
Abstract
Anxiety, a condition which is commonly found in patients with cancer, has negative impacts on their quality of life and treatment outcome. This study aimed to determine the level of anxiety in patients with cancer and explore sociodemographic, disease-related, and hospital-related factors associated with anxiety in those patients. A cross-sectional study was conducted on 510 inpatients with cancer at Thanh Hoa Oncology Hospital, Vietnam. Data were collected from self-administered questionnaire forms on hospital depression anxiety-A, interviews with patients, and patient medical records. The univariate and multivariate linear regression analyses were performed using STATA ver. 14.0. Our finding that the patients’ mean anxiety score (standard deviation) was 7.22 (3.8); 27.6% of the patients had an anxiety score between 8 and 10 points, and 15.5% had an anxiety score of ≥11 points. In the multivariate model, in more advanced stages of cancer, and patients with metastasis were more likely to have higher levels of anxiety than those who presented no sign of metastasis. The longer the patients had cancer, the less anxious they became. Lower levels of anxiety were observed in patients who stated that hospital facilities were adequate or had trust in health workers. Patients with cancer need to be provided with psychological support in the early stage of cancer detection and when metastases form. A strong patient–health-care provider relationship after diagnosis may help reduce distress among patients with cancer with higher levels of medical mistrust.
Introduction
Cancer is one of the leading causes of death in the world, killing people at an alarming rate. Global burden of disease in 2013 1 reported 14.9 million incident cancer cases, 8.2 million cancer deaths, and 196.3 million DALYs due to cancer. According to 2014 Annual Health Review of the Vietnamese Ministry of Health, 2 there were estimated 125 000 new cases and over 80 000 deaths from cancer each year. Moreover, in Vietnam, the incidence of cancer has increased rapidly to rank in the top 5 causes of death, 3 and only at the later stages of cancer (III or IV) did more than 70% of patients have a medical examination at health facilities. 2,4
Anxiety and depression may have negative effects on patients with cancer. For example, they may lead to functional disorders, longer hospital stay, and less effective treatment outcome. 5 Thus, it is of great importance to do research on those illnesses. 6 -9 Besides physical pain, emotional distress, comorbidities, anxiety, and stress are also important factors affecting their quality of life. 10 -13
Symptoms of anxiety are identified in patients with cancer at a frequency of 30% to 35% in Vietnam. 14,15 Several factors have been found to be associated with anxiety in patients with cancer, including sociodemographics, functional status, and social support. 14 -17 Community characteristics and many other factors affecting the anxiety of patients need to be studied thoroughly to provide evidence-based care for patients with cancer, thereby improving their quality of life. 7,17,18 Identification of risk factors for anxiety in patients with cancer can improve their health outcomes.
In the context of hospital, overload is particularly serious at central hospitals of Vietnam 19 and anxiety of patients is affected by hospital-related factors. 20,21 A number of studies on these factors were conducted in central hospitals in Vietnam, 14,15 but none has been carried out in provincial hospitals, including those in Thanh Hoa province. The study aimed to determine the level of anxiety in patients with cancer and explore sociodemographic, disease-related, and hospital-related factors associated with anxiety in patients with cancer.
Methods
Study Design
This cross-sectional study was carried out in Thanh Hoa Oncology Hospital from March 2018 to September 2018.
Study Participants
The study team screened all patients with cancer for eligibility. To be included in the study, a patient must be (1) at least 18 years old and (2) able to read, understand, and complete a consent form in the Vietnamese language. Those who had high mortality rates were excluded from the study.
Sampling
The sample size of this cross-sectional study was calculated using the following formula
22
Convenience sampling was used to select inpatients with cancer at Thanh Hoa hospital that met the inclusion criteria. In total, 510 inpatients with different types of cancer, including 353 males and 157 females, were selected.
Data Sources
Data were collected from 2 sources: (1) Patient medical records, from which demographic and health data were extracted; (2) self-administered anxiety questionnaire forms; and (3) face-to-face interviews, which helped verify demographic data of patients and assess the hospital environment.
Measurements
Primary study outcome
Anxiety of patients was the primary outcome of this study. Zigmond and Snaith 24 developed the Hospital Anxiety and Depression Scale (HADS) as a tool to measure anxiety and depressive symptoms. It has been widely used in hospitals to screen for psychological disorders. 7,9,23,25 -28 This tool consists of 14 questions divided equally into the anxiety subscale: Anxiety scale from the Hospital Anxiety and Depression Scale (HADS-A) and the depression subscale (HADS-D). A 4-point Likert scale was used for all questionnaire items, ranging from “0” (low/negative perception) to “3” (high/positive perception). Therefore, domain scores are scaled in a positive direction where higher scores denote higher anxiety. A domain score of 0 to 7 indicates “normal,” 8 to 10 “borderline,” and 11 or greater “abnormal/disorder.” 24,28,29 The validity of HADS was confirmed 28,30 and the scale proved to be able to detect cases of mental diseases with sufficient accuracy. 27,29 The HADS has been translated into Vietnamese 31 and used with various populations. 14,15,31,32 The HADS-A subscale was internally reliable (α-anxiety = .904) in our study.
Study interviewers were 4 members of the Thanh Hoa hospital’s health staff. They were all trained to obtain informed consent, conduct interviews, and oversee the completion of the self-administered HADS-A questionnaire forms.
Independent variables
We interviewed the patients about factors that might be associated with their anxiety, including demographic information (eg, age, gender, occupation, education level, and marital status), socioeconomic status of their families, ability to pay treatment fees, health insurance status, and the environment of the hospital.
Demographic factors: Education level was categorized into 2 groups, namely (1) high school education or lower, and (2) above high school education. Marital status was dichotomized to represent married and living with spouse versus others (separated/ divorced/ widowed, single).
Socioeconomic parameters: Economic status was categorized into 3 groups: (1) poor, (2) near poor, and (3) nonpoor. We also extracted the health insurance status of patients (yes or no). Occupation was grouped into farmer and non-farmer.
Clinical parameters were assessed by the following: length of the time from diagnosis to the time of the interview, tumor entity, cancer stage, and confirmed metastases. We extracted all clinical parameters from the health medical records of the patients.
Treatment parameters: Treatment procedures have been extracted from health medical records, included 3 nominal variables: chemotherapy (yes/no), radiation (yes/ no), and surgery (yes/no). The ability to pay treatment fees was categorized into 3 groups: (1) could afford to pay the bills, (2) had to pay the bills with loans, and (3) unable to pay any amount of the bills immediately. Patient’s perceived treatment outcome was categorized into 3 groups: (1) better, (2) unchanged, and (3) worse.
Hospital environment factors: Patient’s perception about hospital environment included 3 nominal variables (yes/no): (1) adequate hospital facilities, (2) health workers’ positive behaviors, and (3) patients’ trust in health workers.
Statistical Analysis
Data were processed and analyzed using STATA ver. 14.0 (Stata Corp., College Station, Texas). Demographic and clinical characteristics of patients were summarized in total, and differences between the 2 gender groups were examined using t tests for normally distributed data and Wilcoxon rank-sum (Mann–Whitney) test for non-normally distributed data. Besides, χ2 statistic was used to examine the relationships between categorical variables.
Reliability of HADS-A was evaluated by internal consistency (Cronbach α). If the α value is .7 or higher, this suggests that the test is reliable and the scale could be used properly. 33
The mean anxiety score (ranging from 0 to 3 points on a 4-point Likert scale) was calculated for each patient. A total anxiety score was constructed by summing the scores of all questionnaire items; it had a maximum value of 21 points. Anxiety was treated as a continuous variable with normal distribution in inferential statistics.
To separately determine the associations of certain factors with anxiety, univariate linear regression models were performed. Meanwhile, multivariate linear regression models only included variables significantly less than .2 α level in the univariate model and were additionally adjusted for age.
Ethical Consideration
Patients were provided written informed consent forms and were required to complete self-administered questionnaire forms. Clinical information was extracted from the medical records of patients who agreed to participate in the study.
The protocol was approved by hospital administrators and the Scientific and Ethical Committee of Thang Long University (QĐ 235 \012018\ SĐH–ĐHTL). Written informed consent forms were obtained from all participants. The patients’ personal information would be kept confidential.
Findings
In our study, we recruited 510 patients with cancer from Thanh Hoa General Hospital, including 353 males and 157 females. At the time of the interview, they were confirmed to have cancer for a median (interquartile range) period of 5 (10) years.
Overall, the mean (standard deviation [SD]) age of the patient was 58.98 (10.5) years old, and female patients were significantly younger than male patients. Besides, 91.4% of the patients had a high-school education or below, and about 90.6% of them were married or lived with their spouses (Table 1). Nearly 77% of the patients reported living above the poverty level, and 98.6% participated in health insurance. No significant differences in terms of education, health insurance status, and occupation were observed between males and females.
Characteristics of 510 Cancer Patients in Thanh Hoa General Hospital, Thanh Hoa Province, 2018.
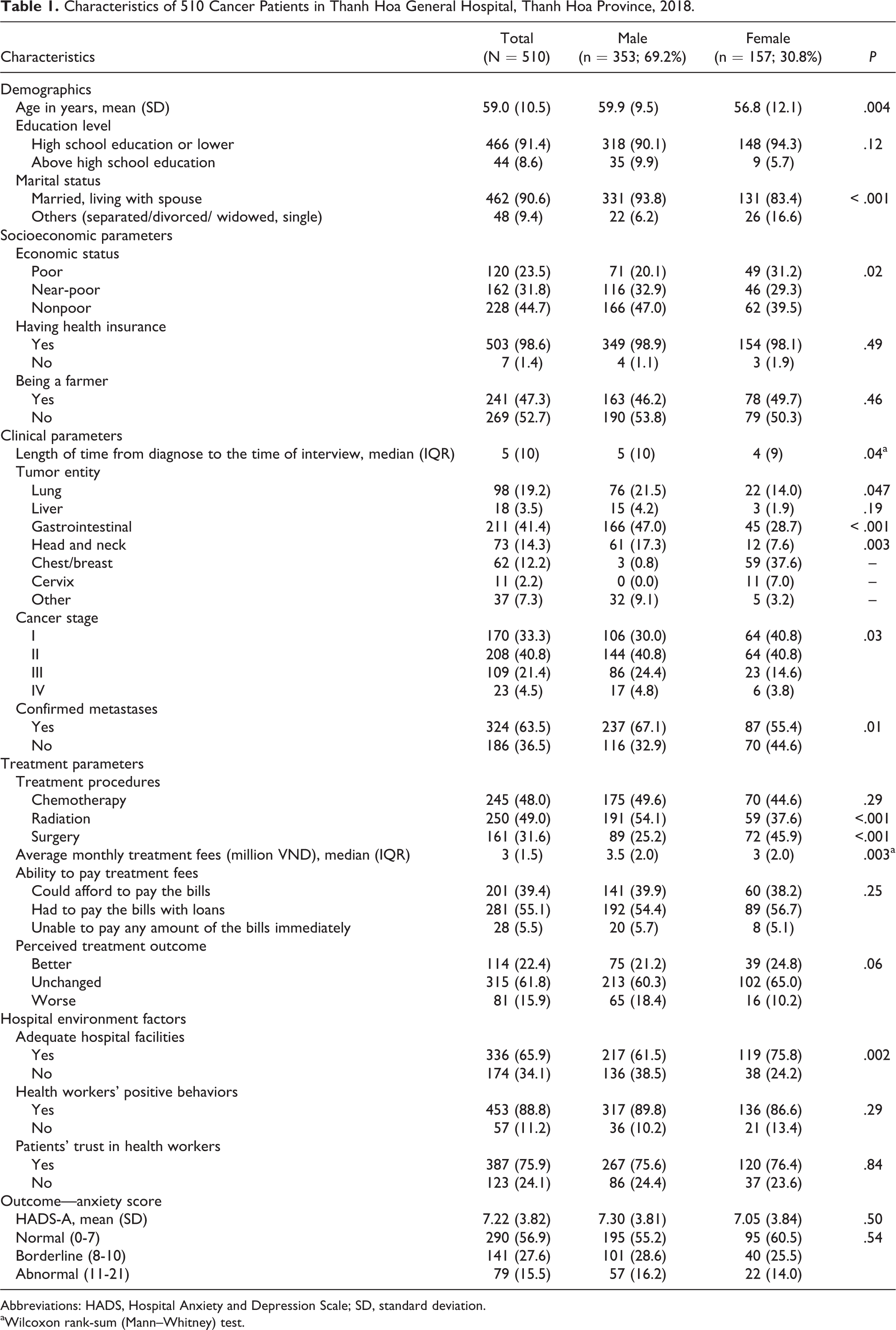
Abbreviations: HADS, Hospital Anxiety and Depression Scale; SD, standard deviation.
aWilcoxon rank-sum (Mann–Whitney) test.
About 41% (n = 211) of the patients had gastrointestinal cancer, compared to 19.2% (n = 98) having lung cancer (Table 1). Regarding cancer stages, 40.8% of the patients (n = 208) were in stage II, 21.4% (n = 109) in stage III, and 4.5% (n = 23) in stage IV. At the time of interview, more male patients than their female counterparts were diagnosed with metastases (67.1% vs 55.4%); this difference was statistically significant. There was no significant difference between the 2 gender groups in terms of the proportion of patients who reported experiencing health workers’ positive behaviors or having trust in them.
Patient’s Anxiety Scores
In this study, patients had a mean (SD) anxiety score of 7.22 (3.8) of a maximum score of 21 points (Table 1), and the 2 gender groups saw no difference in this anxiety score. In addition, 43% of the patients received a score indicating either the borderline or abnormal level in the anxiety subscale.
Factors Associated With Anxiety
Univariate analysis
We performed a linear regression analysis to examine potential risk factors individually (Table 2). Education was statistically significantly associated with the perceived quality of life. Patients with more than 12 years of schooling were more likely to report a higher level of anxiety. Their mean score of anxiety was 1.35 points higher than those who only completed high school education or any lower level of education.
Univariate and Multivariate Linear Regression Analysis of Characteristics Associated With Anxiety Score of 510 Patients With Cancer at Thanh Hoa General Hospital, Thanh Hoa Province, in 2018.

aA 1-unit increase in covariate corresponds to a β increase in the total anxiety score (if the coefficient >0) or a β decrease in total anxiety score (if the coefficient <0)
bThe factors have been adjusted for in multivariate linear regression model.
The anxiety score reduced slightly over the length of time from the diagnosis of cancer to the time of the interview; however, this reduction was statistically significant. It decreased by an average of 0.05 points for each year added to the duration of diagnosis.
Regarding hospital environmental factors, patients reporting that hospital facilities were adequate scored 2.3 points lower than the others. Patients witnessing health workers’ positive behaviors scored 1.33 points lower than the others. In addition, the anxiety score of patients having trust in health workers was 2.0 points lower than that of those without trust.
Variables, such as age, marital status, gender, economic status, occupation, average monthly treatment fees, or ability to pay treatment fees, had no association with anxiety (Table 2).
Multivariate analysis
All covariates significant at the .05 α level in the univariate model were included in the multivariable model (Table 2). The latter model was additionally adjusted for age.
In the multivariable analysis with all other factors held constant, the anxiety score of surgical patients was 1.144 points higher than that of nonsurgical ones. In addition, cancer stage, confirmed metastases, perceived treatment outcome after cancer treatment, and the length of time between cancer diagnosis and the time of the interview had independent effects on the level of anxiety. Patients with later stage cancer had a higher level of perceived anxiety. When adjusting for individual factors, the anxiety scores of stage II, stage III, and stage IV groups were 1.85 points, 1.98 points, and 2.69 points, respectively, higher than that of the stage I group. With every 1-year increase in the duration of diagnosis, the anxiety score decreased by 0.07 (Table 2). The anxiety score of patients with confirmed metastases was 0.76 points higher than those with non-confirmed metastases. The anxiety scores of patients reporting no change in their treatment outcome and those stating that their health status became worse after treatment were significantly higher than that of those reporting their health status improved after treatment.
In the multivariate linear regression model, we found 2 hospital environment variables strongly associated with the anxiety score. More precisely, patients reporting that hospital facilities were adequate scored 1.87 points lower than the others. In addition, when all other factors were held constant, the anxiety score of patients having trust in health workers was 1.08 points lower than that of those without trust.
Variables, such as age, education level, marital status, occupation, average monthly treatment fees, or patients witnessing health workers’ positive behaviors, had no association with anxiety in the multivariate linear regression model.
Discussions
This study aimed to fulfill 2 objectives: (1) examining the level of anxiety among patients with cancer and (2) identifying factors associated with anxiety. The results show that the mean anxiety score of patients was 7.22; about 15.5% had an anxiety score of ≥11 points. Patients with more advanced stages of cancer and patients with metastasis were more likely to have higher levels of anxiety than those who presented no sign of metastasis. The longer the patients had cancer, the less anxious they became. Lower levels of anxiety were observed in patients who stated that hospital facilities were adequate or had experiences of positive health worker attitude.
The mean level of anxiety symptoms in our study was significantly higher than those reported by prior studies. 17,26 Patients with an anxiety score of >7 accounted for 43%. This figure indicates that anxiety in patients with cancer should be paid more attention. This result is similar to previous findings in Vietnam, China, and some other countries which ranged from 20% to 60%, depending on what parameters were used. 7,9,16,25,26,34 -36 It can be seen that anxiety is relatively prevalent in patients with cancer, as they have to adapt to the unpredictable and uncertain trajectory of the disease, which may affect their family life, social life, and work life.
In our study, several disease-related factors were significantly associated with anxiety; however, we found no association of sociodemographic factors, such as age, gender, education level, with anxiety in the multivariate regression model. This finding is in agreement with those of the previous studies. 37
Our study results show that the longer the length of time from the diagnosis to the time of the interview, the lower the level of anxiety of patients with cancer. Some researchers 35,38 have noted that fears commonly occur in patients with cancer, especially when the condition is initially diagnosed, when the decision on treatment is made, or when they feel apprehensive about the progression or recurrence of cancer. Patients with cancer with longer duration of diagnosis had a tendency to accept the disease, feel no fears of death, or feel not as anxious as they were when initially diagnosed with cancer. Hinz et al 25 showed that patients were more anxious at the start of their treatment but later became higher on psychological stability over time. The mean anxiety scores of patients at discharge or 1 year after discharge was similar to those of the general population but lower than those of cardiac patients. 7,25 As our study had a relatively large sample size (510 patients), a small change in anxiety score (0.07) after 1 year of diagnosis of cancer is statistically significant but not practically significant. The interpretation of results should be given careful consideration.
It should be noted that these anxiety scores may vary according to the stage of cancer. Our study confirms the findings that a more advanced cancer stage was associated with anxiety. 26,37,39 In later stages of cancer, patients are weaker and present more symptoms and metastases. Furthermore, they may have difficulty consuming foods and drinks, feel pain, and experience sleep deprivation. As a result, they tend to be more worried about their health, lose hope of having effective treatment, have frequent thoughts of death, and have worrying thoughts of their family members. Patients undergoing surgery for cancer were more likely to be anxious than those with nonsurgical treatment, as surgical cancer treatment causes pain to patients, and prolonged recovery. Besides, the treatment outcome/response has a profound impact on the anxiety of patients. Particularly, if the treatment proved ineffective, that is, the patient condition remained unchanged or became worse, their level of anxiety increased accordingly. This is seen not only in patients with cancer but in those with other medical conditions.
According to a study conducted by Sheppard et al 21 , the lower levels of anxiety were seen among patients who had a high opinion of health workers’ professional competencies and interpersonal skills. In other words, patients with higher levels of mistrust in health care tended to have higher levels of anxiety, which is similar to our result. A possible explanation is that patients with no trust in health workers, service quality, or hospital facilities, felt more anxious, as their treatment of a fatal disease like cancer had to depend on the health-care provider. Positive communication with patients and the patient-centered care approach can improve the relationship/interaction between patients and health workers, thereby reducing the level of mistrust in health workers and service quality, and ultimately relieving the anxiety of patients. Annunziata et al 20 suggested the importance of sensibly disclosing diagnostic and prognostic information to patients and their families. Also according to this author, patient satisfaction with information giving is associated with their better quality of life and decreased anxiety among patients with cancer.
Limitations: In this study, we excluded advanced patients with cancer at high risk of death. Therefore, the prevalence of patients with anxiety in this study was lower than the actual figure. Besides, due to the nature of this cross-sectional study, it was not possible for us to identify the changes in any particular anxiety of patients at different points of time. On the other hand, the self-report bias is inevitable when a self-administered questionnaire is used. Finally, our results could not generalize to a large population because we just selected patients conveniently in one single provincial hospital.
In conclusion, our study results indicate that anxiety is a major problem among patients with cancer. Thus, patients with cancer need to be screened for anxiety in particular and mental health in general, especially in the early detection, so that health workers then can provide them with proper psychological support. Clinicians should consider and carefully monitor the psychological conditions of patients with cancer before and during surgery in order to optimize therapeutic effects and alleviate anxiety of the patients. A strong patient–health-care provider relationship after diagnosis may help reduce distress among patients with cancer with higher levels of medical mistrust.
Supplemental Material
Supplemental Material, multivariate_model_stata_result - Anxiety Among Inpatients With Cancer: Findings From a Hospital-Based Cross-Sectional Study in Vietnam
Supplemental Material, multivariate_model_stata_result for Anxiety Among Inpatients With Cancer: Findings From a Hospital-Based Cross-Sectional Study in Vietnam by Dung Viet Truong, Quyen Thi Tu Bui, Do Tri Nguyen and Jaleesa Moore in Cancer Control
Footnotes
Authors’ Note
All authors designed and conceptualized the paper. DVT and QTB analyzed the data; DVT, QTB, and DTN interpreted the results, prepared and reviewed the manuscript. All authors contributed to the critical revision of the manuscript for important intellectual contents, read, and approved the final manuscript.
Acknowledgments
The authors express their thanks to The Director, doctors, and nurses at Thanh Hoa Oncology Hospital for supporting them in data collection. The authors are also indebted to Thang Long University for financing support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Thang Long University, Ha Noi supported for data collection.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.