T stage, N stage, M stage, and metastatic organ number showed marked differences between the patients with and without surgery, which was consistent with the previous studies.17,18 Many methods such as multivariable Cox regression and instrumental variable method were recommended to adjust the effect of these confounding factors. However, none of these methods alone could entirely avoid the bias.19,20 In this study, the multivariable Cox regression and PSM method were adopted to verify the benefit of the surgery on prognosis in different subgroups. Thus, the reliability of the results was improved.
A series of studies suggested that surgery could prolong the prognosis of rectal cancer patients. Based on 10,796 rectal cancer patients with stage I–III who underwent tumor resection, Guren and colleagues suggested the five-year survival improved from 1993–1997 to 2007–2010. 21 Zhang and colleagues conducted a pan-cancer analysis of the prognostic factors for metastatic cancer. They suggested the surgery was negatively associated with all causes of death risk for metastatic rectal cancers after adjusting for age, sex, and other clinical characteristics. 22 Consistent with these studies, our study also confirmed negative associations between surgery on the primary site and all causes of mortality, even in patients with distant metastasis and patients with advanced age (>80 years). We also suggest the surgery could not prolong the survival in patients with four organ metastasis. Another study with 158 stage IV colorectal cancer patients indicated that resectioning the primary tumor in asymptomatic stage IV does not affect survival.11,23 The results may be partly explained by the relatively poor prognosis and smaller sample size. Previous studies suggest that distant organ metastasis could markedly decrease the overall survival of cancer patients, and a dose-response relationship between the metastatic organs and the prognosis was observed.24,25 A total of 25 rectal cancer patients with four organ metastases were included in the final analysis, and the median survival was estimated to be about 5 months. Statistical power was not sufficient to detect a significant difference.
The present study has some limitations. First, as reported in the SEER database, the SEER database does not capture information about surgery four months after the diagnosis. Thus, the results should be explained with caution as the patients without surgery may undergo surgical treatment and therefore underestimate the effect of the surgery. Second, as the SEER database did not differentiate between different surgical methods, which may affect patients’ prognosis. Therefore, we cannot overinterpret which surgical procedure has an effect on prognosis. Third, the present study adjusted the treatment means, but caution should be exercised in interpreting the results due to reported sensitivities of 80% for radiation therapy and 68% for chemotherapy acquired from the SEER database. 26 Fourth, the choice of receiving surgery is not only determined by the tumor characteristics of the patients but also the patients’ preferences. However, the database could not capture the patients’ intentions, which may affect the results. Fifth, the primary endpoint of this study was OS, and we did not consider the relief of the local symptoms or the quality of life. Although little evidence suggests surgery could prolong the survival in patients with four organ metastases, they may benefit from the symptom relief. Thus, the results should be explained cautiously.
The present study suggested most rectal cancer patients received surgery after diagnosis. A series of clinical factors such as age, T stage, N stage, and M stage were associated with the surgery. The surgery on the primary site could significantly increase the prognosis of the patients, no matter in patients with different age subgroups and three or fewer organ metastasis. However, rectal cancer patients could not benefit from the surgery in patients with four organ metastases. Thus, surgical treatment should be recommended if the patient meets the indications for surgery and have willing to undergo surgery, except for the patient with four organ metastases. The results could help the clinicians to tailor target treatment regimens to the patients in the clinical practice.
Supplemental Material
Supplemental Material - Not all Rectal Cancer Patients Could Benefit From the Surgery on the Primary Site
Supplemental Material for Not all Rectal Cancer Patients Could Benefit From the Surgery on the Primary Site by Jin Zhou, Wenqian Yu, Jing Xia, Shiyi Li, Linshen Xie, and Xin Wang in Cancer Control
Footnotes
Acknowledgments
The study was supported by the National Natural Science Foundation of China (81903398), The research start-up fund for the introduction of talents of Sichuan University (YJ2021112), Medical youth Innovation research project of Sichuan Province (Q21016).
Author Contributions
JZ: conceptualization, data collection, and investigation, writing original draft, critical revision. WQY: methodology, assisted in the conceptualization, formal analysis, and contributed to the draft writing. JX: software, imaging analysis and the related draft revision. SYL: contributed to the methodology, writing, and data curation. XW: validation, data curation, and project administration. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the National Natural Science Foundation of China (81903398), The research start-up fund for the introduction of talents of Sichuan University (YJ2021112), Medical youth Innovation research project of Sichuan Province (Q21016).
Ethics Approval
Cancer is a reportable disease in the United States. The data in the SEER database does not require informed patient consent. This study used previously collected deidentified data, which was deemed exempt from review by the Ethics Board of the Ethics Committee of West China Fourth Hospital and West China School of Public Health, Sichuan University.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.