
Abstract
Introduction
Cancer patients’ quality of life (QoL) significantly influences treatment response and mortality rates. Understanding QoL domains among patients with cancer and what affects it can help create interventions that improve QoL and ease patients’ experience. This study measures the OoL among patients with cancer and influencing factors.
Methods
A prospective cross-sectional questionnaire-based study included cancer patients aged >18 currently receiving treatment. The questionnaire collected social and economic data, followed by the validated Arabic version of the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire (EORTC-QLQ-C30). Means and standard deviations for described numeric variables and frequencies and percentages described categorical variables. Analysis of variance, F-tests, and P-values were reported.
Results
Among 182 cancer patients, 60% were female. Younger patients exhibited higher QoL in physical and role functioning (P = .016 and .03) and experienced more significant financial impact (P = .0144). Females reported more adverse effects from cancer symptoms, including fatigue, nausea, vomiting, and pain (36.7% vs 25.5%, P = .005; 20.6% vs 11.5%, P = .0186; 34.7% vs 25.1%, P = .0281). Single patients had superior QoL in physical functioning compared to others (P = .0127). Patients traveling long distances were more likely to face adverse financial consequences (P = .007). Asthmatic patients exhibited lower QoL in physical, role, and cognitive functioning (72.3 vs 37.8, P = .0147; 76.4 vs 22.2, P = .0024; 84.7 vs 44.4, P = .0038) and reported increased dyspnea and appetite loss (16 vs 55.6 and 26.1 vs 66.7, both P < .05).
Conclusion
Factors influencing QoL in Saudi cancer patients include age, marital status, gender, hospital distance, and chronic conditions. Thus emphasizing the necessity for personalized care strategies to enhance outcomes and alleviate the overall burden of cancer care.
Introduction
Cancer continues to be a striking global health concern, representing a substantial risk to individuals’ physical and mental health and serving as a primary cause of mortality globally. In contemporary times, there has been an upsurge in the frequency of cancer not only in Saudi Arabia but also in several other countries.1-6 Given the escalating incidence of this ailment, it is imperative to comprehend its ramifications on the quality of life (QoL) of affected patients. Quality of life encompasses a holistic evaluation of an individual’s general welfare and capacity to engage in routine tasks and experience enjoyment in life. The emotional, physical, and psychological well-being of cancer patients may be significantly impacted by the detrimental impact of the disease and its treatment, underscoring the significance of evaluating and managing their QoL.7-9
Several demographic factors have been shown to affect QoL among cancer patients, including age,10,11sex,10,12 distance traveled for care,13,14 and financial difficulties.15,16 In addition, several studies indicated an inverse relationship between QoL of chronic comorbidities among patients with cancer.17,18 One study found that the cancer stage was associated with lower performance status among patients with rectal cancer. 19
Lower performance status may be translated to more symptoms, such as pain and fatigue, which may affect QoL. The relationship between overall QoL and the cancer stage is not straightforward. The strong collinearity between cancer stage and cancer therapy makes it hard to distinguish whether the diminished QoL is due to cancer stage or cancer therapy. Studies either implicate cancer therapy, 20 or implicate cancer stage in affecting physical functioning domains. 21 However, other studies found no differences in overall QoL by cancer stage.22,23
The progress made in cancer therapies has resulted in enhanced rates of survival. However, it is crucial to consider the clinical efficacy of treatments and their influence on the QoL.9,24,25 According to several studies, cancer treatment may result in various physical, emotional, and social obstacles, including but not limited to fatigue, discomfort, alterations in body image, anxiety, and challenges in adapting to social and occupational settings. 26 It is imperative to consider these factors to assist patients in sustaining a superior QoL throughout their cancer experience. The incidence of depression and anxiety is widespread among individuals diagnosed with cancer, and the rates of occurrence are contingent upon a multitude of factors, including the type of cancer, the stage of treatment, and the methodologies employed for assessment. A recent investigation in Saudi Arabia indicates a substantial prevalence of moderate to severe depression (57%) and anxiety (44%) among individuals who have survived breast cancer. These results underscore the need for psychosocial assistance to this population. 27
Evaluating QoL in individuals with cancer entails a comprehensive assessment of various aspects, like physical, psychological, social, and functional well-being. Several research studies have emphasized the adverse effects of decreased quality of life on the advancement of diseases and rates of survival. Moreover, cancer patients frequently encounter symptoms of fatigue, depression, and anxiety, emphasizing the necessity for comprehensive support and interventions to tackle these difficulties.16,28 The quality of life of cancer survivors is influenced by the interrelated factors of their physical, mental, and social health. Notwithstanding the challenges associated with cancer management, many individuals exhibit adaptability and coping mechanisms. Survivors’ quality of life may be significantly enhanced by providing comprehensive survivorship care, support services, and personalized attention to their needs.28-32
Research has indicated a significant occurrence of diminished QoL among cancer patients.20,33-35 Based on a study conducted in Saudi Arabia, a substantial proportion of cancer patients, precisely 50.3%, reported a prevalence of poor overall QoL. 36 Incorporating patient-reported outcome measures may enhance communication, augment patient satisfaction, and facilitate the monitoring of treatment response. Given the region’s distinctive cultural, societal, and health care system attributes, it is imperative to undertake research endeavors to investigate the QoL of individuals with cancer in Saudi Arabia.
This study aims to measure and assess the QoL among patients with cancer in Saudi Arabia. The study augments the current knowledge of factors affecting the QoL of Saudi cancer patients by incorporating indicators such as social well-being, financial status, and treatment efficacy.
Methods
Design and Setting
This study was approved by the institutional review board of King Saud University Medical City, Riyadh, Saudi Arabia, on the 11th of October 2020 (20/0718/IRB). This prospective cross-sectional study was conducted in the Cancer Center, King Saud University Medical City, Riyadh, Saudi Arabia, from October 2020 until October 2021. The reporting of this study conforms to STROBE guidelines. 37
Inclusion and Exclusion Criteria
All Patients above 18 years old who were admitted to the medical oncology day clinic (MODC) to receive their current chemotherapy cycle were included in the study. Patients were excluded if they were not on active treatment, were cognitively unable to respond to questions, or refused to participate in the study.
Sampling approach and sample size calculations
A previous study found that patients with cancer have a QOL score of 65 points on average, with a standard deviation of about 27 points. 38 Using a non-probability convenient sampling approach, the sample size calculation was designed to detect 6 or more points-change in the overall QoL with 80% power using an alpha level of .05. Based on the previous parameters 161 patients were the needed sample size.
Patient Identification
A team of 2 interviewers screened and approached all patients on active treatment in the outpatient clinics during the study period to avoid selection bias. Once a candidate was identified, the aim of the study was explained to the patient, and consent was obtained if they agreed to participate.
In addition, an introductory paragraph was written in Arabic explaining the study’s purpose and rationale to the participants. Verbal consent was taken from the patients, and it was explained to them that participation by answering the questionnaire questions is a form of consenting to participate in the study and getting access to patients’ files for research only. Patients’ confidentiality was always protected as patients’ medication record numbers were de-identified and undisclosed once the data was collected. The questionnaire was filled out during a standardized interview through the two interviewers to ensure consistency between responders and to limit response bias by reducing missing information. During the interview, the interviewers were trained to read the questions to the patients and ask for their responses without adding any words outside the questions except if the patient did not understand them.
Survey contents
In addition to demographic information, patients’ comorbidities, and current cancer treatment, subjects were asked about their income, distance traveled to the hospital, nationality, educational status, marital status, and the number of persons living with them.
The European Organization for Research and Treatment of Cancer Quality of Life Questionnaire (EORTC-QLQ-C30) was employed to measure the subject’s quality of life. 39 The primary investigator contacted EORTC and got permission to utilize the Arabic version for academic research. The EORTC-QLQ-C30 consists of multiple scales that measure different aspects of quality of life, including first, 5 functional scales-that measure physical, cognitive, emotional, social, and role; Second, 3 symptoms scales -that measure nausea and vomiting, fatigue, and pain; Third, 2 items that assess patients’ global health status. Lastly, single questions assessed diarrhea, constipation, insomnia, appetite, dyspnea, and the financial impact of cancer. Except for global health status, all scales were measured on a four-point scale: 1 not at all, 2 a little, 3 quite a bit, and 4 very much. Global health status was measured using a seven-point Likert scale from 1 (very poor) to 7 (excellent). Based on the manual of EORTC-QLQ-C30, all responses were linearly transformed to a 0-100 scale. The higher score represents better functionality and better QOL. On the other hand, in the symptom scales, the higher score represented worse symptoms.
Statistical Analysis
Descriptive statistics were done using means and standard deviation for all numeric variables and frequencies and percentages for all categorical variables. Analysis of variance was conducted, and both F test and P values were reported. To account for the multiple comparisons, Bonferroni adjusted significant levels were reported. 40 Lastly, all needed data was collected, and hence, there was no missing data. All data were prepared and analyzed using Microsoft Excel and STATA 17. 41
Results
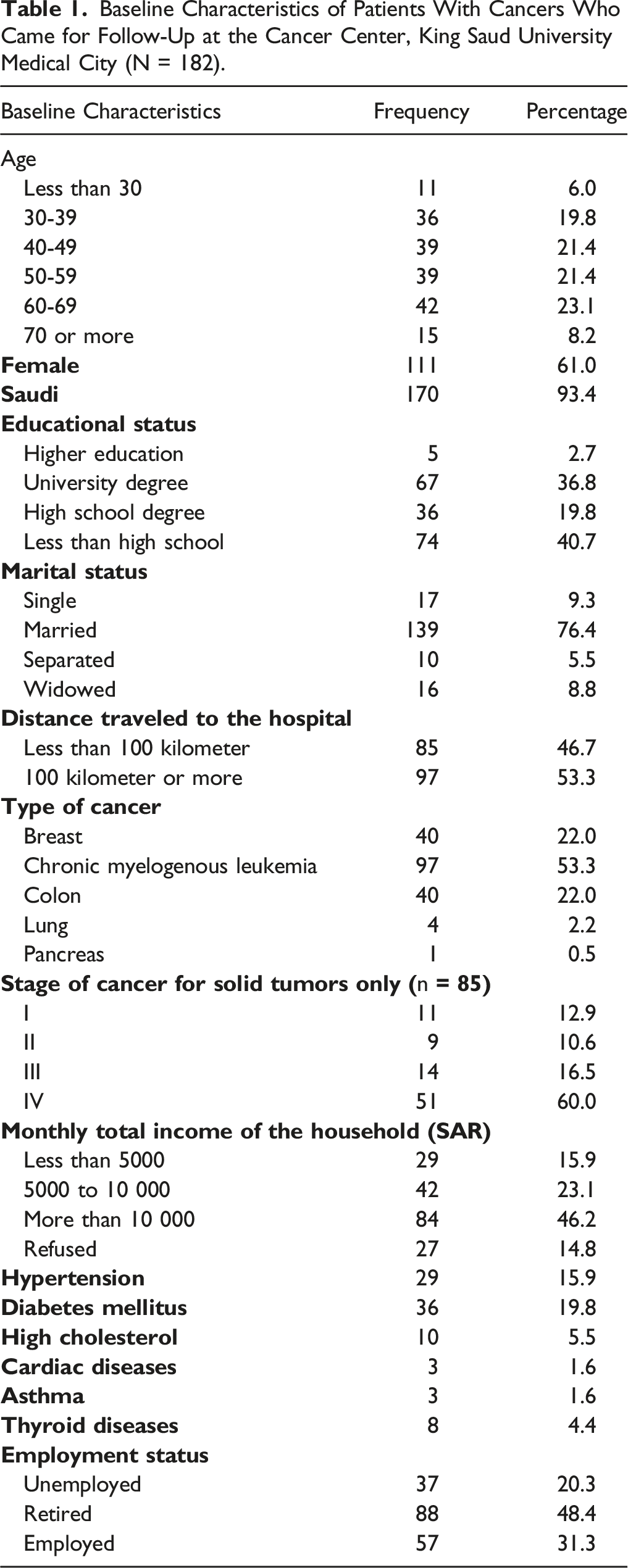
Baseline Characteristics of Cancer Patients
Baseline Characteristics of Patients With Cancers Who Came for Follow-Up at the Cancer Center, King Saud University Medical City (N = 182).
Chemotherapy Regimens Received by Study Cohort (N = 182).

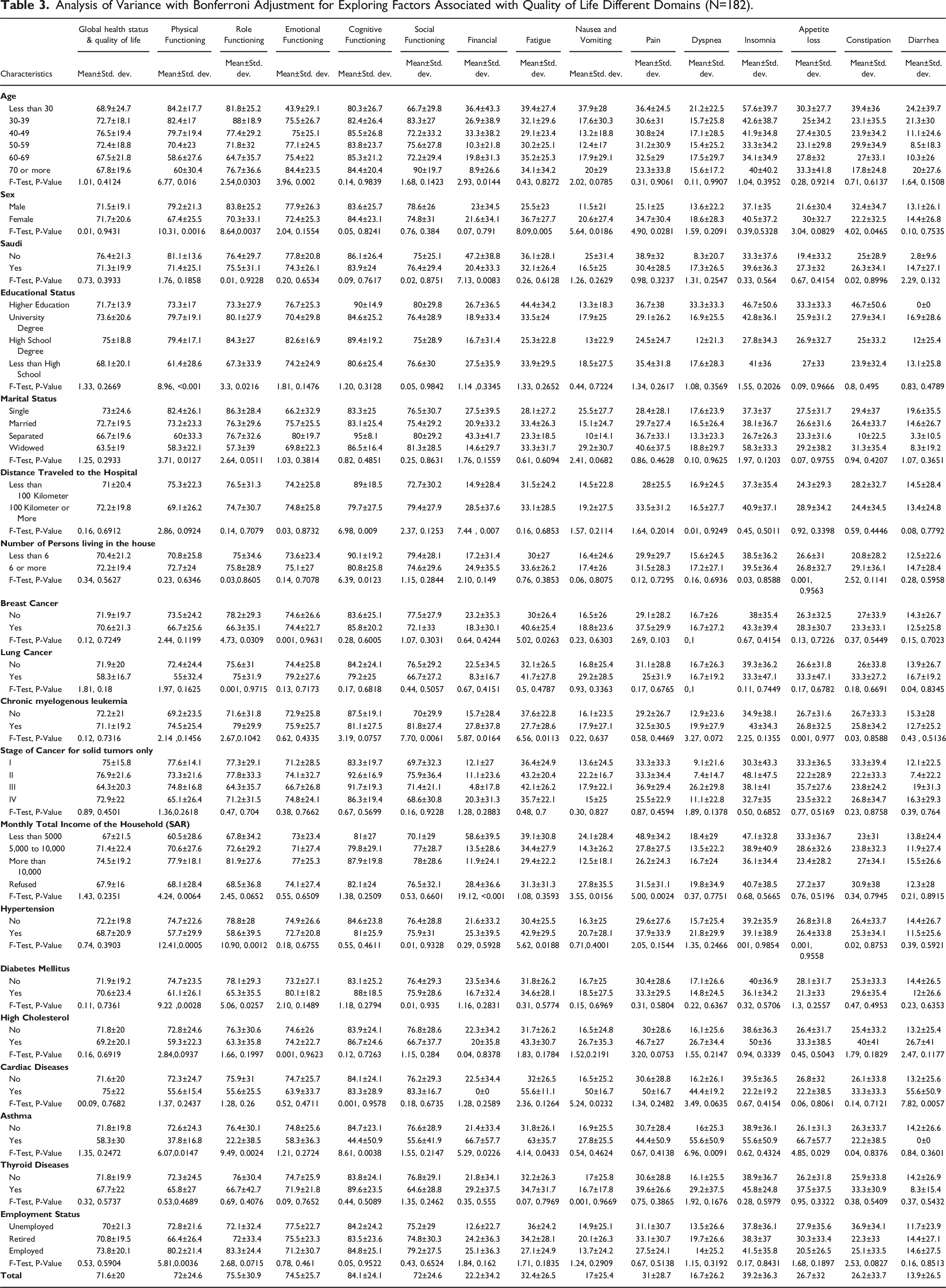
Factors Affecting QoL in Cancer Patients
Analysis of Variance with Bonferroni Adjustment for Exploring Factors Associated with Quality of Life Different Domains (N=182).
Overall QoL Score for Selected Chemotherapy Regimens Among the Study Cohort.

Discussion
This study involved patients with active cancer currently receiving treatment. Several factors were associated with QoL in cancer patients in Saudi Arabia. These factors encompass age, education level, gender, marital status, distance to hospital, household size, cancer type, and chronic comorbidities. It has discovered several variables that seem to be linked to cancer patients’ quality of life. Previous research has also established a correlation between age, level of education, economic position, and quality of life. 42 The research findings provide valuable insights into the factors that impact the QoL of persons diagnosed with cancer. Younger patients with cancer experienced higher QoL in physical functioning and role-functioning domains compared to their older peers. These findings align with previous research indicating that younger patients often exhibit better physical resilience and functional capacity, which may positively influence their QoL during cancer treatment and survivorship.10,43,44 Younger individuals may have fewer comorbidities and better physical fitness, making them better equipped to cope with the physical challenges posed by cancer and its treatments. On the other hand, older cancer patients tend to have higher rates of comorbidities. They may experience more limitations in their physical functioning, potentially contributing to lower QoL scores in this domain. Nonetheless, it is crucial to consider that the specific type and stage of cancer, as well as the treatment regimen, may significantly impact physical functioning across all age groups.
In contrast to younger patients, older cancer patients reported higher QoL scores in the emotional functioning domain. These results may be attributed to various factors, including emotional resilience, coping strategies, and the psychological impact of a cancer diagnosis. Past studies have demonstrated that younger individuals have a remarkably diminished level of well-being, marked by worse physical, social, and emotional functioning when contrasted with older individuals.10,11 Similarly, past studies have demonstrated that younger partners had heightened levels of disease intrusiveness and worse emotional well-being and employed less effective dyadic coping methods. 10 The coping strategies shown by younger couples were impacted by their behaviors and their partners’ actions. 45 This implies that a heightened degree of reliance existed within their connection. The current investigation coincides with past studies, which revealed that the link between mutuality and quality of life in younger patients and older couples was mediated by suboptimal dyadic coping.45-47
The study’s findings reveal prominent gender disparities in QoL within the physical functioning and role functioning domains. Male patients had significantly higher physical and role-functioning QoL scores than their female counterparts. These differences may be attributed to various factors. The study also highlights gender differences in the experience of cancer-related symptoms. Female patients were more likely to be negatively impacted by common cancer symptoms, such as fatigue, nausea and vomiting, and pain, than male patients. These gender disparities in symptom burden are consistent with existing research that has documented higher symptom reporting among female cancer patients. 12 Biologically, hormonal differences between men and women may play a role in the variation in symptom experiences.48-50 For instance, hormonal fluctuations, particularly in the case of breast and gynecological cancers, may contribute to symptoms such as fatigue and nausea. Psychosocial factors may also contribute to these gender differences. Women often report higher levels of psychological distress and may be more inclined to express their symptoms and seek support. 51 Social roles and expectations may shape how individuals perceive and communicate their symptom experiences, with men potentially underreporting symptoms.
The research results did not demonstrate a statistically significant variance in the quality of life between patients of Saudi descent and those of not. However, persons who were not of Saudi Arabian nationality demonstrated a greater likelihood of experiencing negative financial repercussions due to their diagnosis of cancer. This highlights the need to create financial support programs for non-Saudi patients since these efforts may significantly improve their overall QoL. These findings have several implications for health care providers and policymakers. Also, it is essential to address the specific needs of cancer patients who are at higher risk for poor QoL.
Individuals who did not get a high school education saw a decline in their QoL regarding physical well-being and their ability to fulfill societal roles. The observable effects of education on health literacy and access to health care services are noteworthy. Ensuring enough assistance and knowledge on managing their disease is crucial for patients with lower levels of education. This finding aligns with a previous study that reported that individuals with lower levels of education diagnosed with urinary cancer had worse physical, social, and role functioning, as well as advanced incidence of side effects. 52 Studies have revealed a negative correlation between health literacy and physical functioning in older individuals.53,54 The correlation between inadequate understanding, misinterpretations, and ineffective physician communication has been established in noncompliance with cancer therapy. 55
The study’s findings suggest that those who were not married had a higher degree of physical functioning, indicating a superior quality of life. This study’s findings suggest that individuals not involved in a committed partnership may encounter improved physical well-being, which might be attributed to a decreased load of caring obligations. However, the study did not explore the emotional aspects of being single and how they impact an individual’s quality of life (QoL). Previous research findings have demonstrated that those who are married have a greater level of life satisfaction and possess a more extensive social network consisting of family and friends. Studies have demonstrated that older individuals experience a diminished quality of life when their social network is limited. Research has also revealed strong correlations between perceptions of social connectedness and other mental health markers, including sadness, loneliness, and life satisfaction. 56
This study revealed that patients with extensive trips to the hospital reported a worse quality of life regarding their cognitive functioning. The result highlights the need to support those facing travel challenges, such as fatigue and stress, since these variables might influence their cognitive functioning. This discovery underscores the significance of health care service accessibility, particularly for individuals afflicted with chronic ailments such as cancer. Extended travel lengths have the potential to induce heightened levels of stress and weariness and hinder the availability of prompt medical assistance, hence exerting adverse impacts on cognitive performance. To alleviate the challenges faced by patients who must travel significant distances, health systems, and governments should prioritize enhancing infrastructure, providing transportation assistance, and expanding health care facilities. Our finding is in coherence with several past studies that have repeatedly demonstrated that the geographical distance 1 must travel to access health care services may significantly influence an individual’s overall well-being, cancer stage, and satisfaction with life.13,14,57 Studies have indicated that extended trip durations are linked to postponed identification of medical conditions, diminished availability of prompt medical interventions, and heightened levels of stress and anxiety experienced by patients.58,59 Numerous scholarly investigations have proposed implementing telemedicine, establishing local clinics, and providing transportation assistance programs as potential measures to alleviate the adverse impacts of extended journey lengths on the overall welfare of patients. 15
Patients who undertook extensive journeys were shown to have a higher likelihood of encountering adverse financial consequences due to their cancer diagnosis. This finding underscores individuals’ complex and diverse difficulties in undertaking extensive journeys to get health care services. In addition to the physical and cognitive challenges, individuals frequently have financial difficulties.15,16 The financial strain experienced by these people may be intensified due to increased expenses related to transportation, accommodation, and probable income loss, amplifying the overall adverse effects of their health condition.15,16
Previous studies found a negative correlation between higher levels of financial load and quality of life (QOL).15,16 This association is more pronounced regarding physical health than mental health. Additionally, those experiencing higher financial burdens tend to exhibit higher levels of nonspecific psychological distress. The aforementioned financial factors underscore the necessity of implementing financial aid initiatives, travel subsidies, or insurance policies to mitigate the cost burden experienced by individuals.
The observed disparity in average Quality of Life (QoL) ratings between those residing in densely populated homes and those in less densely populated households is a notable discovery with several implications. The cognitive performance of individuals living in densely crowded households was significantly reduced, leading to a poorer QoL. The cohabitation of a significant number of people nearby may lead to increased levels of stress and fewer chances for personal privacy, therefore impacting the cognitive well-being of individuals with cancer. Implementing supportive interventions for patients dwelling in such environments is paramount.60-62
According to Koumarianou et al. (2021), implementing supportive interventions, such as providing resources for family counseling or enhancing living circumstances, may effectively alleviate the adverse consequences of overcrowded homes on individuals' quality of life (QoL). 63 Potential approaches to tackle these challenges involve facilitating individuals' access to housing assistance, offering family counseling services, and giving mental health support. These intrusions enhance patients' overall quality of life and psychological welfare.
Our study results showed that people diagnosed with breast cancer exhibit elevated levels of exhaustion and a worse quality of life, particularly in role performance. Similarly, individuals diagnosed with chronic myelogenous leukemia (CML) have reduced social functioning and increased levels of fatigue. Fatigue is a common phenomenon throughout the populace. Still, it is notably intensified in those who have received a cancer diagnosis, as shown by the investigations conducted by Ericsson et al (2013) and Neefjes et al (2013).46,47 The occurrence of fatigue among individuals who have survived cancer is not restricted solely to the timeframe immediately following the diagnosis and treatment. Therefore, it is essential to detect the presence of fatigue by asking patients about it and teaching them about possible interventions to overcome it. For instance, psychosocial fatigue education and support programs that tackle fatigue-related thoughts and behaviors showed a reduction in the incidence of fatigue compared to standard care.64-66 In addition, acupressure has shown promising results in fatigue reporting among patients with cancer.67,68
Multiple studies worldwide and a few in Saudi Arabia have demonstrated that individuals who have successfully overcome cancer frequently report experiencing fatigue, irrespective of age, gender, or treatment modality.13,48 It is essential to conduct customized interventions to effectively address the symptoms and concerns that are encountered by persons who have been diagnosed with various types of cancer. Earlier studies have discovered that those diagnosed with colorectal cancer had the highest quality of life, while those with lung cancer experienced the lowest levels. Breast cancer patients exhibited a significant prevalence of depression, negatively impacting their social interactions, role functioning, and overall quality of life.49,50 Hair loss, altered body image, diminished sexual functions and libido, and reduced quality of social life were observed as side effects resulting from breast cancer, primarily due to early menopause.49,50 Individuals diagnosed with head-neck and sarcoma conditions may have exacerbated bodily alterations due to their illnesses.
The present study findings indicate that individuals who have received a diagnosis of Chronic Myeloid Leukemia (CML) have worse scores in social functioning and elevated levels of weariness compared to individuals who do not have this diagnosis. Chronic Myeloid Leukemia (CML) management may exert various physical and mental burdens on individuals, potentially leading to social isolation and difficulties in maintaining an active social life. The potential manifestation of unfavorable outcomes aggravates the constraints above. Our findings are consistent with earlier research that highlights the need to provide psychological support and interventions tailored to the specific needs of persons diagnosed with Chronic Myeloid Leukemia (CML) to promote their social well-being. 69 Moreover, the emotional and psychological consequences linked to the phenomenon of living with a chronic cancer condition like Chronic Myeloid Leukemia (CML) may substantially add to feelings of exhaustion. Installing exercise programs or counseling services is crucial in improving the overall quality of life for chronic myeloid leukemia (CML) patients by effectively managing exhaustion. 69
Comorbid chronic illnesses affect cancer patients’ quality of life (QoL), which is crucial to their health. 70 The coexistence of anxiety and hypertension had considerably lower QoL ratings compared to those who didn’t. 71 This shows the necessity of treating hypertension in cancer patients for better health. Several studies have shown that hypertension negatively impacts QoL, underlining the necessity for comprehensive therapy for both disorders.72-76 Our study also demonstrated that cancer patients with diabetes also had worse physical and role functioning. A previous study found that diabetes was linked to a lower QoL for breast cancer survivors. 77 Diabetes has been demonstrated to increase tiredness and physical limits in cancer patients, lowering QoL. Our study has demonstrated that patients with heart problems had higher nausea, vomiting, and diarrhea and decreased quality of life. Cardiovascular disorders may complicate cancer therapy and cause side effects, lowering QoL. Previous investigations have shown that cardiac disorders might cause treatment-related problems, requiring frequent monitoring and supportive measures. 78 Study findings also revealed that cancer patients with asthma had worse physical, role, and cognitive QoL. Such findings about the impact of chronic conditions on QoL necessitate the need for integrative oncology care, which may improve QoL and fulfill patients’ needs. 79
The study also highlighted that younger cancer patients were more likely to be financially impacted by cancer compared to older patients. Financial toxicity in cancer care is a growing concern, as the cost of treatments and supportive care may lead to significant economic hardships for patients and their families.15,80 Although the treatment is free of charge in SA, younger patients may be particularly vulnerable to financial distress due to their potentially more significant economic responsibilities and lower income stability than older patients. Prior studies have repeatedly demonstrated a robust correlation between income levels and diverse health outcomes. Individuals with lower socioeconomic status are more likely to have a greater prevalence of chronic illnesses, limited health care accessibility, and worse overall health outcomes. The topic of income-related health inequalities has been thoroughly examined in various studies conducted.81,82
The provision of financial aid and the accessibility of affordable health care services play a vital role in improving the quality of life for those diagnosed with cancer, particularly those facing financial limitations. Individuals who have received a diagnosis of chronic diseases, such as hypertension, diabetes, and asthma, have been seen to experience a decrease in their overall quality of life, particularly in their physical well-being and their capacity to carry out their various duties and responsibilities effectively. 15
In comparing the current results with Asian countries, the mean global health status among patients with breast cancer in this study was 70.6 (SD = 21.3), which was higher than what was measured among Indian women in the sub-Himalayan region (64.4 ± 29.7) but not statistically significant. 83 All functional scales in this study were higher than those reported among Bangladeshi patients with cancer, which was also reflected by the low global health status score of 48.85 (SD = 19.38). 84 On the other hand, a study that was conducted in Nepal reported a higher mean global health status among Nepali cancer patients (83.3 ± 17.70) despite a high mean financial burden score (68.02 ± 33.81). 85
This study has a few limitations. First, the small sample size might hinder addressing the association between QoL and patient status. Second, the sample included patients receiving both oral and intravenous agents. Both routes of administration may be burdensome on the patients with various side effects. However, oral anticancer agents might have a limited impact on social factors affecting the patient’s QoL. Determining the prevalence of features associated with a decreased quality of life posed significant challenges, primarily due to the vast array of psychological and clinical factors associated with this drop. Lastly, the significant heterogeneity between chemotherapy regions that the study cohort took reduced the ability to study the impact of chemotherapy regimens on QoL. Subsequent research endeavors have to consider a sufficient sample size to comprehensively evaluate the psychological and clinical variables linked with a reduced QoL among persons diagnosed with cancer.
Despite the limitations outlined, this study provides valuable insights into the QoL encountered by those diagnosed with cancer and the diverse array of factors that impact it. By incorporating these factors in health care, there is potential to boost the well-being and overall health outcomes of patients, particularly those with cancer.
Conclusion
Age, gender, education level, marital status, distance to hospital, household size, cancer type, and chronic comorbidities were factors associated with the QoL of Saudi cancer patients. Policymakers and health care providers should routinely evaluate the effect of cancer care on patients’ QoL to improve the outcomes and prevent unwanted associated burdens.
Footnotes
Acknowledgement
The authors are thankful to the Researchers Supporting Project Number (RSP2023R115) at King Saud University, Riyadh, Saudi Arabia for supporting this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The research was funded by Researchers Supporting Project Number (RSP2023R115) at King Saud University, Riyadh, Saudi Arabia.