
Abstract
Objective
To obtain breast cancer survival estimates in Manizales, Colombia, considering socioeconomic level, health insurance regime and residential area, while adjusting for age, histology and stage at diagnosis.
Methods
Analytical cohort study based on breast cancer incident cases recorded by the Population-based Manizales Cancer Registry between 2008-2015. Patients were followed-up for 60 months. Cause-specific survival was calculated using the Kaplan-Meier method for variables of interest, with the Wilcoxon-Breslow-Gehan test for differences. Cox multivariate regression models were fitted.
Results
856 breast cancer cases were included. The 5-year cause-specific survival for the entire cohort was 78.2%. It was higher in women with special/exception health insurance, high socioeconomic level, <50 years old, ductal carcinoma, and stages I and II. Residential area did not impact survival. In Cox models, the subsidized health insurance regime (HR: 4.87 vs contributory) and low socioeconomic level (HR: 2.45 vs high) were predictors of the hazard of death in women with breast cancer, adjusted for age, histology, stage and interactions age-stage and insurance-stage. A positive interaction (synergistic effect modification) between health insurance regime and stage regarding to survival was observed.
Conclusion
Socioeconomic factors significantly contribute to the inequities in breast cancer survival, independent of the stage at diagnosis. This suggests the need for comprehensive interventions to remove barriers to accessing the health system. This research provides evidence of survival gaps mediated by certain social determinants of health and generates data on the overall performance of the Colombian health system.
Introduction
Breast cancer (BC) is the leading cause of cancer incidence and mortality among women globally, showcasing notable disparities in its impact across countries based on their development status. Developing nations despite experiencing low incidence, grapple with elevated mortality, whereas developed countries observe the converse trend. 1 In light of the anticipated surge in cancer cases by 2040, which is expected to be most striking in developing countries, 1 the imperative for cancer surveillance and the adaptation of cancer healthcare services becomes unmistakable. Consequently, population-based cancer registries (PBCR) facilitate the comprehensive monitoring of this disease in across entire populations and enable the evaluation of healthcare services efficacy through the estimation of cancer survival. This measurement not only reflects the prognosis of the disease but also underscores the influence of health determinants.2-4
Based on the findings of the CONCORD-3 study, 5 it has been observed that BC survival estimates also differ between regions and countries. In North America and Oceania, the 5-year survival stands at approximately 90%, whereas in most Central and South American countries, it falls short of 80%. Notably, there exists a substantial variability in survival figures within these countries. For instance, during the period 2010-2014, BC survival was 72.1% in Colombia and 86.7% in Costa Rica. 5 A prior investigation conducted in Manizales, Colombia, reported an observed 5-year survival of 71% for women diagnosed with BC between 2003 and 2007. 6
According to the World Health Organization (WHO), unnecessary, avoidable and unfair inequalities, configure the concept of health inequities. 7 In BC, these inequities are expressed both in the risk of developing BC and in the possibility of accessing early diagnosis and opportune treatment. As Woods et al 8 point out, cancer stage at diagnosis has been shown to be a key factor explaining differences in cancer survival –including BC– across different populations. While this factor explains, in turn, much of the socio-economic differences in survival, has been insufficient to explain all of them. Woods et al 8 suggest that placing exclusive emphasis on the stage of disease is likely to be overly simplistic if we aspire to fully comprehend the inequalities in survival. 8
Thus, with information sourced from the PBCR of the city, the aim of this research is to derive survival estimates for BC in Manizales, accounting for socioeconomic level, health insurance regime, and residential area. These estimates will be adjusted for variables such as age, histology, and stage. In addition, this research seeks to contribute to the assessment of health inequities and to the evaluate the Decennial Plan for Cancer Control in Colombia. 9
Materials and Methods
An analytical population-based cohort study was conducted in Manizales, Colombia, an Andean city with a population of 434 403 inhabitants (52.9% women), according to the National Household and Population Census, 2018. 10
Inclusion criteria: all BC cases in women residing in Manizales, diagnosed between January 1, 2008, and December 31, 2015, were included. These cases were extracted from the Population-based Manizales Cancer Registry (MCR) database, utilizing topographical codes corresponding to breast (C50.0–C50.9) in the International Classification of Diseases for Oncology, third edition (ICD-O3). 11 Population-based studies, by definition, encompass a census of all cases diagnosed in the study area; therefore, all BC cases in women were included, and no sampling methodology was applied in this study.
Exclusion criteria: BC cases in men (n = 4), non-residents in Manizales (n = 25), as well as benign, uncertain and in situ neoplasms (n = 11), were excluded.
Since the date of diagnosis, cases were passively followed-up for 60 months or until June 30th 2021, to identify the event (death due to BC) and the time-to-event. Using personal identity numbers, the vital status of the patients was verified in government databases (health insurance registries and electoral census). Subsequently, those identified as deceased were cross-referenced on the vital statistics platform (RUAF-ND, by its acronym in Spanish) of the National Administrative Department of Statistics (DANE, by its acronym in Spanish) in order to obtain the date and cause of death directly from death certificates. Access to this information was facilitated by the local health authority’s vital statistics office. Cases that did not present the event by the end of the follow-up, those who died from other causes, or cases where the cause of death could not be verified, along with any losses to follow-up, were censored. BC cases captured by death certificate only (DCO) (n = 5), were excluded for multivariate analysis.
Socio-demographic variables: in Colombia, there exists a universal health insurance system that provides coverage to 97.7% of the population (cut-off year: 2020). Within this system, individuals are allocated to different schemes, referred to as health insurance regimes (HIR). The assignment is based on their income and employment status, comprising contributory (encompassing workers and their families, constituting 73.5% of the population in Manizales); subsidized (catering to the vulnerable population or ‘poor’, accounting for 18.2% in Manizales), special and exception (pertaining workers in the education sector, police and military, making up 2.4% in Manizales). Additionally, there is a small percentage of population without insurance (5.9% in Manizales). 12 This investigation gathered HIR information from clinic histories.
In addition, the characteristics of dwellings and neighborhoods play a pivotal role in determining the socioeconomic stratum (SS) of individuals in Colombia, an indicator comparable to socioeconomic level (SL). Consequently, there are 6 SSs, ranging from 1 –the least affluent– to 6 –the most affluent–. In our research, we grouped this variable into 3 categories based on prior local-level articles6,13: SS 1-2 classified as ‘low’; 3-4, as ‘middle’; and 5-6 as ‘high’. Patient addresses were utilized to identify their neighborhoods, and each neighborhood was then matched to its corresponding SS, based on the predominant SS information for neighborhoods in Manizales, as previously determined by local authorities.
Information regarding age and residential area was obtained from the MCR database. The variable ‘age’ was categorized in 3 groups following the recommendations for BC screening in Colombia: <50 years old, 50-69 years old (the target group for BC screening by biennial mammography), and 70 years and older. The median age of the data was assigned to cases with unknown age (n = 8) trough simple imputation. Addresses were used to establish the residential area (RA) of the cases, classifying them as urban and rural.
Histological and clinical variables: concerning the most valid basis of diagnosis (a quality indicator of PBCRs, as per the International Agency for Research on Cancer), 90.4% (n = 774) of cases were microscopically verified, representing an optimal figure. From the MCR database, ICD-O3 histological subtype codes were collected. The histological subtypes obtained were pooled into 2 categories for analysis: ductal carcinoma and ‘others and unspecified’. To determine the patients’ cancer stage at diagnosis, clinic histories and pathological reports were consulted, and the American Joint Committee on Cancer seventh edition criteria were applied. 14
Bias control: in Manizales, all deaths are certified by physicians, with a certification accuracy of 96.4% for total deaths and 93.2% for cancer deaths. 15 Due to the availability of information regarding the cause of death, high-quality death certification, and a low probability of misclassification, cause-specific survival was used to estimate BC survival.
Statistical methods: 5-year (and annual) BC cause-specific survival probabilities by age, HIR, SL, RA, histological subtype, and BC stage at diagnosis, were calculated using Kaplan-Meier functions. The Wilcoxon-Breslow-Gehan (WBG) test was employed for comparisons. For the multivariate analysis, the HIR variable was categorized into 2 groups: contributory, special, and exception vs subsidized and non-affiliated. RA was not included due to the low number of cases from rural areas. To obtain estimates (adjusted and non-adjusted hazard ratios –HR–) of the variables’ effect on BC survival, Cox regression models were fitted as follows: (i) an unadjusted (crude) model; (ii) an adjusted model including SL and HIR (2 groups) as independent variables, and age, histological subtype and BC stage as adjustment variables; and (iii) an adjusted model with interactions terms: 2 multiplicative terms for the interactions between HIR*stage and age*stage were included to consider the influence of screening (targeting the 50-69 age group) on stage and potential differences between HIRs regarding access to screening and, consequently, cancer stage. The proportional-hazards assumption was assessed with the Schoenfeld’s residuals test. Statistical analysis was performed in Stata 14.2® (StataCorp, College Station, TX, USA).
Ethics statement: this investigation was considered as a minimal risk research (according to the Resolution 8430-1993 from the Ministry of Health of Colombia) and approved by the Bioethics Committee of the Facultad de Ciencias para la Salud, Universidad de Caldas (act N° 007 of 2021). The reporting of this study conforms to STROBE guidelines. 16
Results
For this study, we included 856 incident cases of women residing in Manizales, Colombia, diagnosed with BC between 2008 and 2015. The median age at diagnosis was 58 years old (IQR: 19 years). Approximately half of the cases (51.2%; n = 438) occurred in women belonging to the target group for BC screening in Colombia (50-69 years old). There were 221 cases (25.8%) in women under 50 years of age. Nine out of ten women diagnosed with BC lived in urban areas at the time of diagnosis. Two-thirds (64%; n = 540) of women belonged to the middle SL. Regarding to the HIR at diagnosis, 3 out of 4 women (77%; n = 656) were affiliated to the contributory regime, 16% (n = 140) to the subsidized regime, and only 14 patients (2.0%) belonged to special or exceptional regime. The predominant morphology (79%; n = 678) was infiltrating ductal carcinoma.
Distribution of Early and Late Diagnosed Cases by Socioeconomic, Clinical, and Histological Variables. Manizales, 2008-2015.
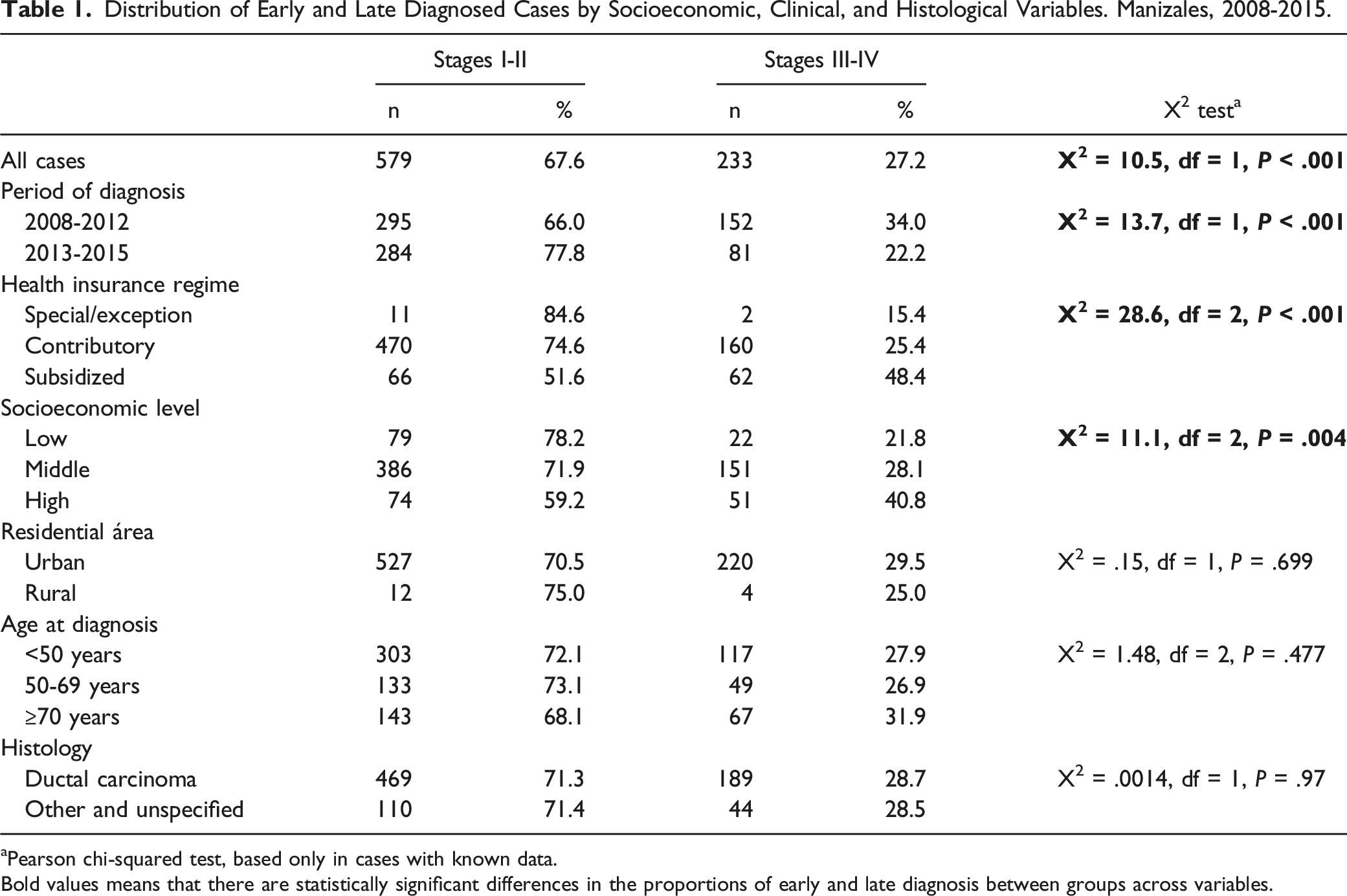
aPearson chi-squared test, based only in cases with known data.
Bold values means that there are statistically significant differences in the proportions of early and late diagnosis between groups across variables.
BC Cause-specific Survival by Socioeconomic, Clinical and Histological Variables. Manizales, 2008-2015.

aWBG: Wilcoxon-Breslow-Gehan test.
bA test based only in cases with known data.
Bold values means that there are statistically significant differences in the proportions of early and late diagnosis between groups across variables.
Women affiliated to the subsidized HIR exhibited consistently lower survival probabilities across all analyzed time points. Their 5-year cause-specific survival was 36.6 and 26.3 percentage points lower than women affiliated to special/exception and contributory HIRs, respectively. Regarding to SL, women from low SL had a 5-year cause-specific survival that was 18.9 and 9.0 percentage points lower than those from high and middle SL, respectively. Survival rates for women residing in rural areas were nearly 10 percentage points lower than those in urban areas, although this difference did not reach statistical significance (given this finding and the low number of rural cases, this variable was not included in the multivariate analysis). As expected, lower survival proportions were associated with advanced age (70 years or older), histological types other than ductal carcinoma, and an advanced stage at diagnosis.
Stratified analysis based on the opportunity of diagnosis (early vs late) revealed divergent outcomes among women in the same diagnostic categories, influenced by socioeconomic factors. BC survival in women of the subsidized HIR with late diagnosis (37.1%) was significantly lower than that of the women of the contributory (61.0%) and special/exception (100%) HIRs (WBG test = 13.74; df = 2; P = .001). Similarly, low SL women with late diagnosis (41.1%) were less likely to survive compared to middle (57.2%) and high SL (71.7%) women (WBG test = 6.90; df = 2; P = .031). Even women diagnosed early exhibited different outcomes depending on their HIR: survival in the subsidized HIR (76.0%) was lower than that in the contributory (89.5%) and special/exception (90.9%) HIRs (WBG test = 11.41; df = 2; P = .003). No association between survival and SL in women diagnosed early was observed (low: 87.5%; middle: 87.8%; high: 94.5%; WBG test = 3.15; df = 2; P = .207). No differences were found by RA in this stratified analysis.
Proportional Risks Models for BC Cause-specific Survival in Manizales, 2008-2015.

aLikelihood ratio (df = 9) = 169.78; P < .001. Age, histology and stage included as adjustment variables.
bLikelihood ratio (df = 18) = 179.64; P < .001. Interactions terms included: HIR*stage and age*stage.
cContributory, special, and exception HIRs.
dSubsidized HIR and non-affiliated.
Bold values means that there are statistically significant differences in the proportions of early and late diagnosis between groups across variables.
Abbreviations: HR: hazard ratio; CI: confidence interval; REF: reference; HIR: health insurance regime; SL: socioeconomic level; RA: residential area.
The univariate Cox regression model indicated significant effects of HIR, SL, age, histology, and stage on BC survival. Regarding the HIR, the univariate model showed that the instantaneous hazard of dying from BC within the 5 years after diagnosis was 3 times higher for women of the subsidized HIR or non-affiliated compared to those in the contributory, special, and exception HIRs. Adjusting for SL, age, histology and stage, reduced the magnitude of this effect to a HR of 1.97 but it remained statistically significant, indicating that the HIR effect was independent. The inclusion of interaction terms increased the HR of this association more than 2-fold (table 3).
Similar findings were observed for the SL: compared to high SL women, middle and low SL women had 2-fold and 3-fold higher hazards, respectively. The effect remained significant when adjusting for the mentioned variables, and the inclusion of interaction terms minimally affected the estimates (less than 10%).
Discussion
This research presents updated population-based BC survival estimations in Manizales, Colombia –a mid-size city from a middle-income country in South America–. Simultaneously, it offers results from an analysis of health inequities, using RA, HIR and SL as predictor variables; the estimations are adjusted by other known predictors like age, histology, and stage at diagnosis.
In Manizales, approximately 8 out of 10 women diagnosed with BC are alive 5 years after diagnosis. This rate is lower than that reported in developed countries in Western Europe (France, Germany, Spain) and North America (USA and Canada), but comparable to Asian (Kuwait, Qatar) and Eastern European (Bulgaria, Croatia, Slovakia, Lithuania, Poland) countries. Within the Latin American context, BC survival in Manizales aligns with the rates reported in Brazil, Chile, and Cuba, but is lower than those reported in Argentina, Costa Rica, Perú, and Puerto Rico. 17 In the current study, survival closely resembles that reported in a previous study in Manizales that analyzed survival in women diagnosed between 2003 and 2007. 6
The distribution of cases based on the stage at diagnosis mirrors that reported in Chile by Ceballos-Morales et al, with around 70% of cases diagnosed in stages I and II. 18 This represents an improvement compared to the earlier cohort of BC patients in Manizales. 6 However, the analysis of staging distribution according to HIR and SL in this study reveals that the health system’s performance in achieving early diagnosis varies based on the HIR and SL of the patients, with a gap that affects disproportionately to women belonging to the subsidized HIR and those with low SL, representing economically disadvantaged and vulnerable women.
These findings align with those observed in North Carolina (USA) by Markey et al, who highlighted associations between advanced stage diagnoses and factors such as lacking health insurance or having subsidized insurance, being of non-Hispanic black race, and residing in rural areas or areas with high socioeconomic deprivation. 19 Similarly, a study conducted in the Colombian Coffee Region suggests that the lack of timely breast cancer diagnosis (defined as delays in confirming the diagnosis due to altered mammography reports) is associated with factors such as HIR, rural residence and low SL. 20 Studies in developed countries have shown that late diagnosis explains up to a third of the inequities in BC survival. 21 It is plausible to consider that this portion of survival inequities explained by staging may be even greater in countries such as Colombia.
Previous studies in Colombia22-24 and the USA25,26 have identified the HIR as a determinant of BC survival, which aligns with the significant differences in survival by HIR observed in our research. The probability of dying from BC within 5 years after diagnosis is 94% higher for women in the subsidized regime compared to those in the contributory regime. This association persisted after adjusting for covariates, indicating that the HIR effect on survival is independent of SL, RA, age and histological type. There is also a positive interaction (synergistic effect modification) between HIR and the stage at diagnosis regarding BC survival. In other words, this result indicates that the health system response varies based on the HIR, and that barriers and delays exist in the care of women in the subsidized HIR, affecting both access to diagnosis (higher frequency of late diagnosis) and timely treatment and adherence (lower survival). In the previous study in Manizales, a 29% higher hazard of dying within 5 years was observed for women in the subsidized HIR compared to those in the contributory HIR, although statistical significance was not reached, likely due to a smaller number of cases analyzed. 6 These results suggest that there has been no progress in reducing health insurance-mediated inequities between the period 2003-2007 and the period 2008-2015; instead, the gap seems to have widened.
Similar to our findings, several studies have evidenced lower BC survival in women of low SL compared to those of higher socioeconomic level,27,28 even independent of BC stage at diagnosis. 29 We observed 93% and 144% higher hazard in women with middle and low SL, respectively, compared to those with high SL. This gap is wider in this 2008-2015 cohort compared to a 35% difference in hazard based on SL in the previous study. 6 The literature suggests that individuals with a better socioeconomic position generally benefit more from cancer prevention activities and have better treatment of detection and diagnosis processes due to improved access to health services, increased health literacy, and fewer financial barriers to health care. 30
Our study did not find differences in survival based on RA, which somehow is in line with reports from other countries: in Germany, slight differences in survival favored women in urban areas, 31 while in United States differences in survival were better explained by the interaction between rurality and poverty. 32 Our results may partly be due to the low number of cases from rural areas, reflecting the urban-centric population distribution in Manizales (94% residing in urban areas). Additionally, it is important to consider that conditions for women in the rural area of Manizales may differ from those in other municipalities of Caldas and Colombia due to geographic, economic, educational or ethnic barriers that could be more significant.
This research extends a survival analysis previously conducted in the 2003-2007 cohort, providing updated and consolidated evidence on survival gaps mediated by certain social determinants of health. It generates robust data on the overall performance of the health system, given the population approach of the study. These findings can be utilized by individuals and civil society organizations to highlight the unfair, unnecessary, avoidable and unethical differences within the Colombian health system concerning BC. Moreover, they contribute to measuring the goals of the Decennial Plan for Cancer Control in Colombia (strategic lines 2, 3, and 5) and the Sustainable Development Goals (specifically, goals 3, 5, and 10). The methodology used is comparable to that of the previous study and other studies published in the international literature.
As limitations of this study, some prognostic factors, such as biomarkers (estrogen and progesterone receptors, HER-2), genetic profile, comorbidities, education level, among others, were not available and therefore not included These factors could have modified the effect of the studied variables, limiting the scope of this study. Detailed information about treatment (e.g., beginning, adherence, scheme, delays), which was also unavailable, could have provided a better understanding of the role of socioeconomic determinants in BC survival inequities. Our study lacked access to data on patients' screening history, which would have allowed us to analyze the potential impact of screening programs, as well as the individual participation of women in screening programs. It is important to take into account that not all cases diagnosed at late stages can be attributed solely to a lack of access, as there are also individual factors related (e.g., lack of awareness).
On the other hand, as strengths of this study, it can be highlighted the optimal quality of the MCR indicators for BC, improvements data completeness for ‘stage’ compared with the previous study in Manizales, a negligible percentage of losses to follow-up, and verification of the cause of death for each case.
Conclusion
BC survival in women in Manizales is 78% 5 years after diagnosis. Advanced-stage diagnosis was more frequent in women belonging to the subsidized HIR and those with low SL. This study suggests that barriers and delays exist in the care of women in the subsidized HIR and from low SL, both for access to diagnosis (greater frequency of late diagnosis) and timely treatment and adherence (lower survival). The research provides evidence on survival gaps mediated by certain social determinants of health and generates data on the overall performance of the Colombian health system. To mobilize all stakeholders within the health system (patients, healthcare personnel, healthcare service providers, insurance companies, government, among others) is essential to overcome the challenges observed regarding BC.
Footnotes
Authors Note
Office of Vital Statistics, Dirección Territorial de Salud de Caldas.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is part of the project , co-financed by the Colombian Ministry of Science, Technology and Innovation (Grant number 111584267659) and by the participating institutions: Universidad de Antioquia, Universidad del Norte, Universidad de Caldas, Universidad de Nariño, Fundación Cardiovascular de Colombia, Queen Mary University of London and the International Agency for Research on Cancer, Centre International de Recherche sur le Cancer.