
Abstract
Background
The second leading cause of death in Italy is cancer. Substantial disparities persist in the level of care and outcomes for cancer patients across various communities, hospitals, and regions in Italy. While substantial progress has been made in medical research and treatment options, these advancements tend to disproportionately benefit the wealthier, better-educated, and more privileged areas and portions of the population. Therefore, the primary aim of the current study is to explore possible reasons for inequalities in access to and utilisation of care from the perspective of cancer patients, who are recipients of these treatments, and healthcare providers, who are responsible for their administration.
Methods
After being recruited through social media platforms, patients’ organisations, and hospital websites, cancer patients (n = 22) and healthcare providers (n = 16) from various Italian regions participated in online focus group discussions on disparities in access to and provision of care. Video and audio recordings of the interviews were analysed using Thematic analysis.
Results
Among cancer patients, 7 themes were identified, while 6 themes emerged from the healthcare providers highlighting encountered barriers and unmet needs in cancer care. Most of these emerging themes are common to both groups, such as geographical disparities, information deficiencies, and the importance of psycho-oncological support. However, several themes are specific to each group, for instance, cancer patients highlight the financial burden and the poor interactions with healthcare providers, while healthcare providers emphasise the necessity of establishing a stronger specialists’ network and integrating clinical practice and research.
Conclusion
Current findings reveal persistent challenges in cancer care, including long waiting lists and regional disparities, highlighting the need for inclusive healthcare strategies. The value of psycho-oncological support is underscored, as well as the potential of the Internet’s use for informational needs, emphasising the imperative for improved awareness and communication to overcome disparities in cancer care.
Keywords
Introduction
Cancer represents a significant global health challenge, with its impact extending beyond the physical aspects of the disease to affect the psychological, social, and economic well-being of individuals and their families. 1 Despite advances in medical science and healthcare systems, one key aspect of this challenge is the existence of health disparities that are differences in health outcomes or access to healthcare among different populations or groups. Health disparities are often influenced by various social, economic, environmental, and structural factors and play a crucial role in influencing cancer outcomes such as survival rates, disease awareness, quality of life, and the mental well-being of patients and their families. Income, education, geographic location, and ethnicity are some of the most important underlying reasons for disparities in cancer across Italy. 2 It is vital to address these disparities comprehensively, taking into account various aspects of the healthcare system as well as the needs of cancer patients. 3 Thus, this study seeks to shed light on these persistent disparities in cancer care in Italy from the perspective of cancer patients and healthcare providers.
The existing literature has emphasised the issue of disparities in cancer outcomes as a matter of critical concern, highlighting several factors possibly contributing to exacerbating such disparities. Firstly, socioeconomic status and ethnic background were found to contribute to disparities in cancer outcomes. Indeed, cancer patients who are at risk of experiencing greater disparities are those with lower socioeconomic status, who are frequently from ethnic minority backgrounds.4,5 Secondly, differences in healthcare infrastructure and accessibility, variations in insurance coverage, cultural and language barriers, and disparities in cancer screening and prevention programs can all play a significant role in creating disparities.6,7 Furthermore, it is important to recognize the geographic dimension of disparities in cancer, as evidenced by various studies. Such disparities are reflected in certain regions in Italy which expose marked geographic inequalities for example in breast cancer mortality rates.8,9 One of the reasons behind geographic disparities in Italy is the decentralisation of the healthcare system, which has determined differences in healthcare access, quality of care, and overall health outcomes across the 20 regions. 10
Moreover, disparities in cancer outcomes can be further compounded by differences in access to information. Cancer patients frequently require information about prognosis, where to seek specific treatments or examinations, the pros and cons of treatment, and where to find psycho-oncological support. 11 The main issue resides in the fact that not everyone has equal access to this information, and when these informational needs remain unmet, they are often associated with decreased treatment adherence, increased healthcare costs, anxiety, and depression.12-14 The Internet has been cited as the most frequently consulted health information resource.15,16 Thus, if digital literacy is well developed, the Internet could be a resource and a means to address these disparities. 17 However, the Internet is not always accessible to everyone (eg, remote areas and rural centres) and even when online information is available to cancer patients, disparities still persist. Indeed, how people discern sources of cancer information online, the barriers and facilitators of online information-seeking behaviours 18 and the reasons behind disparities and variations in such behaviours are still relatively unknown.
Lastly, providing psycho-oncological support was found to be a crucial dimension of equitable care. Generally, the risk of emotional distress is notably higher in cancer patients than in the general population. 19 It is evident that support is needed. However, it is not always accessible to everyone in Italy, with reasons beyond economic factors remaining unclear. In a recent publication, 20 disparities and barriers in accessing, utilising and providing psycho-oncological support were considered. These inequities, rooted in economic factors, resource allocation, and society awareness levels, highlight a lack of specific budgets for psycho-oncological support in 37% of European countries, with mental health not prioritised in many eastern European nations. Socio-demographic factors such as age, gender, education, income, and residence contribute to an uneven distribution of psycho-oncological support, with disparities among cancer types as well. However, further personal barriers, which may be related to patients and healthcare providers, need to be explored more in depth in order to identify and formulate a strategy to overcome them.
Although many factors were identified as reasons for cancer disparities, it is essential to acknowledge that substantial knowledge gaps persist. While some research has delved into the socio-demographic aspects of these disparities, there is a pressing need to go beyond the surface and explore the underlying reasons comprehensively. This entails not only considering the patients’ perspectives but also that of healthcare providers, which play a crucial role in the provision and improvement of cancer care. 21 Furthermore, the literature has not adequately addressed the nuanced barriers encountered by both patients and healthcare providers in their respective roles within the complex landscape of cancer care.
Examining disparities in cancer is important for a number of reasons. Firstly, recent data from the European Commission reveal a concerning 2.4% increase in cancer deaths in Italy in 2022 compared to 2020, as reported in the European Cancer Information System. 22 Additionally, Italy’s cancer incidence rate in 2022 is higher than the EU average, with an estimated 390,700 new cancer diagnoses in 2022, marking an increase of 14,100 cases over 2 years (from 2020). 23 Despite Italy’s commendable efforts in managing cancer risk factors such as smoking and alcohol consumption, there are evident disparities in participation rates in comprehensive screening programs, primarily influenced by factors such as income and education.24,25 These variations underscore the need for targeted interventions to address the root causes of these disparities and ensure equitable access to screening and treatment services across all socioeconomic strata. Secondly, obtaining insights directly from patients and healthcare providers will allow a comprehensive understanding of the challenges and opportunities within the cancer care system. Thirdly, identifying both the barriers and facilitators contributing to disparities in cancer care will enable the development of targeted interventions to address disparities and inequalities.
Thus, the aim of this qualitative study is to explore the underlying reasons and key factors contributing to disparities and inequalities in cancer care, with a specific emphasis on barriers and needs related to diagnosis, treatment, psycho-oncological support, information-seeking behaviours, and decision-making processes of cancer patients and healthcare providers. By addressing these issues comprehensively, we aim to contribute to a more equitable, patient-centred, and effective cancer care system, ultimately improving the lives of those affected by cancer. The present study is part of a wider project named “Cancer Care BEACON'' that will create a decision support tool that aims to assist stakeholders (eg, cancer patients, healthcare providers, researchers and policy-makers) in making informed decisions related to cancer care. For example, these tools will include resources to empower patients in making informed decisions about the most suitable facilities for their cancer needs, to support healthcare providers with education materials and guidelines, to assist researchers in identifying appropriate hospitals for conducting future clinical trials, and to serve policy-makers by collecting information on policy initiatives and reports crucial for informed decision-making in cancer healthcare policy. The BEACON consortium comprises a team of psychologists, oncologists, data scientists and policymakers from different EU countries: European Institute of Oncology (IEO; Italy), SporeData (SD; Estonia), University of Palermo (UNIPA; Italy), the European Alliance for Personalised Medicine (EAPM; Slovenia), and the Klinicki bolnicki centar sestre Milosrdnice ustanova (SMUHC; Croatia).
Methods
Participants
Participants were recruited between April 2023 and November 2023. Eligibility criteria were carefully defined. Cancer patients who were 18 years of age or older, those who had received a cancer diagnosis at any point in their lifetime, or those who were actively serving as caregivers for individuals with a cancer diagnosis were included. Concerning the healthcare providers, participants specialised in cancer diseases (ie, medical oncologists, surgeons, clinical oncologists, psycho-oncologists, palliative care specialists, physical and rehabilitative medicine specialists) and working in an Italian hospital, centre or healthcare facility were included. Additionally, all participants from both groups were required to be fluent in Italian and have reliable Internet access to facilitate their participation in online focus group discussions. Family members or caregivers of cancer patients were included, as well as cancer survivors, in order to provide a wider perspective of the experience of a cancer patient. Exclusion criteria were restricted to individuals without Internet access and those who had not received a cancer diagnosis themselves or were not caregivers to cancer patients. Recruitment was conducted through various social media platforms, such as Facebook and Twitter, hospital websites and thanks to the collaboration of patients’ organisations. A total of 40 patients and 25 healthcare providers and researchers were invited to participate in the discussions.
Procedure
The reporting of this study conforms to COREQ guidelines 26 [see supplementary file 1]. This study was part of the wider BEACON project; the full details of the BEACON study, including objectives and methodologies, are comprehensively documented in the protocol study. 27 The current study specifically focuses on gathering qualitative insights from cancer patients and healthcare providers regarding disparities in cancer care provision or reception. After obtaining ethical approval from the Bioethics Committee of the University of Palermo, all participants were required to provide informed consent, which was obtained through electronic means before the focus group discussions were held. To organise the online discussions of around 50 minutes each, participants were grouped into 5 separate sessions for cancer patients and 4 sessions for the healthcare providers, as data saturation was reached. Each session was moderated by 2 trained psychologists from the who are also co-authors of the present study. Data saturation is defined as “the point at which no new information or themes are observed in the data”. To determine data saturation, we evaluated information redundancy accompanied by a diminishing emergence of new themes in focus group discussions. 28
During the online discussion, GF and VC explained the rules of the focus group discussion, provided more detailed information about BEACON, and guided the group ensuring that all the participants had the opportunity to share their experiences, perspectives, and insights regarding the disparities they have perceived or known of. During the interview field notes of the discussion were taken along with audio-video recordings. Additionally, the online format allowed for geographical diversity, not only in terms of ruralness of residence but also of a variety of Italian regions potentially allowing more heterogeneous responses.
Data Analysis
The analytical process in this study adhered to the key stages of qualitative thematic analysis, as outlined by Clarke and Braun. 29 Data analysis was conducted by two female trained research psychologists (GF, PhD; VC, MSc) independently to ensure robust and comprehensive results. A bottom-up qualitative thematic analysis approach was employed, emphasising the emergence of themes from the data rather than imposing a pre-existing coding framework. This approach allowed for a deep exploration of participants’ experiences and perspectives. In the initial phase, after the transcription of the audio and video recordings of the focus group sessions, and after anonymisation processes, two authors (GF and VC) thoroughly read each text multiple times to become well-acquainted with the content. During the second phase, authors carried out an initial coding of the data, utilising codes to identify segments within the textual reports, based on their semantic content. This process facilitated the systematic organisation of the data. In the third phase, the various codes were aggregated into sub-themes and potential main themes with specific attention to identifying barriers and facilitators as well as the preferences and needs of participants. This step allowed for a deeper exploration of all the nuances within the data. Any discrepancies in coding and theme identification were resolved through discussions among the authors to ensure inter-rater reliability and consistency in the analysis process. In the fourth phase, the emerging themes were further developed and reviewed for coherence and relevance to the research question. This step aimed at refining the themes, assuring they accurately reflected the data. In the final phase, the themes were labelled, accompanied by explicit definitions for each theme to add clarity and transparency to the analysis. To further validate the emerged themes, an author who was not involved in the earlier phases of analysis (DM) scrutinised the entire process and the identified themes. External validation adds credibility and robustness to the emerging themes. 29 The focus group interview guides comprised different open questions aimed at exploring cancer patients’ difficulties in accessing care, potential delays and reasons for delays in diagnosis or treatment decisions, barriers to patients’ information-seeking behaviours and decision-making processes, unmet needs and challenges in accessing psychological support. For healthcare providers, the interview guide aimed at exploring the ways they see integration between clinical practice and innovative research, difficulties in communicating with certain patients, and challenges in participating in multidisciplinary teams. The whole interview guide can be found in the study protocol paper. 27
Results
Patients’ Characteristics
Italian Patients’ Health Status.

Healthcare Providers’ Characteristics
Sociodemographic Characteristics of Italian Patients and Healthcare Providers.

Patients’ Themes
Themes, Sub-themes and Example Quotes From Italian Patients.
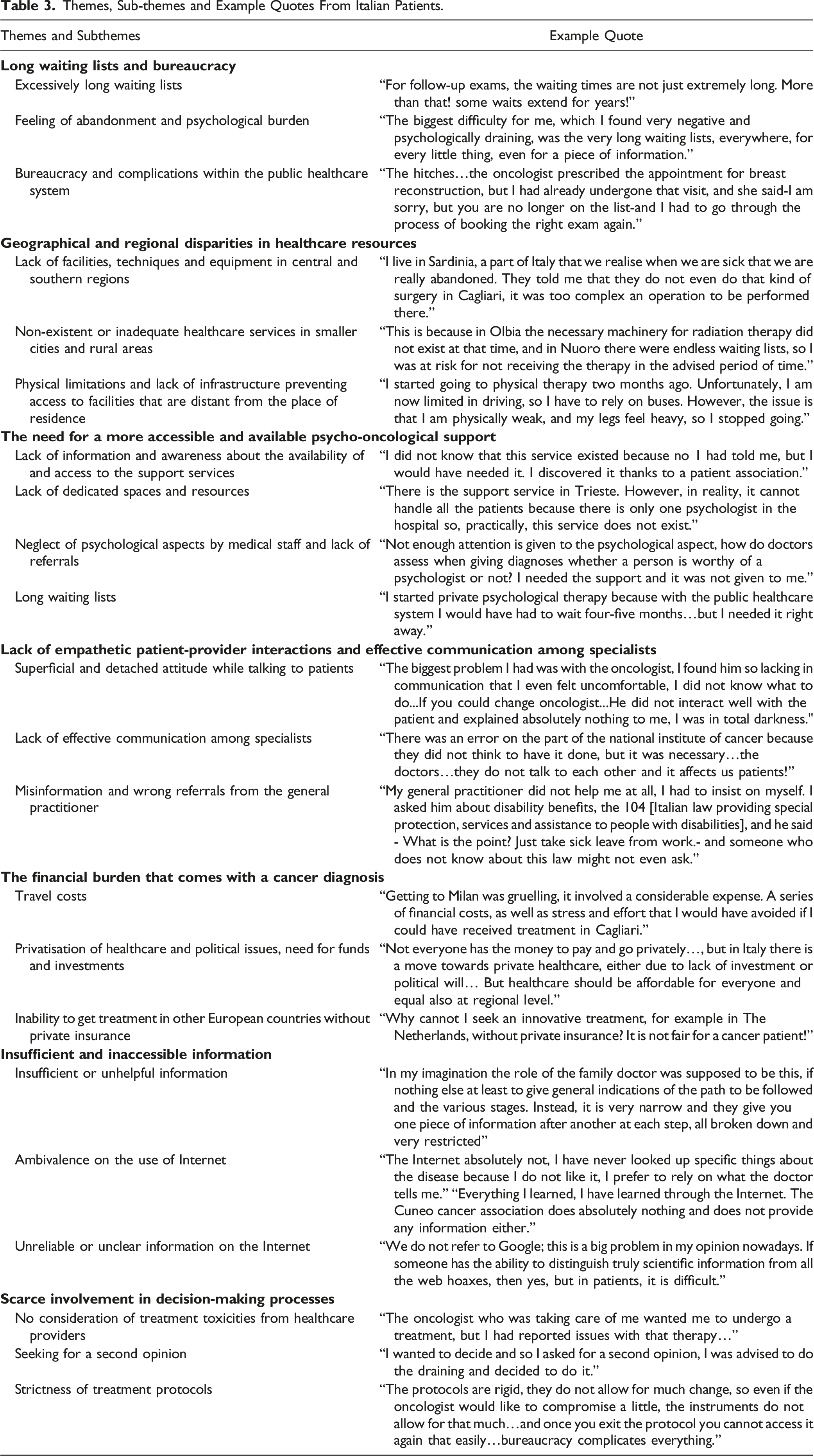
Long Waiting Lists and Bureaucracy
The majority of participants expressed frustration with excessively long waiting lists both for exams and procedures, as well as the reception of useful and necessary information, indicating a need for reduced waiting times to enhance patient access and well-being. Frequently, patients stated that they understood that the Italian medical staff is overloaded with work and patients, nonetheless, they felt abandoned and psychologically burdened by the exceedingly prolonged waiting lists. Moreover, bureaucracy and complication in the public healthcare system were also significant barriers, for more than half of the cancer patients. This includes difficulties in obtaining accurate prescriptions of appointments and medical exams, in maintaining one’s own position in the waiting list, avoiding further delays in diagnosis and treatment. Additionally, rigidity in the sequence of steps, lack of uniformity among regional protocols and subdivision of responsibilities among different professionals, generate difficulties in comprehending the pathways between appointments and exemption possibilities. Specifically, patients do not know whom to turn to for this information and what rights they are entitled to, sometimes discovering them by chance. For instance, one patient complained about the lack of necessary and practical information: “I did not know anything about exemptions. I did not know that Sardinia reimbursed expenses for meals and travel costs. I discovered it after months and months during which I had to cover all the expenses myself”.
On the other side, facilitators in accessing care included having personal connections with healthcare professionals. These relationships foster trust and communication between patients and medical staff. Furthermore, participants appreciated the ease of booking appointments and the efficiency of medical visits and test results, underscoring the importance of a streamlined healthcare system.
Geographical and Regional Disparities in Healthcare Resources
Geographical and regional disparities emerged as a significant concern for the majority of the participants. Indeed, participants reported that the healthcare resources are not equally distributed across different regions. Particularly, cancer patients living in less developed or remote areas, like the islands (ie, Sardinia and Sicily), often face challenges in accessing adequate medical facilities and essential equipment for treating specific types of tumours. The most prevalent barrier, mentioned by the vast majority of participants, was the lack of facilities, training, resources, techniques, and equipment in various hospitals and cancer centres in central and southern regions. Similarly, participants from smaller cities and rural areas experienced greater difficulties in obtaining adequate care compared to those living in larger cities. For example, one patient from a southern region clearly emphasised the issue of regional disparities: “There should be no regional healthcare, but we should all have the possibility of being treated as close to home”.
The Need for More Accessible and Available Psycho-Oncological Support
The majority of participants agreed on the utility and the value of psychological support in the oncological field, with 57.9% of participants having a positive opinion of the usefulness of psycho-oncological support, while 10.5% held a neutral or negative view and the rest did not express an opinion on the matter. However, psycho-oncological support is often lacking due to misinformation and the limited availability of resources and dedicated spaces. Further, many participants expressed frustration with excessively long waiting lists, which hindered their access to psycho-oncological services. Additionally, patients reported to be unaware of the existence of such mental health services. This was the case of one participant, living on an island, who was unaware of the possibility of psycho-oncological support: “I think the support of a psycho-oncologist is very important for the patient and the family, unfortunately in Olbia, there is no psycho-oncologist so who can you turn to?”. In these cases, the support offered through associations, online communities, and the exchange of experiences with fellow patients constituted a valid means of support for the majority of the cancer patients who took part in the current study. In general, patients require comprehensive knowledge of the availability of psychosocial resources to meet their needs and preferences. The utility and importance of patients’ groups could be grasped from the following quote: “I gained great benefit from sharing notes of lived life, which have certainly alleviated my situation. Sharing is a powerful weapon. It helped me through hard times”.
Lastly, some patients who experienced a lack of empathy from medical staff, highlighted the tendency of medical professionals to neglect the psychological well-being of the patients and treat them as “numbers” and not actual people.
Lack of Empathetic Patient-Provider Interactions and of Effective Communication Among Specialists
Another recurring theme that emerged during the focus group discussions, concerned the interactions between patients and healthcare providers. Many of the participants expressed their frustration with what they perceived as a superficial and detached attitude expressed by their doctors. They shared experiences of feeling lost and uncomfortable during their interactions with oncologists, describing a lack of effective communication that left them disoriented. Furthermore, patients recounted instances of misjudgement and misinformation from both oncologists and, especially, general practitioners. General practitioners did not prove useful for most patients, as well as not knowing the rights of the cancer patient, or not being able to refer the patient to the correct specialist. Many patients pointed out the lack of general practitioners, especially in small villages, and their difficulty due to the huge number of patients per doctor. Overall, patients expressed frustration at the healthcare system’s inability to provide them with adequate medical support, assistance with bureaucratic procedures, and guidance on their rights as cancer patients. These interactions emerged as significant barriers to their cancer journey, with a substantial number of patients (45.5%) highlighting dissatisfaction with their general practitioners and an even higher percentage (55%) expressing a desire for more attention and availability from their medical providers.
Moreover, collaboration among specialists was highlighted by a few patients, suggesting that a more cohesive approach among healthcare professionals could lead to improved patient outcomes. Additionally, the neglect of therapy-related side effects was identified as an area in need of attentive consideration. However, the most significant facilitator, as emphasised by half of the participants, was the quality of the interaction and relationship between patients and their medical providers. Patients wished for genuine care, empathy, and open communication from their healthcare team. Furthermore, they stressed the importance of having medical professionals who were readily available to provide support and information throughout their cancer experience, as reported by one participant: “I am lucky because I have a very good general practitioner, he has a 360-degree view of the patient and tells you which specialist to go to depending on what needs to be done”.
The Financial Burden that Comes with a Cancer Diagnosis
The financial aspects of dealing with cancer emerged as a prominent theme during the discussions with cancer patients. Patients voiced their concerns about the economic burdens associated with their illness, particularly in terms of the costs related to travel between regions and from provincial towns to larger cities for treatment. This geographical disparity created a significant financial strain for many individuals and their families. Furthermore, the extended waiting lists for public healthcare services led to another challenge, compelling patients to seek private healthcare alternatives, even for essential psychological support. This private healthcare pathway, though providing quicker access to care, came with substantial costs that added to the financial burden already borne by patients and their loved ones. The financial challenges associated with cancer care were identified as significant barriers to patients’ well-being. Nearly one-third of the participants highlighted the economic costs as a substantial obstacle. The broader issues of healthcare privatisation, political factors, and the need for increased funding and investment were also recognised as barriers by the majority of the participants.
Some patients expressed frustration over the inability to seek treatment in other European countries without private insurance, further compounding their financial concerns. Conversely, the facilitators in addressing these financial challenges were less prominent in the discussions. Only a small number of patients mentioned the importance of financial availability and having insurance as a potential facilitator.
Insufficient and Inaccessible Information
The participants highlighted the critical importance of having access to clear and comprehensible information about available treatment options when dealing with cancer. They expressed their frustration with the often insufficient or unhelpful information provided by doctors, which led them to online searches (ie, the Internet) for more comprehensive insights. However, this reliance on the Internet is not always possible and some patients reported to be aware of the existence of unreliable sources online. Access to reliable information emerged as a great need and a potential facilitator in enhancing knowledge about the disease. Furthermore, the Internet served as a valuable tool for connecting with fellow patients and relevant associations through platforms like Facebook groups and pages.
The barriers to obtaining essential information were multifaceted, with more than half of the participants identifying the lack of awareness about reliable and useful information sources as a significant challenge. Additionally, the shortage of informative and empathetic doctors was highlighted by the participants as a substantial barrier. On the other hand, several facilitators emerged to address these challenges. Almost half of the participants emphasised the value of doctors who are thorough and available in providing the needed information. Some patients expressed trust in medical professionals over online sources, choosing not to turn to “Dr Google.” Word of mouth and personal connections were also considered helpful in gaining knowledge about the disease. Associations dedicated to cancer information and the exchange and discussion with other patients played crucial roles in enhancing understanding. Despite initial reservations, the Internet was recognised as both a facilitator and a barrier. Some patients found it to be a useful source of information, while others mentioned using it to connect with resources and other patients. Additionally, books and scientific literature were mentioned as sources of information by a minority of participants.
Scarce Involvement in Decision-making Processes
The decision-making process within the healthcare context is crucial for patients, and it can be influenced by various factors, as indicated by current findings. The main significant barrier, reported by at least half of the participants, was the limited possibility of actively participating in the decision-making regarding cancer treatment. Most participants stated that healthcare providers made decisions on their behalf and they had to accept it as it was, even when they had concerns about the possible toxicity or had experienced severe side effects. This has led most of the participants to seek a second opinion in another hospital or through a private consultation to be able to express their feelings and concerns about the suggested treatment. A substantial portion of the patients mentioned the strictness of treatment protocols being a rigid barrier to the possibility of active involvement in treatment decisions, reducing the flexibility of available options.
Some participants, however, were able to negotiate changes in their treatment plans based on their health conditions and preferences by taking a firm position and refusing the healthcare providers’ proposals. In addition, several patients requested specific genetic tests as they knew from official sources, or word of mouth, that were crucial to take before surgery or treatment and as a preventive action. They expressed the importance of being the protagonist in their illness and making decisions aligned with their preferences, even if it meant going against medical advice. A stubborn attitude of the patients or their caregivers, and advocacy for informed personal choices have worked as facilitators in making treatment decisions. For example: “I decided not to take the medication. Knowing the side effects of chemotherapy, I said -I am not doing chemo, solve my problem differently- and they listened to me, and they accepted.”
Patients’ Informational Needs.

Note. The current table reports the informational needs that emerged from the focus group transcripts.
Healthcare providers’ themes
Themes, Sub-themes and Quotes Examples From Italian Healthcare Providers.

Excessively Long Waiting Lists and Clinical Workload
First, healthcare providers mentioned the pervasive challenges in providing appropriate care arising from a lack of dedicated spaces and resources in the public healthcare system, resulting in strict time schedules, leaving them with little time even for essential tasks or needs. The combination of insufficient personnel and a scarcity of specialised staff adds to the issue, creating a scenario where healthcare providers are under an overwhelming burden left with little, if no, time for meals or deserved rest, let alone attentive care to patients.
This strain is clearly evident in the protracted waiting lists for patients, underscoring a systemic struggle where healthcare providers find themselves stretched thin, both in terms of physical resources and time, adversely impacting the quality and timeliness of patient care. A participant expressed the issue in the following quote: “Because we do not have enough personnel, there are not dedicated spaces… we are literally chasing the covering of the waiting lists that continue to grow disproportionately…”.
Geographical and Regional Disparities in Healthcare Resources
As well as for the patients, healthcare providers highlighted numerous disparities related to resource allocation in different geographical locations and regions. The vast majority of healthcare providers reported unequal distribution across the Italian regions and areas of financial, structural and personnel resources and diagnostic and therapeutic tools. Several healthcare providers explained how these differences have a crucial impact on the patients’ survival. For example, one participant stated: “The time it took for the medical reports to reach the centre… and everything… five months passed… of course, when the diagnosis arrived, the patient had been dead for a while… and it is unacceptable…”
The limited availability of advanced and innovative treatment and diagnostic tools, as well as the lack of uniformity in cancer diagnosis, also requires the patients who can afford it to travel to the northern regions, adding further workload to healthcare providers and facilities that operate in those better-equipped regions. As reported by the majority of healthcare providers, geographic disparities, mostly regional, are also related to socio-economic factors influencing screening awareness, additional delays due to obsolete equipment and to the fracture between allocated resources and the actual implementation in different regions. This hinders the possibility of having dedicated spaces and personnel that are adequate for the patients in need of care.
The Need for Greater Involvement of Psycho-Oncologists
During the focus groups, healthcare providers emphasised a critical challenge in the limited availability of psycho-oncologists who are specialised in addressing the psychological needs of cancer patients. This scarcity results from a simultaneous lack of specific allocation of resources and dedicated spaces. Another relevant sub-theme that emerged, regarding psychological support to cancer patients, is the indispensable role of psycho-oncologists in facilitating providers’ communication with patients and contributing to shared decision-making processes that are transparent and informed. Psycho-oncological support not only facilitates healthcare providers in managing these challenges but also enhances their ability to engage in empathetic and effective conversations with patients. Participants also emphasised the value of having a psycho-oncologist as an integral part of a multidisciplinary team, emphasising the importance of their constant presence for a better and more comprehensive clinical practice. However, transcripts also highlighted challenges associated with patients’ acceptance of psychological support. Despite the recognised significance of psycho-oncologists, some patients refuse this support, complicating scenarios for healthcare providers. The need for the constant presence of a psycho-oncologist and the patient’s resistance to accepting the support is articulated in the following quote: “The most significant challenges arise in situations where family members recognise the need for psychological support, but patients refuse it”.
Difficulty in Involving Patients in Shared Decision-making
Regarding shared decision-making processes, healthcare providers expressed a genuine desire to involve patients in decision-making, recognising its importance. However, the essence of oncological malignancies, which often necessitate prompt intervention, poses significant time constraints. Providers also acknowledged that clinical protocols, especially in well-studied or less severe situations, might limit the extent to which patients are involved in decision-making. Conversely, in cases of rare tumours where evidence-based interventions are less common, patients are more actively engaged in the decision-making process. The complexity arises from balancing established protocols with individualised choices, as illustrated in the following quote. “It often happens to us to actively involve the patient in the decisions, especially with rare tumours for which we might not have extensive scientific data or numerous studies”.
Another issue for healthcare providers is instances where patient involvement in decision-making is not possible due to a lack of the time and resources necessary to inform the patient regarding all the possibilities, the consequences and the possible impactful side effects; the patients cannot possibly make decisions if they are not properly informed.
The Need for Patient Empowerment
Healthcare providers agreed that the main goal, when speaking of disparities in accessing cancer care, would be that of empowering patients enhancing their awareness regarding prevention, booking procedures, access to treatment programs, lifestyle choices, but, mostly, with regards to their rights as oncological patients. As a matter of fact, issues arise when general practitioners do not inform the patients sufficiently or, as reported by the majority of the healthcare providers, when they are not fully aware of the procedures and management of oncological patients themselves: “The general practitioner is the weak link... they are very overworked and are then the problem.”
Lastly, healthcare providers highlighted how in some regions, such as Piedmont and Sardinia, there is a lack of patients’ associations and organisations which are usually of great help both to patients and healthcare providers. At least half of the healthcare providers emphasised the crucial importance of these associations in providing support and information to patients and, thus, lightening the workload of healthcare providers. Patients’ associations are also helpful in building networks between professionals on a regional and national level and providing help right within the centres or hospitals by both giving directions and informing patients and helping medical staff with administration and bureaucracy.
Limitations in the Integration of Clinical Practice and Research Activities
This last theme highlights the challenges faced by healthcare providers in integrating clinical practice and research activities, pointing to several structural complications. Healthcare providers express a genuine desire to engage in research, but excessive workloads often confine these activities to limited personal time, such as nights, free hours or even holidays. Despite a collective interest in research and a strong belief in its importance, time constraints, insufficient funding, and a lack of resources hinder the extent and quality of research efforts. Notably, a significant sub-theme emerges regarding clinicians being remunerated for research but primarily functioning in clinical roles, indicating a misalignment between roles and actual responsibilities. Indeed, a participant reported: “Right now, clinical work is saving the National Healthcare System because these institutes are full of people whom I call ghosts for the government because they do not know they exist, hired on research funds but doing tons of clinical work”. Bureaucratic obstacles and very slow ethics approval processes further complicate research endeavours, prolonging timelines and additionally burdening the workload.
Discussion
In the current study, diverse cancer patients’ and healthcare providers’ characteristics served as a foundation for an exploration of reasons for disparities in cancer experiences in Italy. Indeed, different barriers and unmet needs possibly contributing to cancer disparities emerged during the online focus group discussions with patients and healthcare providers.
Overall, the identified themes, despite the specificities and uniqueness of the two groups (ie, patients and healthcare providers), show a high degree of consistency and similarity. These themes often complement each other, presenting two different facets or viewpoints of the same complex phenomenon. In particular, barriers related to hospitals, including waiting lists, bureaucracy, and geographical and regional disparities, were frequently reported by all participants. Both patients and healthcare providers expressed concerns about waiting lists and the unequal distribution of resources in hospitals. While patients were found to face the threat of prolonged waiting times, risking delayed treatment and potential compromise to both their survival and mental well-being, healthcare providers were found to navigate an overwhelming workload due to resource shortages. This challenges the providers’ capacity to deliver attentive and timely interventions increasing the patient load and, consequently, lengthening the waiting times for patients. This finding aligns with existing literature, as numerous studies conducted in Italy have highlighted the recurrent issue of excessively long waiting lists in accessing care through the public national healthcare system and how it impacts survival and quality of life. 30 Evident differences in quality and availability of health services arise between regions and a clear fracture is observed between the north and the south of Italy. 31
Furthermore, in both groups, the value of psycho-oncological support emerged. This highlights the recognition of the importance of addressing not only the physical aspects of cancer but also the psychological and emotional burden that comes with a cancer diagnosis. The value attributed to psycho-oncological support by cancer patients in the current study extends beyond the immediate challenges of treatment and recovery. It recognises the long-term psychological effects that a cancer diagnosis can have, emphasising the importance of ongoing support throughout the entire cancer care continuum. Addressing the emotional aspects of the cancer experience becomes essential to promoting resilience, coping mechanisms, and improved overall quality of life for individuals affected by cancer. 32 However, as emerged from our results, the need for psycho-oncological support among cancer patients is often unmet, thus giving rise to disparities between those who have the opportunity to access such services due to awareness or referral, and those who are unaware of the existence of these services in hospitals. This discrepancy underscores a crucial aspect of healthcare inequality, where the accessibility of psycho-oncological support services may be contingent upon factors such as economic availability, information dissemination and referral pathways. 33 In a recent publication, 20 the lack of awareness regarding the benefits of psychological support in cancer patients, and its positive impact on survival and quality of life, hinders both the utilisation of such support by patients and the referral by healthcare providers. In addition, personal characteristics of the patients, as well as those of the healthcare providers, together with socio-economic factors, were found to prevent the access, the use and the provision of psycho-oncological support. 34 On the side of healthcare providers, it became apparent from our results that there is a need for increased awareness and communication regarding psycho-oncological support services. Some patients may not be aware of these services due to a lack of information from healthcare professionals or a gap in communication channels. 35 This points to an opportunity for healthcare providers to play a crucial role in bridging this information gap, ensuring that all individuals, irrespective of their background or level of knowledge, have equal access to valuable psycho-oncological support that can significantly impact their cancer journey. Moreover, in our findings, psycho-oncological support not only proves invaluable for the patients but also serves as a crucial resource for supporting healthcare providers. These support initiatives might act as a means to equip healthcare providers with the necessary tools to navigate the intricate emotional landscape of cancer. 36
Patients’ information needs diverge from those of healthcare providers, yet they are complementary. On one hand, some patients have highlighted their frequent experience of encountering a lack of clear and comprehensive information and poor communication from healthcare providers. This perceived lack of clarity from healthcare providers aligns with the time constraints and stress often reported by providers due to overwhelming workloads, potentially impacting the depth of information provided to patients. In this case, the Internet and online resources could potentially address this misalignment between patients feeling under informed and healthcare providers lacking sufficient time to dedicate to patient informational support. Indeed, the Internet has proven advantageous for both patients and healthcare providers. Healthcare providers recognise the Internet’s value in empowering patients however, they highlight challenges associated with digitalisation, both within populations and hospital systems. Despite the Internet’s potential as a useful tool in overcoming certain barriers, as discussed in a recent publication, it may inadvertently give rise to new obstacles such as the potentially overwhelming abundance of information and the need to distinguish between reliable and untrustworthy sources. 18 For more detailed information see Table 4.
Regarding decision-making processes, patients and healthcare providers shared slightly different yet complementary experiences. In these processes, patients express a desire for increased involvement in managing their illness and gaining a deeper understanding of its impact on their lives. On the other hand, healthcare providers acknowledge the constraints of protocols but aspire to enhance patient inclusion in medical decisions. Recent research highlights the numerous advantages of shared decision-making and active patient involvement in the care process.37,38 In this context, evidence in narrative medicine is noteworthy. This field emphasises the significance of patient and provider experiences through storytelling. Several studies have explored the feasibility and impact of narrative medicine in oncological clinical practice. For example, a digital platform has been developed to elicit guided narratives from patients undergoing chemotherapy or radiotherapy for solid tumours. 39 This innovative approach aims to capture the human side of medicine, incorporating the experiences and reflections of both patients and providers. 40
Lastly, themes that emerged only by patients’ results corresponded to financial burden and interactions between patients and healthcare providers. From the patients’ perspective, the economic burden associated with their oncological diagnosis and treatments was mainly represented by travel-related costs and expenses of private alternatives to public healthcare. This finding aligns with recent data indicating that approximately half of cancer patients experience personal economic challenges tied to the disease and its treatment, a phenomenon referred to as financial toxicity. 41 Patients also reported the issue of ineffective and unsupportive interactions with their healthcare providers. They shared the need to experience empathetic and open communication with their physicians and the desire to be guided with adequate information on bureaucracy and patients’ rights by their oncologist and general practitioner. On the other side, a theme that only emerged from healthcare providers' results corresponded to the difficulty in integrating clinical practice and research activities. Despite the existing interest and desire to conduct research, practical obstacles such as insufficient time and resources strongly affect the extent and quality of the research endeavours.
The current study has important practical implications. First, the significance of psycho-oncological support highlights the necessity for inclusive and integrated healthcare strategies that address both the medical and psychosocial aspects of care. This approach should be accessible to a wider population, as emphasised in Germany’s National Cancer Plan, which aims to offer psycho-oncological care to all cancer patients based on their individual healthcare needs. 42 Addressing such disparities may entail improving communication strategies within healthcare settings, implementing comprehensive training programs for healthcare providers to recognise and address the psychological needs of cancer patients, and establishing more accessible channels for patients to receive information about available support services, such as disseminating and implementing the European Society for Medical Oncology (ESMO) guidelines in many different healthcare systems. 43
Secondly, since there has been an identified need for information, primarily from patients but also indirectly from healthcare providers, it would be beneficial to find a way to disseminate information in a simple and clear manner and provide comprehensive informational materials. The Internet could be advantageous in this regard. Despite the limitations and barriers to Internet access, 18 the dissemination of reliable information online could help mitigate geographical disparities, facilitate access to essential resources, and foster a more informed healthcare community. It is crucial to explore effective strategies to ensure that information reaches both patients and healthcare professionals, promoting transparency and understanding in the healthcare communication landscape. The BEACON project, of which this study is a part, is oriented in this direction with the goal of centralising oncological information and making it publicly available. The objective is to empower stakeholders in the field of cancer, including patients, healthcare providers, researchers, and policymakers, by providing an online decision support tool with critical resources for cancer care and research. 44
The strengths of this study include its multiple perspectives, with our sample involving not only patients but also healthcare providers. Moreover, another strength is the use of the COREQ guidelines to conduct and correctly report the methodology of the current study. 45 Finally, considering the study’s aim to explore the possible factors contributing to cancer disparities, having had the opportunity to include participants from diverse regions, each with distinct clinical and personal histories and backgrounds, can be viewed as an added value that enhances our qualitative investigation.
The results of the study should be interpreted in light of potential limitations. One limitation is the small sample size of our study and the exclusion of a segment of the population, either elderly or those lacking access to devices or Internet connectivity. 46 Moreover, the study is not longitudinal, and such temporal constraint should be considered in interpreting the findings because changes in participants’ perceptions and needs might emerge over time. Accordingly, other reasons for disparities might emerge as well as fluctuate along with participants’ experiences. Additionally, there is a prevalence of breast cancer patients in our sample possibly limiting our exploration of diversity of other cancer diagnoses. Similarly, the majority of healthcare providers operate in urban centres limiting the observation of healthcare dynamics in more remote areas. Despite the effort to implement a sampling strategy as inclusive as possible, the generalisability of the results may be limited by the fact that the participants who accepted are those who are already interested and sensitive to the topic. 47 In terms of future directions, expanding the scope to include more countries and diverse healthcare systems could provide a broader understanding of cancer disparities. Additionally, incorporating longitudinal studies would enable a more dynamic exploration of the factors influencing cancer outcomes over time.
Conclusion
Overall, the findings contribute valuable insights to inform inclusive healthcare strategies and address disparities in cancer care. The study underscores the persistent issue of excessively long waiting lists and regional disparities in accessing cancer care, aligning with existing literature highlighting its impact on survival and quality of life. The value of psycho-oncological support is emphasised, but disparities in access reveal the need for improved awareness and communication. The study also highlights the potential of the Internet in addressing information needs, despite associated challenges. Future directions involve expanding the study’s scope to include more countries and healthcare systems and incorporating longitudinal studies to better understand the evolving dynamics of cancer disparities over time.
Supplemental Material
Supplemental Material - Understanding Reasons for Cancer Disparities in Italy: A Qualitative Study of Barriers and Needs of Cancer Patients and Healthcare Providers
Supplemental Material for Understanding Reasons for Cancer Disparities in Italy: A Qualitative Study of Barriers and Needs of Cancer Patients and Healthcare Providers by Giulia Ferraris, Veronica Coppini, Maria V. Ferrari, Dario Monzani, Roberto Grasso, and Gabriella Pravettoni in Cancer Control
Supplemental Material
Supplemental Material - Understanding Reasons for Cancer Disparities in Italy: A Qualitative Study of Barriers and Needs of Cancer Patients and Healthcare Providers
Supplemental Material for Understanding Reasons for Cancer Disparities in Italy: A Qualitative Study of Barriers and Needs of Cancer Patients and Healthcare Providers by Giulia Ferraris, Veronica Coppini, Maria V. Ferrari, Dario Monzani, Roberto Grasso, and Gabriella Pravettoni in Cancer Control
Footnotes
Authors’ Contributions
GF, VC, MVF, DM, RG, GP conceptualised the study, acquired funding, and planned the design and the methodology. GF, VC, and MVF wrote the first draft of the manuscript. DM, RG and GP reviewed and edited the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the “Beacon Cancer Care” funded by the European Union’s EU4Health Programme (EU4H) under Grant Agreement Number: 101080005.
Ethical Statement
ORCID iDs
Data Availability Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.