
Abstract
Objective
It remains unclear whether primary tumor resection improves survival in patients with metastatic Siewert type II adenocarcinoma of the esophagogastric junction (AEG). Therefore, our study attempted to investigate the prognostic value of primary tumor resection on metastatic AEG.
Methods
In total, 4200 patients diagnosed with metastatic AEG were retrieved from the Surveillance, Epidemiology, and End Results (SEER) database from 2004 to 2015. Patients were categorized into two groups according to the performance of primary tumor resection. Pearson’s chi-square test, Kaplan–Meier survival curve, and Cox regression analysis were conducted in this study. In addition, propensity-score matching was conducted to match 323 patients who received primary tumor resection and another 323 patients without.
Results
Multivariate Cox regression analysis demonstrated that primary tumor resection was a significant prognostic factor in patients with metastatic AEG before matching. Moreover, in the matched cohort, metastatic AEG patients receiving primary tumor resection had significantly longer overall survival (hazard ratio [HR]: .54, 95% confidence interval [CI]: .46–.64, P < .001) and cancer-specific survival (HR: .53, 95% CI: .45–.63, P < .001). Subgroup analysis similarly revealed that primary tumor resection was significantly associated with better survival in most subgroups.
Conclusion
The present population-based study identified that primary tumor resection led to significantly superior survival in patients with metastatic AEG. These findings are likely to contribute to the development of individualized therapy in metastatic AEG.
Keywords
Introduction
Adenocarcinoma of the esophagogastric junction (AEG) is relatively rare but highly aggressive, 1 being a great health threat worldwide. The classification of AEG lacks a single standard system due to its special anatomical location, 2 and each subtype exerts different clinicopathological properties. 3 The Siewert classification divides AEG into three types based on the endoscopic location of tumor epicenter relative to the esophagogastric junction (EGJ): Siewert type I (5 to 1 cm above the EGJ), type II (1 cm above to 2 cm below the EGJ), and type III (2 to 5 cm below the EGJ).4,5 While Siewert type II is widely considered as the true cardia carcinoma arising from the esophagogastric junction.5,6
The proportion of metastatic patients at diagnosis in AEG is not uniformly reported by large-scale studies. A recent study reports that approximately 30% of AEG patients are diagnosed with metastasis. 7 The 5-year overall survival (OS) of patients with distant metastasis is lower than 10%. 8 According to the present guidelines from the National Comprehensive Cancer Network (NCCN), the standard therapeutic algorithm for patients with metastatic AEG is palliative systemic therapy combined with best supportive care.9,10 Cytotoxic agents mainly include fluoropyrimidine, platinum, irinotecan, and taxanes. 11 Moreover, molecularly targeted drugs (mainly trastuzumab and ramucirumab) and immunotherapy have also been confirmed to bring survival benefit. 11
However, chemotherapy generally gives rise to unsatisfactory efficacy in the long run, 12 and systemic therapy alone cannot eradicate the primary tumor lesion. Therefore, it is rationale to selectively apply local consolidation (including consolidation chemoradiation and surgery) to improve the long-term prognosis. In other types of malignant tumors, local therapy of the primary tumor lesion has been reported to decrease overall tumor burden and alleviate potential local compression.13,14 However, the prognostic value of primary tumor resection on patients with metastatic AEG remains an open question. Therefore, we attempted to investigate whether primary tumor resection in metastatic AEG was associated with patient survival by extracting eligible patients from the Surveillance, Epidemiology, and End Results (SEER) database in this retrospective study.
Materials and Methods
Data Source and Study Population
Our study cohort was retrieved from the National Cancer Institute’s SEER program. The SEER program includes 18 registries covering approximately 30% of the US population, which is considered as an authoritative source containing information on patient demographics, tumor features, and primary treatment modality. 15 Since the SEER database is publicly available and de-identified, no approval was required from the local ethics committee.
The detailed identification criteria of Siewert type II AEG were described in our previous study. 16 In summary, eligible Siewert type II AEG patients could be identified by using a combination of “TNM 7/CS v0204+ Schema” encoded 28 (EsophagusGEJunction) and “Primary Site – Labelled” encoded 160 (Cardia, NOS). Patients with Siewert type II AEG were downloaded from the SEER database between 2004 and 2015. Patients with metastatic AEG were determined based on the following inclusion criteria: 1) metastatic AEG patients older than/of 18 years; 2) ICD-0-3 code within the range of 8140–8145, 8210–8211, 8220–8221, 8255, 8260–8263, 8310, 8480–8481, and 8490; 3) positive histological diagnosis; 4) active follow-up; 5) survival of or over 1 month; 6) only one or the first one in the case of synchronous other cancers; and 7) available information of local treatment to the primary tumor. Based on the inclusion criteria, 4200 eligible patients were included in this retrospective study. The flow chart of patient selection is shown in Supplementary Figure 1.
Patient demographics (age at diagnosis, sex, race, and marital status), tumor characteristics (tumor grade, tumor size, T stage, N stage, and metastatic site), treatment modality, and patient survival were collected for further analysis.
Propensity-Score Matching
Selection bias is inevitable in retrospective studies due to unbalanced baseline clinicopathological parameters. To attenuate selection bias along with unevenly distributed covariates, propensity-score matching (PSM) was further performed. The definition of propensity score is the conditional probability of assignment to a particular treatment given a vector of observed covariates. 17 Patients receiving primary tumor resection were matched with those not receiving by PSM using 1:1 nearest neighbor matching with a caliper of .05. After matching, standardized difference (SD) of each covariate was calculated to compare the similarity between two groups. And the absolute value <.1 indicated that covariates were well balanced between two groups.
Statistical Analysis
Outcomes of interest included OS and cancer-specific death (CSS). Patients were assigned into two groups based on the performance of primary tumor resection. Survival curves were plotted by Kaplan–Meier method between the primary tumor resection group and no primary tumor resection group before and after PSM. Possible survival difference between the two groups was determined by log-rank test. Univariate Cox regression analysis was used to investigate potential prognostic factors, and variables with P-value <.05 in univariate analysis were incorporated into multivariate analysis. Results were shown as hazard ratios (HRs) and its 95% confidence intervals (CIs). R software for Mac version 3.6.1 (The R Foundation for Statistical Computing, Vienna, Austria) was utilized for data analysis and representation. A two-sided P-value <.05 was suggestive of statistical significance.
Results
Baseline Characteristics of Patients
Baseline Characteristics of Patients (N = 4200).

Survival Analysis and Prognostic Factors in Unmatched Patients
We further investigated possible survival difference between patients undergoing primary tumor resection and patients without resection. Kaplan–Meier curves were plotted in unmatched patients stratified by the status of primary tumor resection. As shown in Figure 1(A) and 1(B), patients receiving primary tumor resection had significantly better OS and CSS rates than those who did not receive (both P < .0001). The 5-year OS rate was 2.92% and 13.73% in the no local resection group and local resection group, respectively (Figure 1(A)). And the 5-year CSS rate was 3.49% and 14.70% in the no local resection group and local resection group, respectively (Figure 1(B)). Kaplan–Meier curves for (A) overall survival and (B) cancer-specific survival according to the status of primary tumor resection in the unmatched population.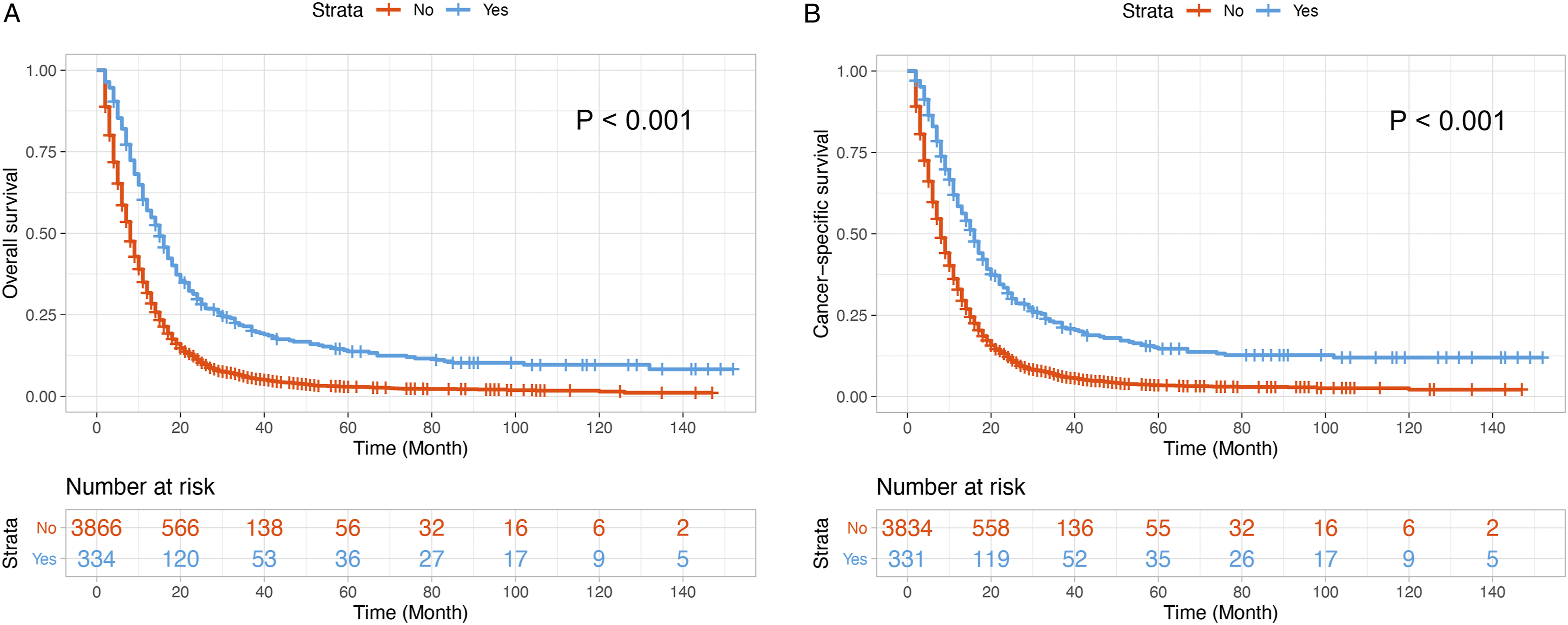
Prognostic Factors for Overall Survival (OS) and Cancer-Specific Survival (CSS) by Cox Regression Model Before Matching.


Forest plot for subgroup analysis in the unmatched population. Patients were divided into subgroups according to different clinicopathological characteristics. Patients undergoing primary tumor resection had better (A) overall survival and (B) cancer-specific survival in almost all subgroups.
Survival Analysis and Prognostic Factors in Matched Patients
In order to balance the covariates between the no local treatment and local treatment group, a 1:1 propensity-score matching was performed, which identified 646 matched patients (323 patients in each group). As shown in Supplementary Table 1, the SD values of various clinicopathological variables were decreased after matching. Except for T stage (SD = .111), the distribution of age, race, sex, marital status, tumor grade, tumor size, N stage, radiation, chemotherapy, and number of metastatic site was well balanced between the no primary tumor resection group and primary tumor resection group (all SD < .1).
Prognostic Factors for Overall Survival (OS) and Cancer-Specific Survival (CSS) by Cox Regression Model After Matching.
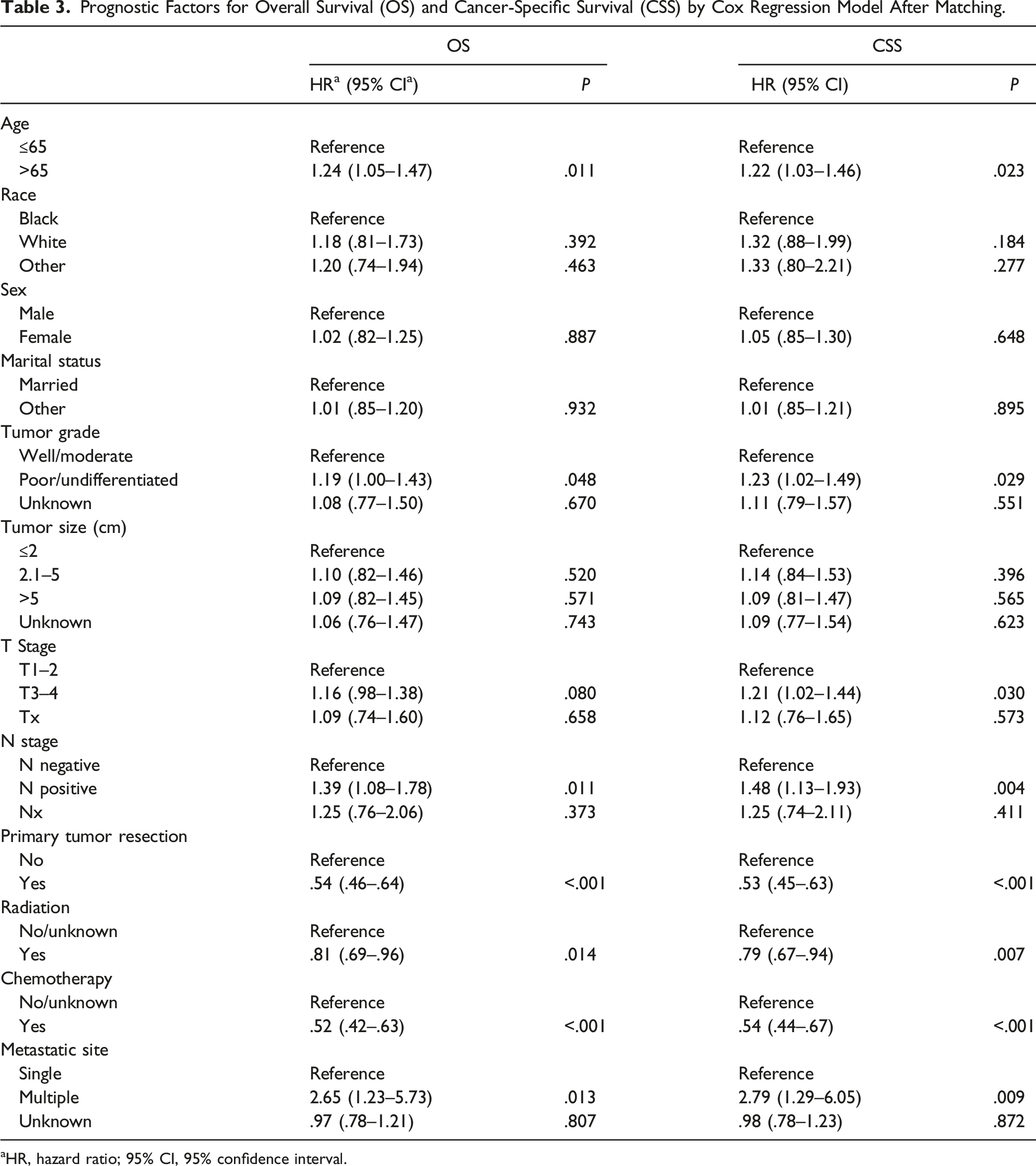
aHR, hazard ratio; 95% CI, 95% confidence interval.

Kaplan–Meier cohort selection curves for (A) overall survival and (B) cancer-specific survival according to the status of primary tumor resection in the matched population.

Forest plot for subgroup analysis in the matched cohort. Patients were divided into subgroups based on different clinicopathological characteristics. Patients receiving primary tumor resection had better (A) overall survival and (B) cancer-specific survival in most subgroups.
Discussion
In the present study, we examined the influence of primary tumor resection on patient survival in metastatic AEG. This population-based analysis revealed that primary tumor resection could prolong the survival of patients with metastatic AEG. This finding was further supported by PSM analysis to avoid possible confounding factors, which consistently showed better survival in patients undergoing primary tumor resection in the matched group. Subgroup analysis robustly suggested the superior survival outcomes in patients undergoing primary tumor resection than those without in most subgroups.
Given the rarity of this malignancy, only a few existing studies have compared the survival difference between primary tumor resection and palliative chemotherapy in stage IV gastroesophageal adenocarcinoma. Most of the studies have reported the survival benefit by surgical resection of primary tumor.18-21 Notably, in a phase II clinical trial enrolling 252 patients with resectable or metastatic gastric or gastroesophageal junction adenocarcinoma, Salah-Eddin Al-Batran et al 22 revealed that neoadjuvant chemotherapy followed by surgical resection showed a favorable survival. However, these studies have small sample size and investigate gastric cancer, esophageal carcinoma, AEG, or all of them. To our knowledge, this is the first large population-based analysis investigating the significance of primary tumor resection in metastatic AEG management. As the one of the largest clinical databases, the SEER database compensates for the low number of metastatic AEG cases, which renders our present findings more convincing.
The performance of chemotherapy and distant metastatic pattern were taken into consideration in PSM analysis, which is one of the noteworthy features of our study. According to the present clinical guidelines and clinical studies, systemic therapy is the mainstay in the standard clinical management of metastatic AEG 11 and the pattern of distant metastatic organs definitely affects prognosis. 23 As expected, significantly prolonged survival was detected in patients receiving chemotherapy than those without chemotherapy in both unmatched and matched cohorts. The number of metastatic sites and the specific site of distant metastasis have been demonstrated as independent prognostic factors in patients with stage IV AEG. 7 Therefore, the number of metastatic sites and distant metastatic organs were also matched by using PSM in the present analysis to alleviate potential biases. Here, we similarly found that the number of metastatic sites was significantly associated with patient survival. A novel finding was that only AEG patients with single metastatic site could gain survival from primary tumor resection, possibly due to the relatively small sample of patients with multiple metastatic sites.
In this study, we proposed that surgical resection of the primary tumor lesion could improve patient survival in metastatic AEG, which is consistent with the findings in other types of malignant tumors localized in the digestive tract. In a cohort from MD Anderson Cancer Center, patients with metastatic gastroesophageal adenocarcinoma (including adenocarcinoma of the esophagus or stomach and AEG) first received systemic therapy and were further treated by consolidative local therapy (local consolidation chemoradiation, surgery, or both). 8 As a result, surgery (as local consolidation) was an independent prognostic factor for longer OS in the multivariate analysis. Moreover, they also found that patients undergoing surgery were 63% less likely to die compared to those untreated ones according to the multivariate Cox proportional hazards model. Zhang et al 24 reported the positive correlation between primary tumor resection and survival outcome among patients with metastatic rectal cancer. Similarly, to investigate the significance of palliative primary tumor resection on survival among patients with metastatic colorectal cancer, a previous study indicated that palliative resection of the primary lesion gave rise to significantly prolonged survival. 23
However, the resection of primary tumor lesion can also give rise to several possible risks. Both endoscopic resection and surgery might delay the performance of systemic treatment, especially in the case of severe post-operative complications. 25 Although surgical resection is the only curative intervention in most types of malignancies, existing studies suggest that surgery might be associated with tumor progression. 26 For one thing, surgical resection potentially enhances metastatic seeding of tumor cells and increases the formation of new metastatic niche. For another thing, surgical stress (including trauma, ischemia/reperfusion injury, inflammatory response, and immune suppression) might promote tumor progression. 27 Therefore, primary tumor resection should be applied in cautiously selected patients, and multidisciplinary assessment should be performed to establish personalized therapeutic strategies in metastatic AEG patients.28,29
One of the limitations of this study is selection bias, which might be inevitable in retrospective studies. Here, we performed PSM analysis to match unbalanced baseline clinicopathological parameters. Second, the detailed information of chemotherapy (regimen and dose) and radiotherapy (dose) was inaccessible from the SEER database, which might also affect patient prognosis.
Conclusion
In summary, in this large population-based and propensity-matched study, we demonstrated that surgical resection of the primary tumor lesion could significantly prolong patient survival. In consideration of the possible post-operative complications and medical cost, multidisciplinary evaluation should be conducted to provide individualized clinical decisions.
Supplemental Material
Supplemental Material - Influence of Primary Tumor Resection on Survival of Patients With Metastatic Siewert Type II Adenocarcinoma of the Esophagogastric Junction: A Population-Based, Propensity-Matched Analysis
Supplemental Material for Influence of Primary Tumor Resection on Survival of Patients With Metastatic Siewert Type II Adenocarcinoma of the Esophagogastric Junction: A Population-Based, Propensity-Matched Analysis by Jiamin Chen, Xuan Jia, MM, Hanwen Chen, Jianting Cai, and Liubo Chen in Cancer Control.
Ethical statement
Ethical Approval
Since SEER database is publicly available and re-identified, approval was waived by the local ethics committee (the Second Affiliated Hospital, Zhejiang University School of Medicine) in this retrospective study. Written informed consent is not required in this retrospective analysis.
Footnotes
Acknowledgments
The authors are grateful for the efforts of the SEER program in creating and maintaining the SEER database.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Zhejiang Provincial Department of Health (No. 2018KY083).
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.