
Abstract
Cancer causes the highest economic loss of all of the leading 15 causes of death worldwide. The economic loss includes the loss of income and the expenses associated with health care costs. The Low awareness of the community toward cancer, the inadequacy of professionals and service providers, and the high budget consuming nature of the treatments are creating a great burden on the cancer patients. The objective of this study was to calculate patient side cancer treatment cost and to assess the contributing factors, among the cancer patients who were treated at Hawassa University Comprehensive Specialized Hospital. The health facility based cross-sectional study design was employed using a consecutive sampling technique. Questionnaires was used to collect primary data; while chart was used to collect the secondary data. Indirect costs incurred on these patients due to off job days were checked. Descriptive and inferential statistics were applied to illustrate the data. On average, $209.99 was spent on treatment by each cancer patients. Of these, medication cost is the highest ($20.77, IQR = 0.53-112.56) from the direct medical costs, and transportation cost is the highest ($58.33, IQR = 22.0-131.67) from the indirect medical costs. Inpatients paid $245.16 (IQR = 147.64-439.20); while outpatients paid $147.37 (IQR = 81.42-240.50). The patients lose about 55.99% of their average annual income. Outpatients pay $0, 92 less than in patients (P = 0.00, CI -0.72-0.34), and the cost increases by $0.2 for the patients who came from Oromia. The cost of transportation and medication were the one which were significantly affecting the burden; but the total cost of treatment was lesser when compared to similar studies done in different areas. The cost balances toward the patients who came from the Oromiya region. Treatment service has to be extended to West Arsi Zone to minimize the cost of transportation and awareness about cancer is needed in the first place and due attention has to be given to thyroid cancer. Furthermore, facility side study should be done to see the complete picture of the burden.
Introduction
Cancer is the highest economic loss of all the leading 15 causes of death worldwide. The economic loss is both in terms of income and expense for treatment. 1 Studies estimating the global cost of cancer as the main cause of great loss of life years representing a huge loss of resources in medical, non–medical and human terms. 2 As cancer treatment costs are increasing, insurance’s cost sharing is balancing toward the patients. 3 For example, the estimated health care cost of cancer has increased from $124 billion in 2010 to $157 in 2020 in US. 4 The economic impact of cancer is not limited to the increasing direct cost of treatments; rather it can extend to the greater indirect costs including loss of productivity and impaired quality of life. 5 The cost estimation was highly dependent on a number factors like, the type of cancer treatment patient needs, how long patient needs to be treated, where a patient will be treated, patient health insurance coverage, whether patient has supplemental insurance or medical costs and hidden costs. 2
The increasing population in Ethiopia is not limited to 84 million; the growth rate can take it to the ninth most populated country in the world by 2030. The incidence of cancer goes parallel to these population growth. 6 The Low awareness of the community towards cancer 1 , the inadequacy of professionals and service providers, 7 and the high budget consuming nature of the treatments 1 are creating a great burden on the cancer patients; adding up on the high prevalence and complicated nature of the disease. 2 From total national mortality in Ethiopia, 5.8% is by cancer. There is no data about cancer for the general population of Ethiopia, other than for Addis Ababa population. But the annual cancer incidence in estimated to be around 60,960 and death by cancer to be more than 44, 000. 8
Limited information is found regarding the cost for cancer treatment in Ethiopia. It is important to have a knowledge of the economic impact of cancer to develop and implement health interventions. This study will help and provide a guideline to estimate the economic burden or costs of cancer on the patient side.
Methodology
Description of Study Area
Hawassa city is the capital of the Southern Nations, Nationalities and Peoples Region (SNNPR) of Ethiopia. The city administration catchment area has 6 health facilities, one general hospital, and one referral hospital. The study area was Hawassa University Comprehensive Specialized Hospital (HUCSH), which was found in Hawassa City Administration, SNNPR, Ethiopia. The Hospital was established in 2006. It is the only teaching comprehensive specialized referral hospital in the region; and provides service for people living in the town, in the region and nearby areas.
Study Design
The health facility-based cross-sectional study design was used to estimate patient side economic cost of cancer treatments on cancer patients who are getting treatment at Hawassa University Comprehensive Specialized Hospital in 2018/19.
Source Population
All patients treated at Hawassa University Comprehensive Specialized Hospital.
Study Population
All patients on cancer treatment at the Oncology Department of Hawassa University Comprehensive Specialized Hospital in the year 2018/19.
Inclusion Criteria
Any cancer patients who are on treatment, alive, having recorded with full information, who is available at the time of the study, willing and capable to respond to the interview at the time of the study.
Guardians of children who can fulfill the above inclusion criteria and can give adequate information on behalf of the cancer patients.
Companions who can fulfill the first inclusion criteria and who can give adequate information on behalf of the cancer patients.
Exclusion Criteria
Referred cases- those who are transferred to other health facilities and who cannot be accessed for an interview during the data collection period.
Patient with Incomplete files due to mortality, dropouts.
Patients not capable of responding and with no any companion.
Study Variables and Measurements
Dependent variable
Direct cost on the patient side and their companion. This is the cost incurred on the patients while they were accessing treatments. It is categorized into two: the direct medical costs and indirect medical costs. The direct medical costs include payments for medicine, laboratory services, physiotherapy and surgery, while the indirect medical costs are payments for accommodation, food and transportation. These are collected from the patients record and using questionnaires.
Indirect cost on patients and their companion. This is the income loss due to the time spent being on treatment at the hospital. It is estimated by the number of days the patients stayed in the hospital and the average daily per-capita income of the less developed country.
Sample Size and Sampling Techniques
Convenience sampling technique was used to identify and interview patients who were coming to the oncology center every day during the study period. The sample size was determined by the study period which took place from December-May, 2019. Hence, a total of 423 patients were interviewed during the study period.
Data Collection
Quantitative primary and secondary data were used to assess cancer patients who are accessing services at HUCSH during the study period and their respective records. A semi-structured, mixed open and close-ended questionnaire was used to collect the socio-demographic data/no alternatives. Chart is used to collect secondary data about the treatments provided to calculate direct and indirect costs.
Records of each cancer patient, who were fulfilling the inclusion criteria, was used. The patient contacted were outpatient as well as inpatients. These data were used to estimate the cost of each service. Finally, all the data collected was transferred to the chart for compiling each patient’s record. This complete excel sheet was transferred into the STATA v.14 software.
Data Quality Control
Data collection was accomplished using BSc nurses who were in the oncology departments and two assistants serving the patients’ records. The training was provided to these data collectors and was supervised by the investigators. Pre-test of questionnaires and data collection charts was conducted to check the quality and reliability of the questionnaire. Five percent of the sample size was used to check the pre-test at Yanet Specialized clinic. Modification of the data collection tools and translation of the questionnaires to the local language was done. Completeness of records was checked every day by the investigator.
Data Analysis
All the compiled data were recorded in the Excel sheet, in terms of socio-demographic, direct and indirect cost of cancer treated patients. Each treatment services was recorded as a ‘direct medical cost,’ in terms of laboratory services provided, medicines administered, chemotherapy provided, surgery and radiotherapy provided. Other facilities the patient used as an ‘indirect medical cost’ from the first day up to the time of data collection. In addition, the number of days elapsed on treatment was used to calculate the ‘indirect cost’ other than indirect medical cost. The costs are estimated based on the existing price in the hospital. The data were imported to STATA v. 14 and is used for analysis. The variables were described in terms of the total cost for each cancer type, patient type, and the respective socio-demographic characteristics. The illustration was done in tables, charts and graphs. Furthermore, each independent variable was compared among themselves; and their contribution to the total cost was identified using linear regression. The normal distribution of the dependent variable (total cost) was corrected after log transformation. Furthermore; multicollinearity and homoscedasticity were checked. Coefficient and P values are used to indicate the association and hence its significance.
Ethical Consideration
Ethical approval of the research proposal was obtained from the Institutional Review Board (IRB) of Hawassa University, College of Medicine and Health Science. A formal letter was written to HUSCH and Yanet Special Clinic to permit us to undertake the research. Informed verbal consent was obtained from all study subjects before conducting the data collection. For this purpose, a consent form was attached to each questionnaire which explained the purpose of the study, confidentiality, and the respondent’s full right to take part or not to take part in the study.
Results
Socio-Demographic Characteristics
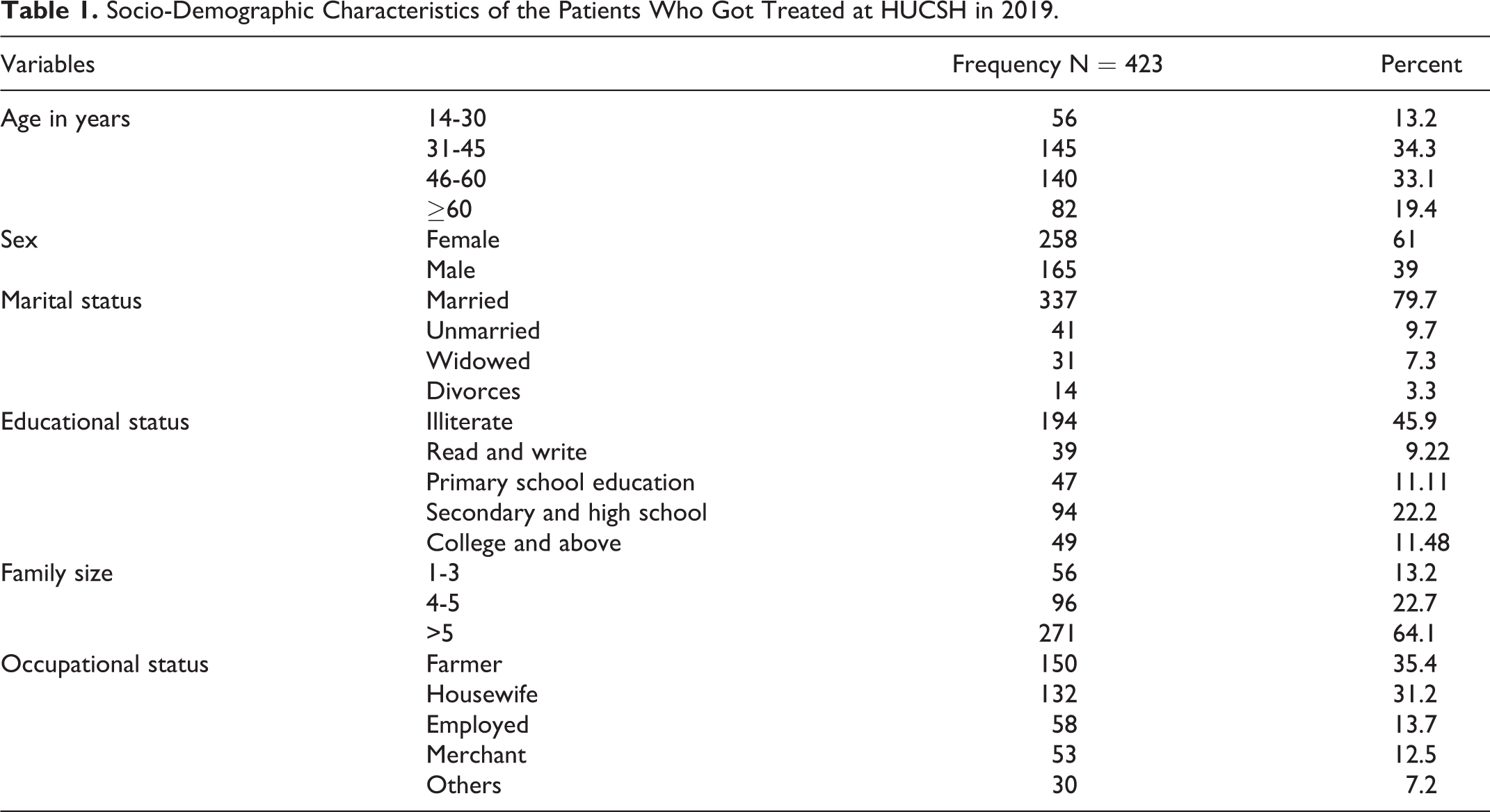
Out of 423 respondents, 330 were inpatient (78.01%) and 93 were outpatients (21.99%). Majority of the respondents were female (n = 258 or 61%). Their mean age was 45 (IQR 15-85) years and the most frequent one was 50 years of age (n = 41 or 9.7%) (Table 1).
Socio-Demographic Characteristics of the Patients Who Got Treated at HUCSH in 2019.
The geographic distribution of most of the patients treated at HUCSH were 249(58.9%) from SNNPR and 171(40.4%) Oromiya regions. Of which 153 (36.17%); followed by West Arsi zone 92 (21.75%) and Bale zone 41 (9.69%) (Figure 1). Accordingly, the median distance from where the patients came was 82Kms (IQR25-171) away from the Hospital.

Map showing the distribution of cancer patients who accessed treatment at HUCSH in 2019.
History of Patients With Cancer
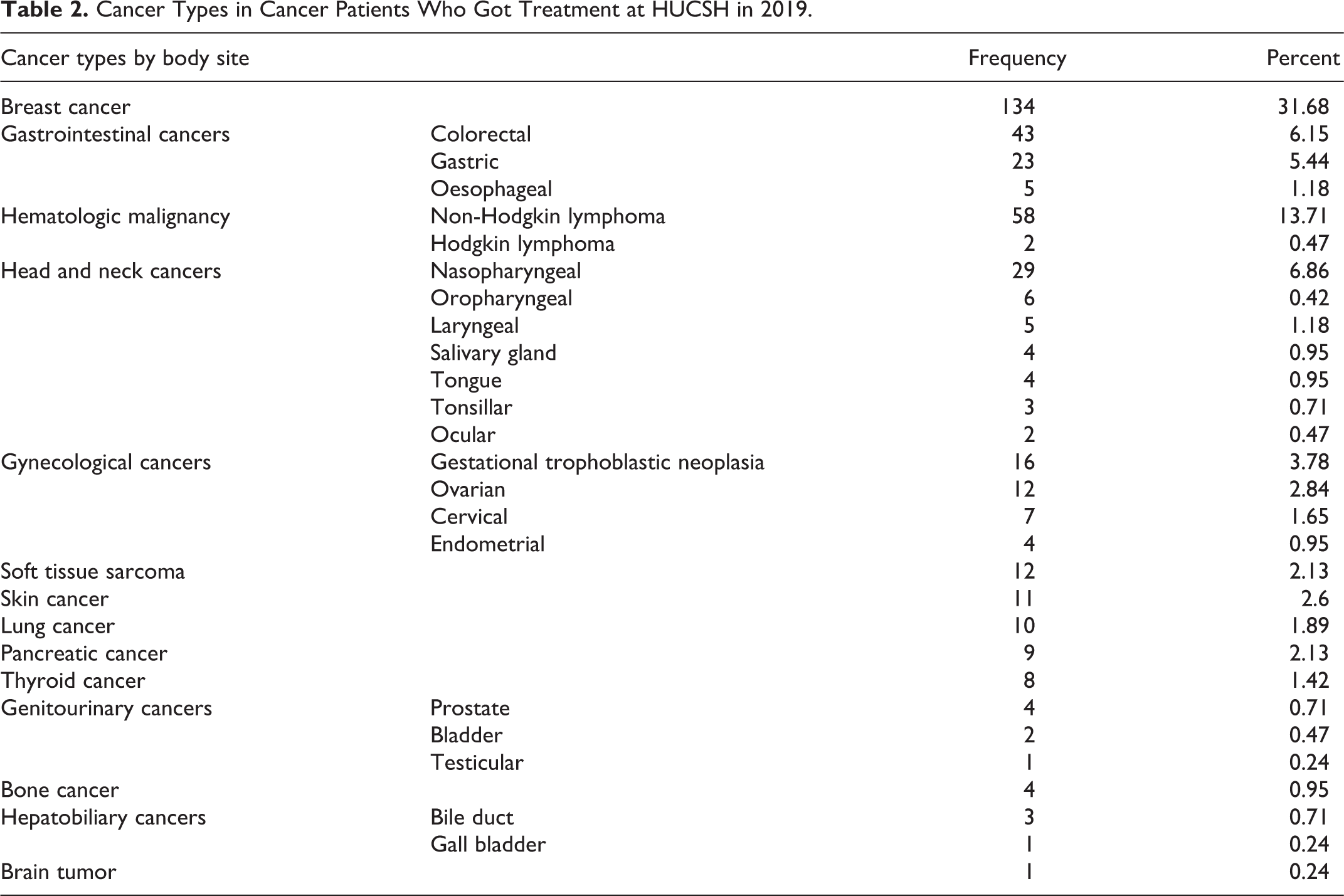
The median duration of the first symptoms to diagnosis was one year (IQR 0.1-15). A total of 35 cancer types were who treated at HUCSH were identified by body site during the study period. The most frequent type of cancer is breast cancer 134 (31.7%); followed by gastrointestinal cancers 71(16.8%) and hematologic malignancy 60(14.2%) (Table 2).
Cancer Types in Cancer Patients Who Got Treatment at HUCSH in 2019.
The Cost Incurred on Cancer Patients
The majority of the costs were covered by patients themselves or by their family members; as every service involved out of pocket cash.
Direct Cost
The median direct medical cost of treatment at the hospital was $76.33 (IQR26.0-177.64). A total of 73.33 (IQR 34.0-150.67) dollars was spent on direct non-medical costs. Generally, an average total cost of $209.83 (IQR 125.22-395.22) was spent by each patient who visited the Hospital for each type of cancer treatment (Table 3). When the components of the total cost are compared, the highest cost was transportation cost and the least was the indirect cost lost while seeking treatments.
Out of Pocket Costs Incurred on the Cancer Patients Accessed Treatment at HUCSH in 2019.a
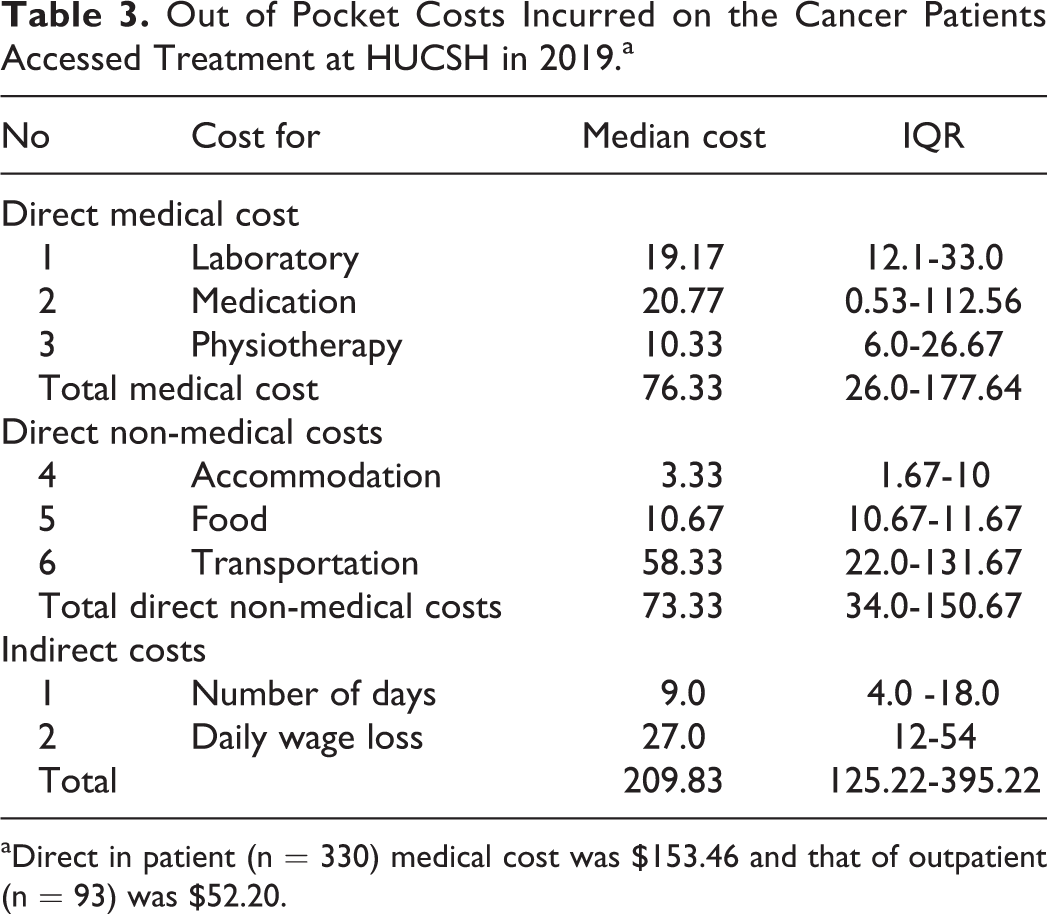
aDirect in patient (n = 330) medical cost was $153.46 and that of outpatient (n = 93) was $52.20.
When the median cost of each type of cancer is concerned separately, medication cost is highest in all types of cancer; followed by laboratory cost (Figure 2).
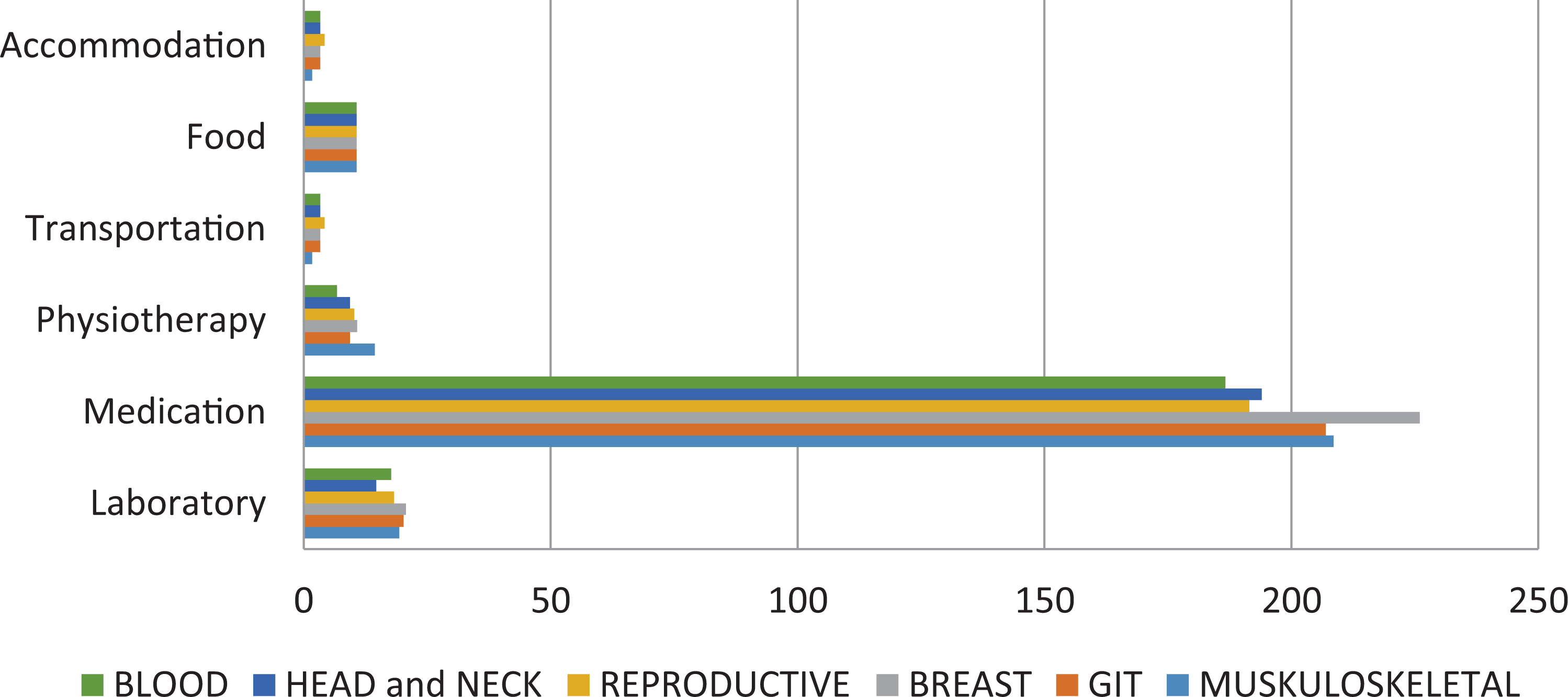
Comparison of cost of cancer treatment for the different types of cancer in 2019.
The total out of pocket money incurred on inpatients was $245.16 (IQR = 147.64-439.20), while for the outpatients $147.37 (IQR = 81.42-240.50).
Indirect Cost
The average number of days the patients were on treatment was 9. In these days, considering their income, they lose about $27.0 (IQR 12-54).
Generally, on average, 55.99% (CI = 50.43-61.57) of their average annual per capita income was lost on the treatment of cancer by each patient.
Cost Predictors
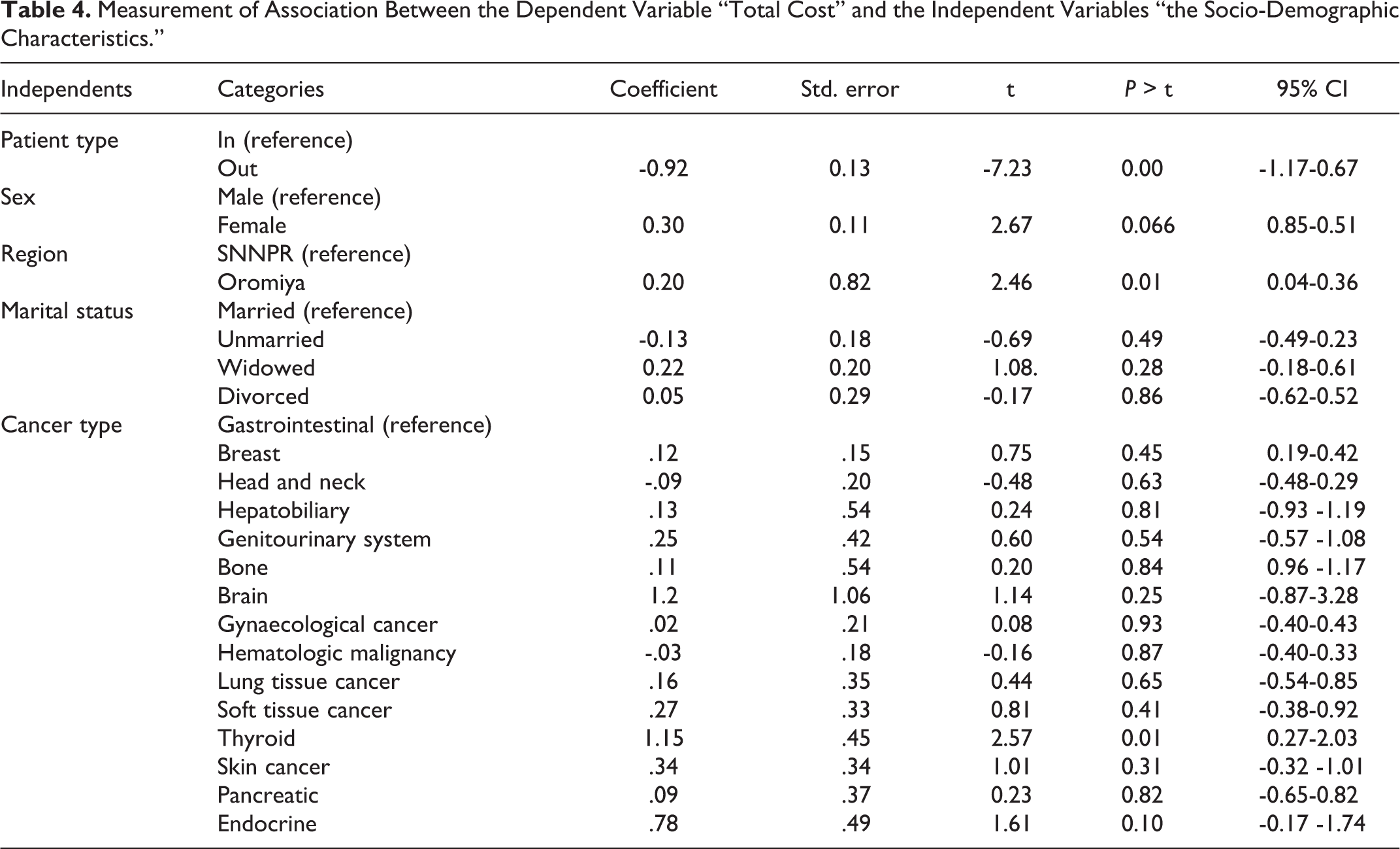
Expenditure for the treatment was not associated with many of the independent variables (Table 4). Outpatients pay $0. 92 less than in patients (P = 0.00, CI -0.72-0.34); furthermore, the cost increases by $0.2 for the patients who came from the Oromiya region. Female patients pay $0.3 more than male patients. Thyroid cancer patients pay $1.15 more as compared to the gastrointestinal cancer patients.
Measurement of Association Between the Dependent Variable “Total Cost” and the Independent Variables “the Socio-Demographic Characteristics.”
Discussions
The average total cost incurred on the patients was lesser than similar cost in other places. The study is the second of its kind in Ethiopia and covers a wide geographic area; since the hospital is the only one providing cancer treatment in that area. Hence; the study provides information about resource allocation in combating cancer. Furthermore, it gives a clue about which part of the population needs due attention. Generally, the amount of money the patients are paying for cancer treatment service and its implication on their average daily income was illustrated well. But this study is limited to out of pocket expenditure only from the patient side. This undermines the amount of money expected to cover the service. Furthermore, the lack of similar study hinder us to show the level of a burden it imposes on the patient income and wealth index. Generally, intangible costs of pain, grief, and suffering were not calculated, cost due to loss of life and lifetime costs due to the disease were not included in this study.
About 35 different types of cancer were identified among the patients treated at HUCSH. The most frequent type of cancer is breast cancer (31.68%); this is less than the national figures (46.72%) of breast cancer incidence. 9 Even though the deviation from the national figure could be due to the small sample size, breast cancer is the one which has to get due attention.
Worldwide, Lung, breast and colorectal cancers take the first 3 ranks in terms of prevalence. 10 -14 The median distance traveled was 82 km away from the hospital; while the patients who got treatment at ABLSH had traveled a median distance of 300 km away from the hospital. 7 The median cost ($58.33) of transportation is far greater than the other direct and indirect costs. It is almost comparative ($55.22) to the study done at All India Institute of Medical Sciences; tertiary public hospitals. 10
The prevalence of cancer is higher (36.17%) in the Sidama zone from the southern region; while the West Arsi zone (21.75) and the Bale zone (9.69%) are the second and third from Oromiya region. The prevalence in the Sidama zone could be from the proximity of the hospital, but the prevalence in the Oromiya zone cannot be assumed due to the proximity of the hospital because there were a variety of administrative areas in the south region that was nearer to the hospital, but few cases were identified. From Esophageal cancer endemic areas in Africa, Arsi Zone is a member for years; and hence it is highly reported as compared to other Ethiopian countries. 15
The direct outpatient medical cost was $52.20; this is lesser when compared to a similar study done at ABLSH ($69.16). 7 Whereas the direct medical cost for the inpatient was $143.56; which was almost half of ($244.42) the cost of cervical cancer patients who got treatment at ABLSH. 7 Of course, the estimation was done only for cervical cancer patient at ABLSH; while this study shows an average cost for every cancer types visited the hospital. Truly speaking, regardless of the shorter average distance traveled compared to ABLSH, transportation cost had contributed more than other direct non-medical costs. The median cost of direct medical treatment was $73.36; this is far less than the median medical cost ($113.23) at All India Institute of Medical Sciences; tertiary public hospitals 10 ; less than the median cost ($1280) of treatment for cervical cancer studied at ABLSH 7 ; and less than the cost ($2011) incurred on cancer patients in Sri Lanka. 16 These studies are compared because the countries are listed in low and middle income countries; otherwise, their life style are quite better than Hawassa. The direct non-medical cost was $73.33; which is somewhat higher than ABLSH cervical cancer patient non-medical cost ($55.17). 7 Even though the difference is not significant, the cost was expected to be lesser for the services in Hawassa when compared to the one in Addis Ababa. The possible reason for this discrepancy could be due to over estimation of the cost by respondents. When each of the cancer types cost is evaluated, the cost of the drug (medication cost) is far more than the other costs. This is also true in the study done at ABLSH for cervical cancer patients. 7 Both study revealed that the price of medicine is higher than other services; not only for cervical cancer treatments just like the other studies, but for all the 35 types of cancers. The indirect cost of treatment accounted for $27 in an average of 9 days missed; this is also much less than the indirect cost incurred ($175) on cervical cancer patients at ABLSH. 2 Services provided in HUCSH is faster when compared to ABLSH; this saved their time and hence their indirect cost. Generally, the total cost of treatment was $209.83; this is far less than the one which was done at ABLSH ($349.9). 7 Even though it was lower when compared to other studies, the cost was 55.99% of their annual average income.
Patient type, sex, occupation, region, years with cancer, education, marital status, type of cancer were checked if they have a significant relationship with the total cost of cancer treatment. There is no single study that had tried to check such an association, maybe because it is very difficult to justify the relationship between those variables with the total cost of treatment, There is no significant relationship in most of the independent variables like the patients residence and the type of cancer (P = 0.27, df = 16, chi.sq. = 18.92). Women also pay more than the male patients. But being outpatient (P = 0.00) can reduce the cost of treatment by $0.92 when compared to inpatients. Furthermore, the furthest the distance of the patients from the hospital had incurred extra payment (P = 0.01) of $0.23. This is confirmed again by the correlation (P = 0.02) between the distance the patients had traveled and the transportation cost. The association between thyroid cancer and the total cost could be due to the high cost of treatment like physiotherapy and medicine. Knowing the determinant factor allow the policy makers and service providers to identify the area of focus.
Breast cancer is the most prevalent one and needs due attention more than the other 34 types of cancers. Thyroid cancer costs more than the other types of cancers. the cancer treatment service has to be extended to West Arsi zones of Oromiya region in order to minimize the high patient flow from that area. Direct medical and non – medical costs are lower compared to other studies. But transportation and medication cost are the one which escalate these costs. The shorter distance travelled and the few days elapsed on treatment indicated that the service provided is faster when compared to other studies. Generally the average total cost is lower than the studies in other places. But still this is more than half of their average annual income.
Conclusions
Breast cancer is the most prevalent type of cancer compared to other 34 different types of cancer; mostly found in Sidama and West Arsi Zones. Thyroid cancer costs more than the other types of cancer. Transportation cost was the highest of direct non- medical costs and medication cost is the highest of direct medical cost. Services provided in the study area was faster and cheaper as compared to the services in other places. Even though it is lesser as compared to other places, the average total cost of treatment was more than half of the patient average annual income. The cost incurred was mostly from transportation and medication; hence the service has to be extended to West Arsi zone of Oromiya region to minimize the cost of transportation. Furthermore, awareness creation is needed; paying attention to thyroid cancer. Furthermore, facility side study should be done to see the complete picture of the burden.
Footnotes
Authors’ Note
This study was approved by the Institutional Review Board of Hawassa University, College of Medicine and Health Sciences (No. IRB/047/11, dated 26/02/2019). The participation of study participants was voluntary. An oral consent was obtained from all participants prior to their participation in the study.
Acknowledgments
We acknowledge Hawassa University for supporting us to proceed with this research and specifically the Comprehensive Specialized Hospital who allowed us to undertake the research in the hospital. Finally, we would like to appreciate the data collectors who dealt with tiresome activities.
Authors Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.