
Abstract
Background
CAAs are congenital malformations of the auricle ranging from ear underdevelopment to anotia, lacks standardized classification, impacting our outcome of different reconstruction approaches. This scoping review aimed to explore which CAA classifications are most used in current ear reconstruction practices.
Methods
We conducted a scoping review following the PRISMA guidelines, searching MEDLINE and Embase databases on November 1st, 2023. Studies on CAA reconstruction that included clear descriptions of the used classification published in the past 5 years were included. Studies were appraised using the Joanna Briggs Institute checklist.
Results
Out of 293 screened studies, 45 met inclusion criteria, encompassing 19 case series and 5 cohort studies. Findings revealed a predominant use of the Nagata classification across rib cartilage and alloplastic material reconstructions, despite noted application inconsistencies. Other systems like Marx's, Weerda's, and Meurman's remain underutilized.
Conclusion
Most studies used the Nagata's classification. Its widespread use underscores the necessity for an easy to use, but standardized classification to improve surgical outcome reporting and assessment accuracy. Further investigation and standardization efforts regarding the Nagata system are recommended.
Keywords
Introduction
CAA, often referred as microtia, is a birth defect affecting the external ear, ranging from slight underdevelopment to complete absence (anotia). The general prevalence for every 10 000 births amounts to 2.06. 1 CAA may occur with other anomalies such as the Treacher Collins syndrome, craniofacial microsomia or be associated with single gene syndromes and chromosomal abnormalities. 2 CAA is often associated with aural atresia, as well as malformations of the middle ear, which can lead to conductive hearing loss.3,4
There are various classification systems for the diagnosis or documentation of CAA. The more well-known and frequently utilized classifications include those by Weerda et al. 5 There are also the earlier proposed classifications by Marx and Tanzer, 6 and the ones by Fukuda and Firmin. Notably, the classifications by Nagata and Tanzer are closely related to the respective surgical techniques. Within the surgical-based classifications, Nagata made distinctions between lobule, concha, and small concha types. The incision for the lobule type is larger than that for the concha type, and for the small concha type, there is a modification of the usual made incision. 7 Firmin also described a 2-stage reconstruction technique based on the type of severities of CAA, which in turn determined the appropriate incision options. Other researchers have also put forward different classification systems.8,9 However, none of these classification systems encompass all auricular morphologies. As an increasing number of new ear reconstruction techniques are introduced, these classifications, designed specifically for their respective techniques, appear overly rigid when considering other reconstruction methods. 8
Additionally, these classifications focus solely on the morphology of the residual ear, omitting associated deformities. The extent of craniofacial microsomia significantly influences the approach and outcome of Stage 2 ear elevation surgery. Facial asymmetry and the development of the mandible are critical factors in determining the timing of surgery. The degree of external auditory canal atresia dictates the need for canaloplasty and affects the size of the reconstructed auricular concha as well as the sequence of surgical procedures. 10 To this end some scholars have proposed their own classifications based on their surgical preferences and treatment protocols. Campo integrated the classifications and surgical techniques of Nagata and Firmin. Roberson et al have proposed the HEAR MAPS classification based on Hearing, Ear (microtia), Atresia grade, Remnant earlobe, Mandible development, Asymmetry of soft tissue, Paralysis of the facial nerve, and Syndromes, facilitating smooth communication among multidisciplinary teams including ear reconstruction and otolaryngology. 9 However, these niche classifications remain confined to their respective teams, with seemingly no subsequent adoption by other groups.
At this moment, it is unclear which classification systems are currently used most often, and how they are used in the surgical field. Therefore, the aim of this review is to explore which classifications are currently most frequently used in the literature on the surgical reconstruction of CAA.
Method
Search Strategy
A literature review was conducted following the PRISMA guidelines to analyze which classification systems for CAA are currently most commonly used in reconstructive surgery on the external ear. For this purpose, an exploratory search was conducted in the MEDLINE database via the PubMed interface on November 11, 2023 (Table 1). First, the articles were screened based on language and the complete availability. Then, all potentially eligible articles were screened by retrieving their full texts. The screening of articles was done using the Rayyan software (https://www.rayyan.ai/). Initially, our search criteria included articles with participant numbers exceeding 100. However, following reviewer feedback and to broaden the scope of our review, we revised the search strategy. This revision removed the participant number limitation, thereby expanding the inclusion to articles with fewer than 100 participants as well (Table 1).
Literature Search.
Study Selection
An article was included if CAA classification was clearly described. Exclusion criteria included publications in a language other than English. Furthermore, systematic reviews and meta-analyses were excluded. Studies that did not involve CAA reconstructions, or only involved secondary reconstructions were also excluded. Furthermore, a filter has been applied for the past 5 years.
Critical Appraisal
The critical appraisal was conducted using a checklist from Joanna Briggs Institute (https://jbi.global/critical-appraisal-tools). Case series and a cohort checklist were used for the critical appraisal. The case series consisted of 10 items, and the cohort list contained 11 items. Each item on the list could be answered with “yes,” “no,” “unclear,” or “not applicable.” Quality was summarized as “high” if the percentage of “yes” answers on the checklist was more than 80%, “moderate” if the percentage of “yes” answers was between 80% and 50%, and “low” if the percentage of “yes” answers was less than 50% (Supplemental Files).
Data Collection
The following data were collected: year of publication, study design, type of classification, age of patients, and number of patients. Additional data was collected on the descriptions of the used classifications, reconstruction techniques, and the geographical location of clinics.
Results
Search Results
Figure 1 provides an overview of the study selection process. A total of 293 publications were identified through the search and underwent full-text screening. No publication was excluded due to language and availability issues and all of them were reviewed for eligibility. Eventually, 46 publications were included in this review.11–33 Five classification systems: the Marx, Weerda and Aguilar, Meurman, Tanzer and Nagata systems were used in the included articles (Table 2) (Figure 2).
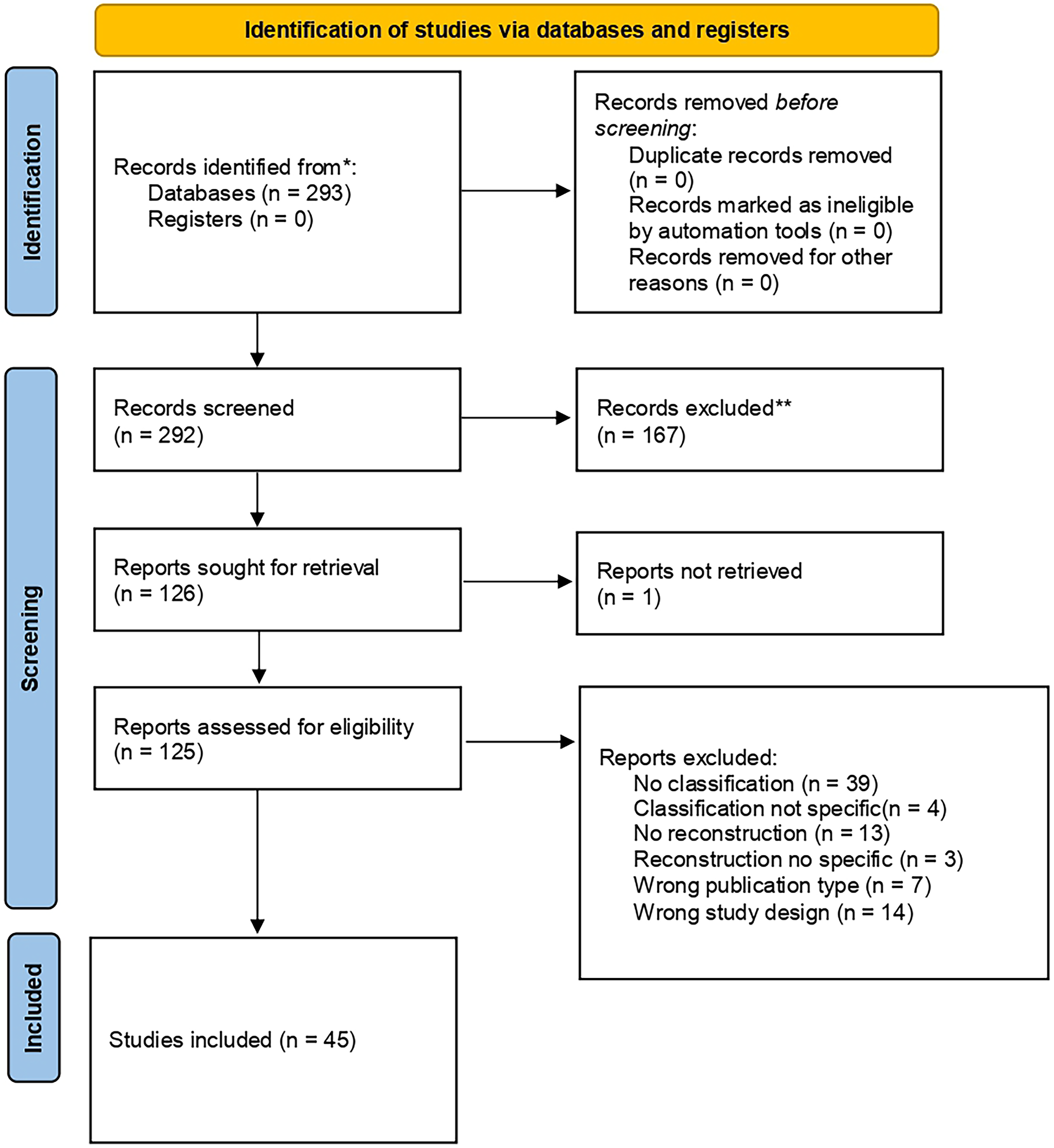
PRISMA flow diagram illustrating the identification, screening, eligibility assessment, and inclusion of studies for the systematic review.
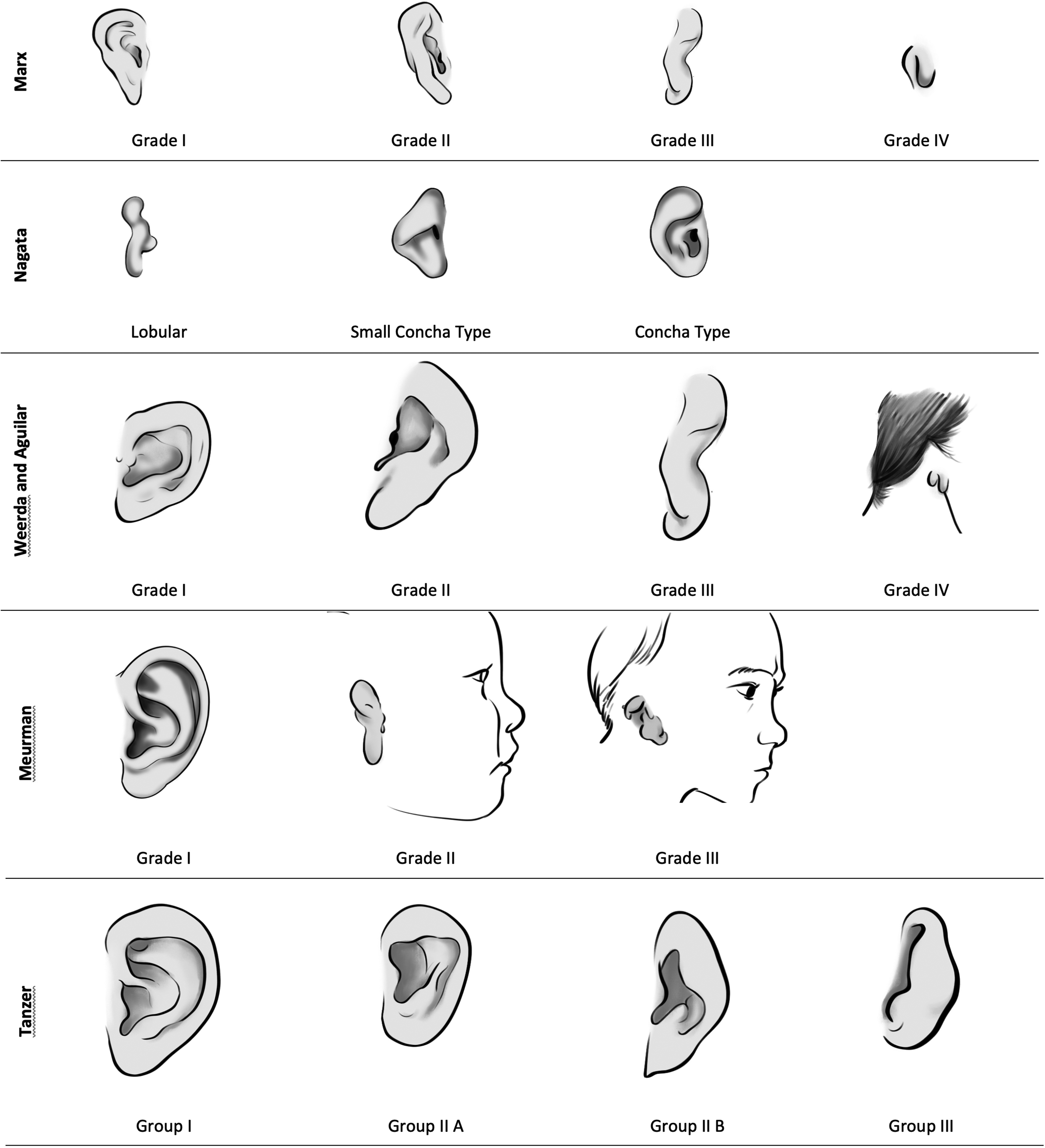
Comparison of various classification systems for CAA/microtia, including Marx, Nagata, Weerda, Meurman, and Tanzer. Each system illustrates distinct grades or types of microtia based on morphological characteristics.
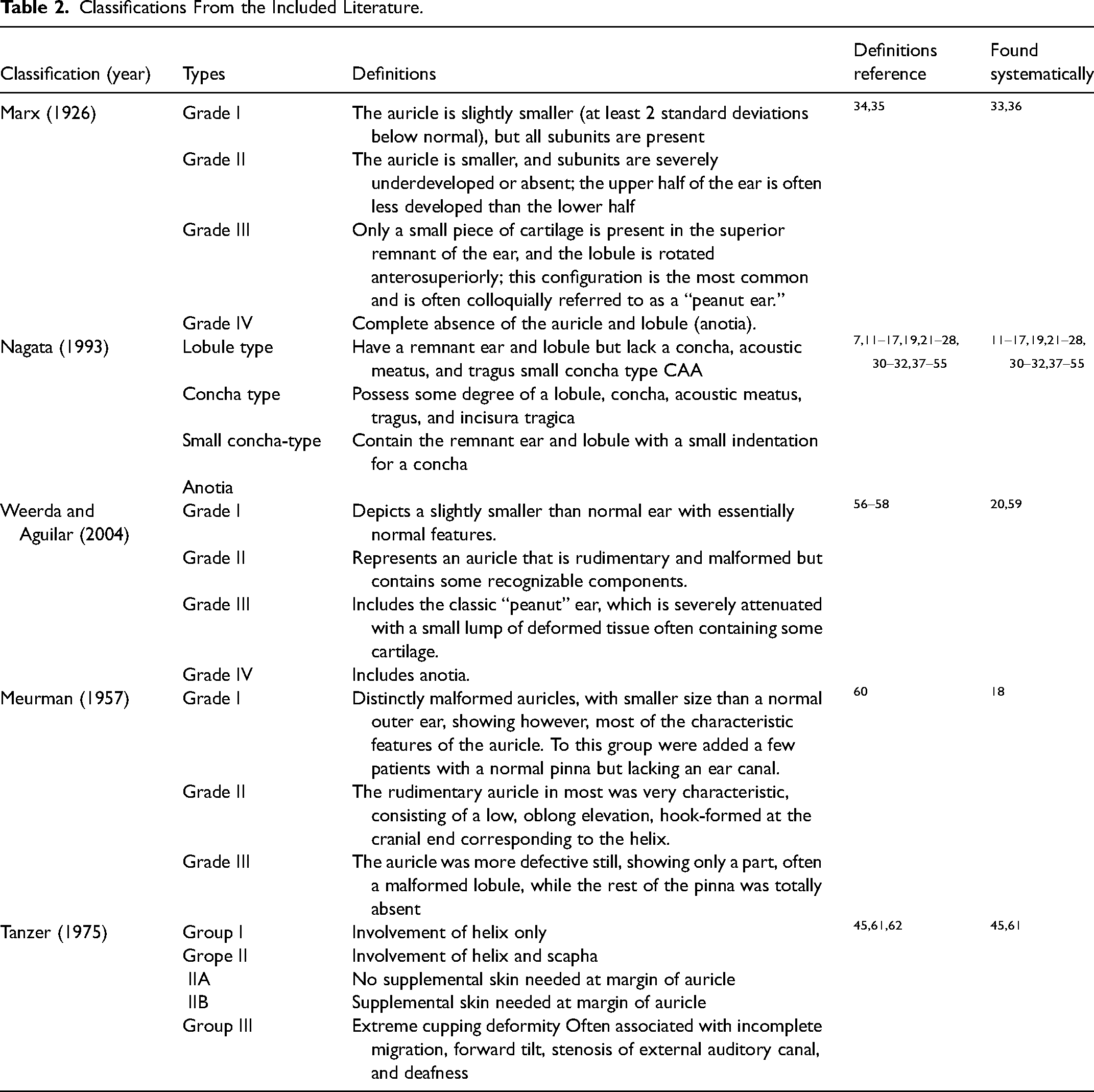
Classifications From the Included Literature.
Study and Patient Characteristic
Table 3 provides a summary of the characteristics of the included studies. Thirty-seven studies were case series11–16,19,20,23–29,31,32,36–52,59,61,63 and 8 were retrospective cohort studies.17,18,21,22,33,53–55 The number of patients per study was between 5 and 1739. The age of the patient ranged from 1 to 55 years. Thirty-seven publications used Nagata's classification to determine the severity of CAA in 11 334 patients.11–17,19,21–28,30–32,37–55 Tanzer's classification was used in 2 studies involving 132 patients.45,61 Marx's classification was used in 2 studies involving 439 patients.33,36 Weerda and Aguilar's classification was used in 2 studies involving 378 patients 20 and Meurman's classifications was used in one study of 410 patients. 18 Finally, Park specifically classified CAA according to the constricted feature in 167 patients. 29
Characteristics of Studies.
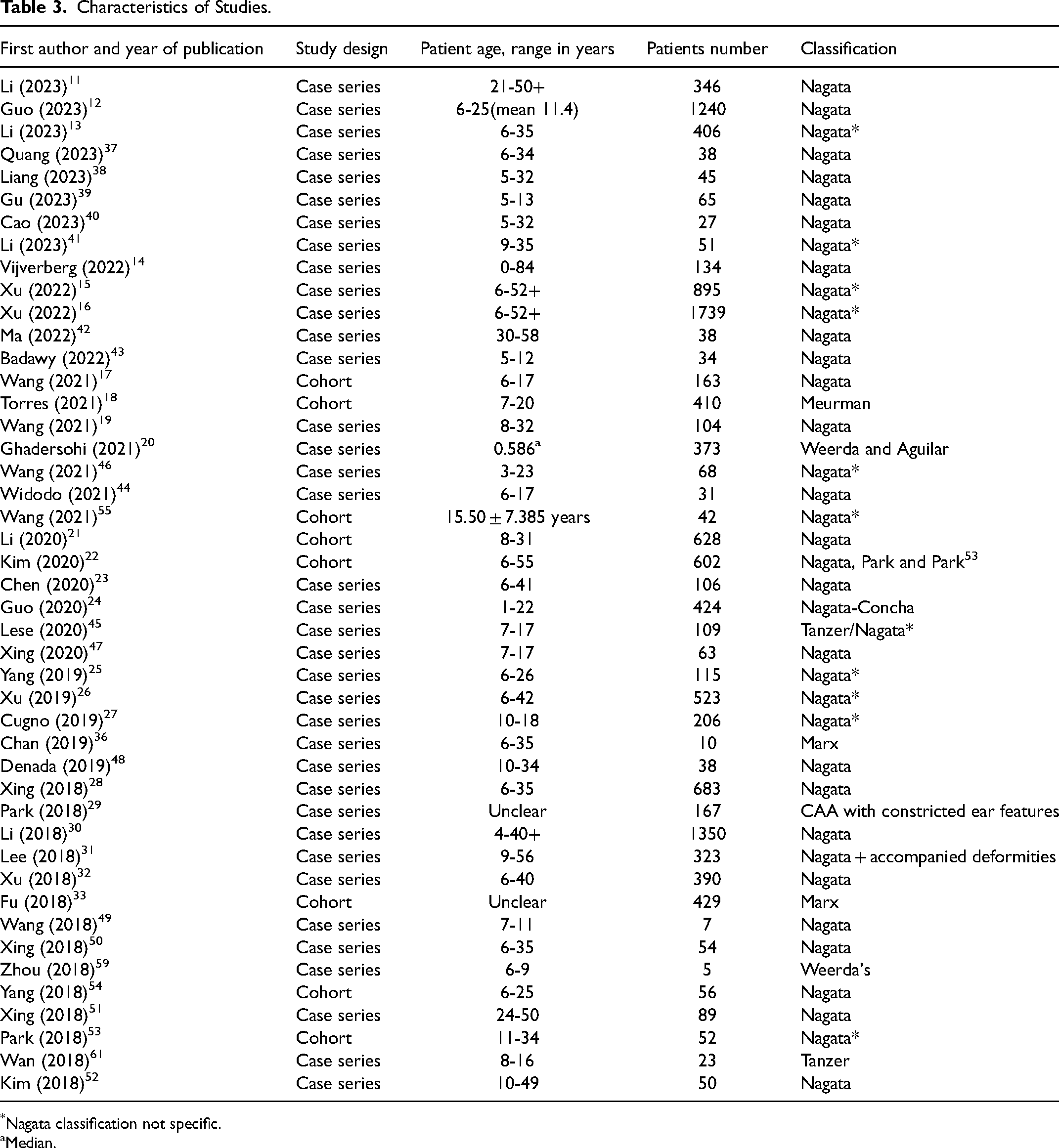
Nagata classification not specific.
Median.
Classification Characteristics
In the articles that used Nagata's classification, the included patients did not always represent all subtypes of CAA (Table 4). Asides from classical lobule, concha, small concha, and anotia type, 7 2 studies further subdivided the lobule type into 2 or 4 subtypes,26,32 while one study further divided the concha type into 4 subtypes. 24 Two articles also described an atypical subtype that is not included in Nagata's classification.14,22
Characteristic of Classification.

Four grading increasing severity characterized by progressive changes in the auricular size, amount of cartilage folded, development of scapha, antihelix, superior crus, inferior crus, and triangular fossa.
Patients number of each subtype not reported.
Nagata classification not specific.
In the studies on ear reconstruction using autologous rib cartilage, Nagata's classification was used in 39 articles.11–19,21–27,30–32,37–39,41–55,59,61,64 Three articles used surgical techniques based on Brent's and Nagata's technique.15,16,20 Two articles described techniques derived from Nagata and Firmin.27,48 Two articles used both Nagata and an expansion method19,22 and 3 articles used only an expansion method.23,25,28,38,46,47,50 Furthermore, 2 articles described self-developed techniques.24,26 One research applied the Mourman classification, and Nagata's method for surgical reconstruction. 18 Tanzer's classification was used in studies applying expansion 61 and the Firmin 45 reconstructive method. One autologous cartilage ear reconstruction study used the Weerda and Aguilar classification. 20
Three articles described the use of alloplastic materials in CAA reconstruction.14,20,46 Specifically, one study utilized the Weerda and Aguilar classification system, 20 while other 2 studies adopted Nagata's classification.14,46
One study used both rib cartilage and Medpor, along with remnant ear cartilage preservation tailored to 4 degrees of constricted-type ear deformities. 29
One study used engineered ear cartilage, where the Weerda and Aguilar classification was used. 59
Fourteen studies exclusively focused on unilateral ear cases,13,17,19,21,22,38,39,41,43,44,48,52,54,61 2 studies only included bilateral ear cases,49,50 and 3 studies included both unilateral and bilateral ear cases for classifying patients.14,45,59The remaining studies did not mention whether their cases were unilateral or bilateral.
In terms of usage across countries and patient numbers, the Nagata classification was used in 8 countries, including 11 334 patients. The Weerda and Aguilar classifications were used in 2 countries with a total of 378 patients. The Tanzer classification was also used in 2 countries, involving 132 patients, while the Marx classification was applied in one country with 430 patients, and the Meurman classification was also used in one country with 410 patients (Figures 3 and 4).
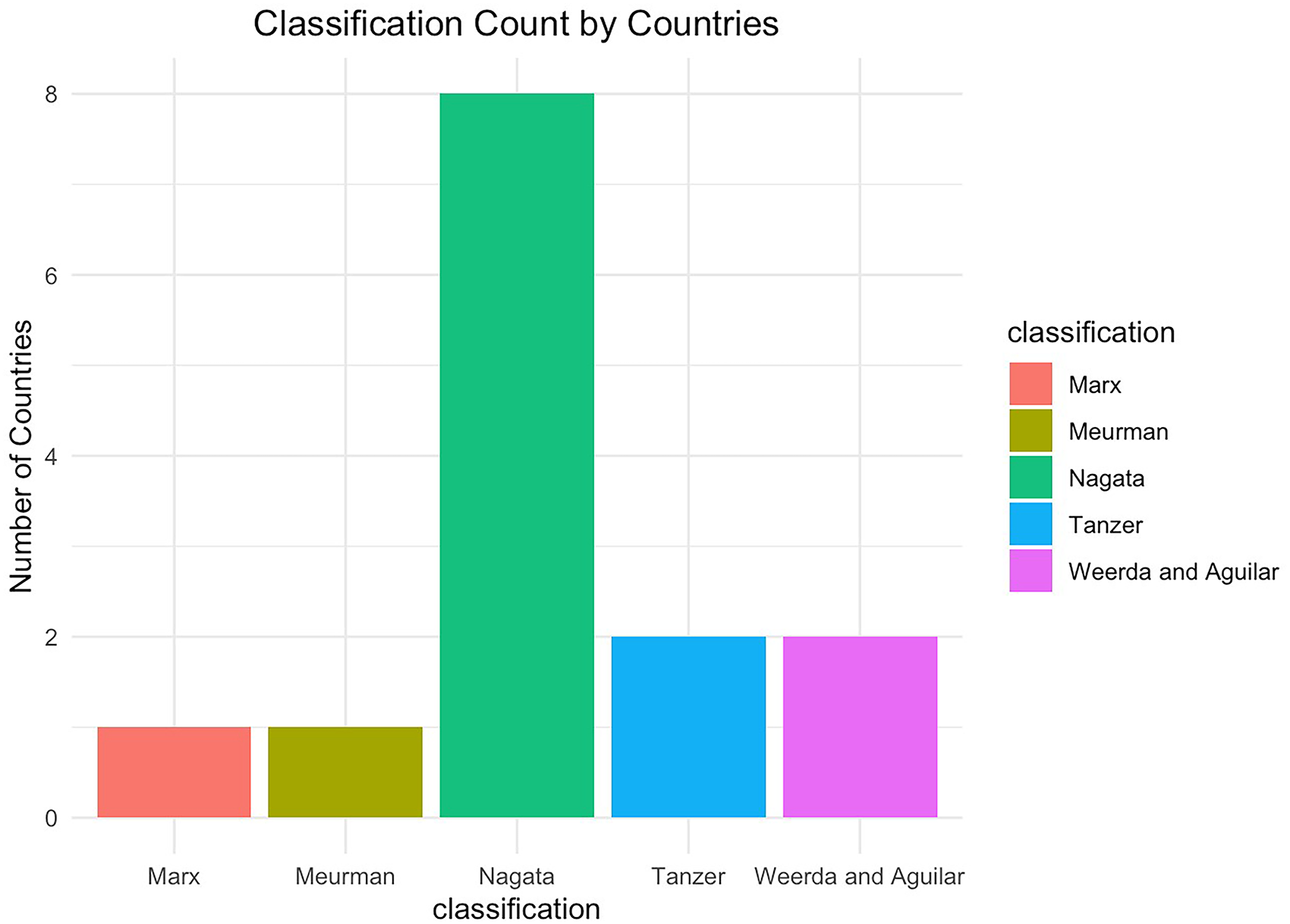
Bar chart illustrating the distribution of CAA/microtia classification systems by country.
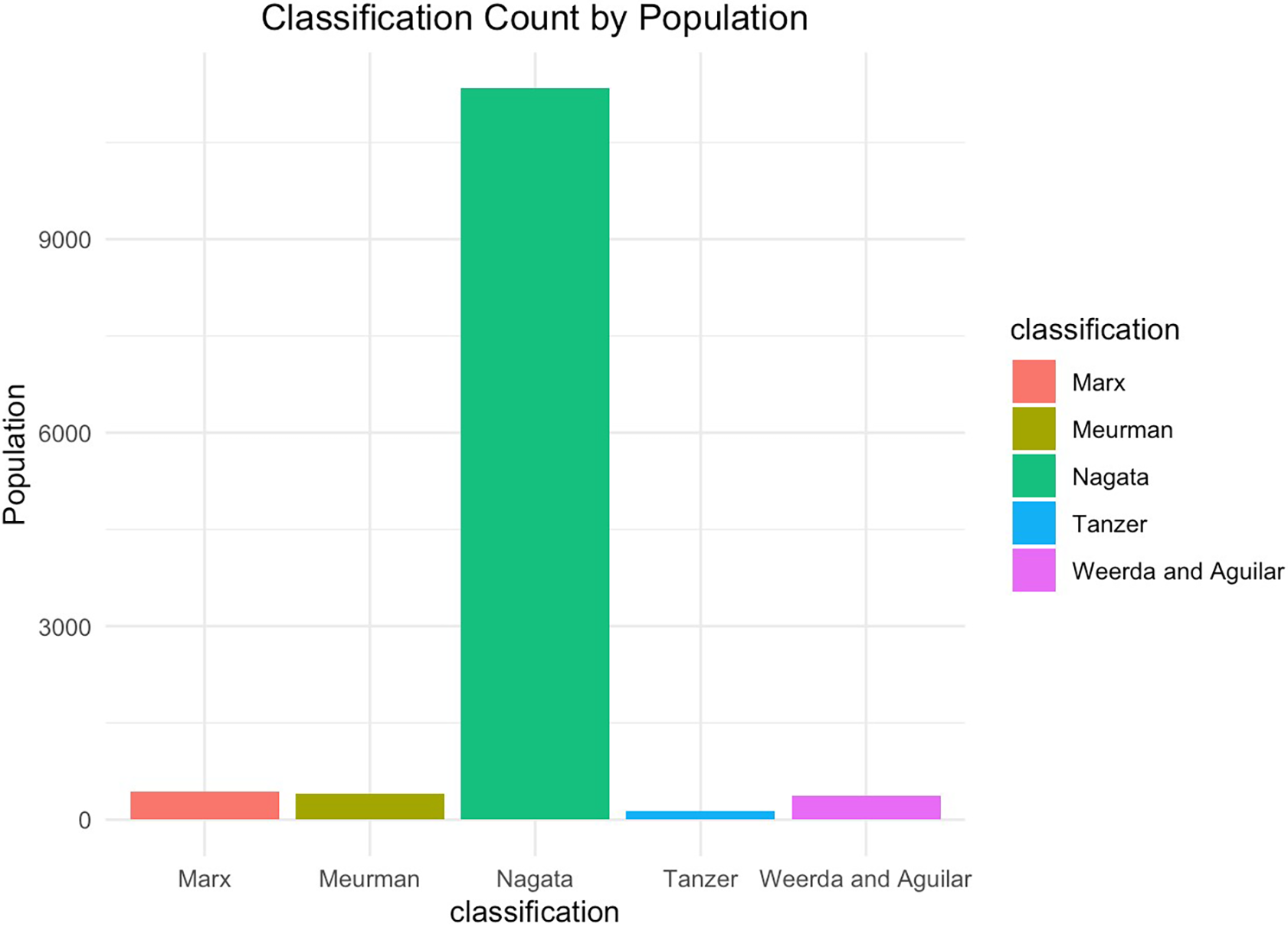
Bar chart showing the adoption of CAA/microtia classification systems by patients population size.
Results Critical Appraisal
Discussion
There is no standardized classification for CAA. As a result, different classifications are used by different researchers and surgeons. This is not efficient for standardizing treatment approaches and analyzing results, nor for international collaboration on treatment and research. This review explored which classifications for CAA are currently most described in the literature on surgical reconstruction.
CAA Classification in Ear Reconstruction With Autologous Costal Cartilage
Nagata's classification was found to be the most widely used classification system of the included studies from the past 5 years. Nagata classification is relevant for determining the incision type for Nagata's surgical technique. 7 The widespread application of Nagata's surgical technique in reconstructive surgeries, as evidenced in all the articles reviewed, likely explains why Nagata's classification was the most utilized in this context.
The other classification systems of Marx, Meurman, and Weerda and Aguilar in the included studies are mostly similar, encompassing descriptions of the size and deformities of the auricle as a whole. In detail, they focus on subunits, components, or features of the ear, which means the number and structure of subanatomical elements such as the helix, antihelix, and concha to determine their normalcy. All 3 systems highlight the classic “peanut ear” lobule morphology. What differs, however, is that Marx's classification provides a more detailed overall description, and Meurman's classification does not include anotia and introduces characteristics of external auditory canal atresia in Grade I. Furthermore, Weerda and Aguilar's classification is aimed at all ear deformities, reflecting their developmental process, instead of focusing on CAA alone. 56 All 3 classifications also utilize a grading approach, reflecting the severity of CAA. In summary, these three clarifications represent an understanding of both the morphology and embryological development of the auricle. However, these classifications may not offer much information for reconstructive surgeries. For example, Grade I in Marx's classification is described as simply a small ear, which may not be an indication for surgery. 65
Tanzer classification was also found to be used by 2 studies.45,61 It categorizes CAA malformation into 3 groups. The first 2 groups are defined by constriction of the helix and/or scapha, with corresponding surgical interventions typically involving otoplasty. 66 Only the third degree is classified as CAA, or microtia, making it relevant for more extensive ear reconstruction. Therefore, while this classification is appropriate for research that focuses on otoplasty, it provides limited information for its application in comprehensive ear reconstruction strategies. 45
In comparison, Nagata's classification focuses on the anatomy of the malformed auricle. The classification is named after the main detailed features (lobule, concha), with each type descripted by ear subunits. These subunits are also aesthetic units of the auricle, 67 that are commonly evaluated for ear reconstructions, 68 reflecting the characteristic of a surgically oriented classification. Nagata's classification was not only used in surgeries specifically employing Nagata's technique but also in other (mainly autologous) non-Nagata ear reconstruction methods. Since Nagata's method is fundamentally an enhancement of Brent's technique, studies using Brent's method for ear reconstruction often employed Nagata's classification.15,16,20 The classification also determines whether remnant ear cartilage can be preserved for auricular reconstruction, thus providing guidance for the expansion methods, as well. Wang et al, for instance, did not carve the tragus and intertragic notch into the cartilage scaffold in patients with concha-type CAA but preserved the original remnant ears. 19 In another study, the use of tissue expanders was also related to the volume of different Nagata types. All patients with anotia required a tissue expander, whereas the lowest usage of tissue expanders (16.2%) was observed in the concha type CAA. 22 The classification details in Nagata's system have also led to the development of new surgical approaches. For instance, Guo et al classified concha CAA into 4 grades, each with specific surgical treatments involving radial cartilage incision, free auricular composite tissue grafting, ear deformity correction, and partial auricular reconstruction. 24 Xu also designed different surgical approaches based on the amount and location of the residual cartilage of 4 types of lobule-type CAA. 32 The variety of the modifications, however, may imply that this surgical based Nagata classification is not detailed enough. Nagata's classification does not fully encompass all deformed ear shapes, as it does not allow for atypical types of CAA. Subsequently few studies describe atypical subtypes of CAA concurrently to the other subtypes according to Nagata.14,22 Patients with small and atypical CAA may require extra aesthetic revisions due to poor cartilage details and aberrant location or have more tendency to not to do ear reconstruction.
The popularity of the Nagata classification likely stems from the historical prevalence of the Nagata ear reconstruction technique, which has shaped the preferences of many surgeons, rather than being inherently specific to Nagata reconstruction or other autologous techniques. Over time, with the emergence of diverse surgical methods such as tissue expansion and Medpor-based approaches, the Nagata classification has been widely adopted across different techniques.14–16,20,46 In our clinical practice, we observed that the mobility of postauricular skin often plays a more critical role in determining the choice of surgical method, influencing factors such as the space available after costal cartilage harvesting or the necessity for distant flaps. Consequently, the value of the Nagata classification increasingly lies in its diagnostic utility for describing auricular morphology, while guiding specific surgical procedures may require more detailed or context-specific classifications to address practical considerations.
The information of low hairline is another valuable insights provided by Nagata classification, significantly impacting surgical planning, postoperative outcomes, and complication risks such as hair growth at the reconstructed auricle or auricle malpositioning.69,70 A low hairline often necessitates alternative techniques, such as TPF/skin graft approaches or alloplastic methods, deviating from traditional 2-stage reconstructions. Despite its importance, our review found a lack of studies categorizing patients by hairline classification, likely due to the absence of standardized definitions or quantifiable criteria. Establishing a standardized framework for low hairline classification within the Nagata system or a future universal classification could enhance research consistency, enable more reliable outcome comparisons, and improve surgical strategies. Addressing this gap is essential for advancing auricular reconstruction methodologies.
Furthermore, Nagata's classification only details the auricle. CAA is often combined with varying degrees of craniomaxillofacial deformity, which in turn influences surgical decision-making and postoperative evaluation of auricle reconstruction. Facial asymmetry and the development of the mandible are critical factors in determining the position of reconstructed ear. The most caudal location of the earlobe is determined by its relative relationship to facial structures. Moreover, surgeons are also aware that patients with low hairlines are more challenging to reconstruct. To this end, a comprehensive assessment including the patient's cranial symmetry, associated deformities, the morphology of the mastoid, and the necessity of external auditory canal formation is essential for a complete plan for ear reconstruction. In this context, the HEAR MAPS classification proposed by Roberson et al offers a more holistic approach. 9 This classification system provides a valuable framework for integrating ear malformations with broader craniomaxillofacial anomalies. Such integration is paramount for enhancing the precision and quality of surgical outcomes. Only one study comprehensively addressed these aspects, 31 highlighting the underutilization of such thorough assessment strategies in current research and practice. However, the HEAR MAPS classification categorizes ear deformities simply into “normal,” “mild,” “moderate,” and “anotia,” similar to the categorizations by Marx providing less surgically oriented, detailing specific anatomical information as Nagata classification. Combining the HEAR MAPS and Nagata classification could therefore significantly benefit the field by improving patient care and standardizing the approach to complex cases involving CAA and associated anomalies.
A comprehensive and standardized classification system is useful for both clinical practice and research. Kim et al identified a correlation between the subtypes of CAA, as classified using Nagata's classification, and the necessity for canaloplasty and secondary aesthetic revisions. This suggests that the subtype of CAA can influence the outcomes of surgical procedures. 22 However, the lack of comprehensive reporting on subtypes of CAA limits our interpretation of these results. This study also found inconsistent use of terminology from Nagata's classification, with many employing other terms for subtypes,15,16,25,26 for example, “sausage type” for “lobule type.”21,25 Furthermore, clear classifications and results for bilaterally affected ears were limited. A well-structured and understandable classification system aids in guiding surgical choices and predicting outcomes, contributing to better-informed decisions by both surgeons and patients.14,71 Future studies on ear reconstruction should therefore include clear descriptions of the classification method used, and report results based on subtypes of CAA.
CAA Classification Ear Reconstruction With Other Materials
The use of the classification systems in alloplastic surgeries was sparse and inconsistent. Vijverberg14 and Ghadersohi20 did not clarify how Nagata's classification, or Weerda and Aguilar's classification, guided the decision to use alloplastic materials in their studies. In Park's research for constricted CAA, Medpor was used as a supplement to autologous rib cartilage. 29 This suggests that exploring the further classification applicability in alloplastic surgeries could be valuable.
Notably, a recent study utilized engineered ear grafts for auricular reconstruction. 59 In this study, patients with CAA classified as Grade II or III according to the Weerda classification were included, ensuring that the severity of the deformity matched the capabilities of the engineered grafts. However, the subsequent surgical techniques employed were the expansion and the Nagata method. The selection of surgical technique heavily relied on the skin tension in the retroauricular region, a factor not fully addressed by the Weerda classification. Currently, there is a paucity of clinical research on engineered ear reconstruction, with only one other study from 2009, which did not specify any classification. 72 Moving forward, the use of engineered ear reconstruction techniques will likely necessitate the development of new classification systems or the adaptation of existing ones to better suit these innovative approaches.
The coverage of healthcare costs associated with ear reconstruction and the application of classification systems in this process are also important factors to consider. These surgeries typically require 2 to 4 sessions over a period of up to 2 years and can be quite costly, underscoring the importance of accurately assessing the necessity for ear reconstruction. Currently, medical insurance predominantly utilizes the simplified International Classification of Diseases coding system, which assigns a single code for CAA and another for anotia.73,74 The Marx classification is also used by insurance companies, providing a clearer guidance for making surgical decisions. 57 For instance, Marx Class I involves only minor ear size reduction, where nonsurgical treatment may be needed. 75 Marx Class II and higher clearly indicate significant absence of ear cartilage, typically necessitating ear reconstruction surgery.33,36 In comparison, the Nagata classification directly dictates how to perform ear reconstruction. It does not explicitly advise whether surgery should be undertaken. 57 Therefore, integrating the use of the Marx classification can have significant practical implications in real-world settings, offering a more comprehensive framework for surgical decision-making based on the severity of ear deformities.
However, a classification including all necessary information detailed above will likely add further complexity and subjectivity to the classification of CAA and involved craniomaxillofacial malformations, which is not practical in everyday practice nor is it conducive to the development of a broad consensus among researchers. In the past few years, automatic characterization of the craniomaxillofacial region has become a hot topic of research. Convolutional neural networks have been applied in identifying ear abnormalities. 76 Vanessa et al 77 used 3D landmarking to evaluate the deformity indexes in patients with cleft lip and palate. Meng et al 78 further used deep learning to perform automated cephalometry in patients with craniofacial microsomia. There are numerous automated assessment algorithms for facial assymetry.79,80 These are common concomitant craniomaxillofacial anomalies of CAA. Therefore, an automated 3D algorithm could potentially be developed to create an integrated classification system that is easy to use and considers both auricular and craniofacial anatomy. Considering smartphone-based applications within 3D imaging, this could provide a global alternative for the future. 81 Currently our unit is in the process to create an automated algorithm to determine ear position. 82
Another barrier to consensus in classification is the subjective differences among scholars, influenced by regional ear aesthetic standards 83 and personal surgical preferences. Additionally, advancements in reconstruction techniques drive the need for more detailed classifications, which further increase subjectivity and heterogeneity, impeding academic communication. Thus, an objective and unified classification system is urgently needed. The unbiased automated clustering method based on ear morphology is an innovative approach that combines artificial intelligence and machine learning. 84 By objectively analyzing the morphological features of many ear samples, the algorithm can automatically cluster these features, creating a data-driven ear classification model. This approach integrates vast amounts of data and expert input, significantly reducing human bias and enhancing classification consistency.
A key advantage of this algorithm is its scalability and adaptability, allowing for dynamic adjustments based on the latest academic feedback. 85 As such, international platforms like International Society of Auricular Reconstruction (ISAR) provide an ideal platform, enabling the collection of global expert opinions to continually optimize ear classification models. Ultimately, this automatic clustering approach can achieve an objective and automated classification system for ear reconstruction, aligning with ISAR's mission of fostering international collaboration. 86
Limitations
This article also has some limitations. A methodological limitation lies in the fact that this review only included studies within the latest 5 years. This was done due to the exploratory nature of this review. This may have led to selection bias, whereby articles using other classifications may have been missed. In addition to the previously mentioned HEAR MAPS classification system, another well-known classification system, the Firmin classification, was not found in this search, although one article used the Firmin reconstruction but Nagata/Tanzer classification. 45 Language may constitute another significant limitation in our study. Although our search was comprehensive within English-language publications, the majority of the literature came from China. This overrepresentation might not fully reflect the diversity of classification preferences used globally, partly because China is both a populous nation and a high-prevalence country for CAA. Including literature in multiple languages in future reviews would allow us to develop a more comprehensive classification system, thereby enhancing our understanding of global practices and nuances.
Conclusion
Nagata's classification is widely recognized in CAA reconstruction studies and is independent of the reconstruction technique. Its broad applicability across various techniques underscores its versatility. However, its applicability to atypical forms and alloplastic techniques requires additional investigation. Further development of classifications like Nagata's that also integrate comprehensive information on craniofacial and related anomalies could provide more precise and comprehensive surgical planning. Incorporating 3D automation technology could be an effective way to refine and unify various classification systems, offering a more detailed assessment of CAA and associated structures. Consistency in using classification terms is crucial for advancing treatment and research in CAA.
Supplemental Material
sj-docx-1-cpc-10.1177_10556656241310101 - Supplemental material for An Overview of the Currently Used Congenital Auricular Anomalies (CAA) Classifications for Surgical Reconstruction: A Scoping Review
Supplemental material, sj-docx-1-cpc-10.1177_10556656241310101 for An Overview of the Currently Used Congenital Auricular Anomalies (CAA) Classifications for Surgical Reconstruction: A Scoping Review by Yangyang Lin, Elsa M. Ronde, Lieve de Voort and Corstiaan C. Breugem in The Cleft Palate Craniofacial Journal
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Chinese Scholarship Council (Grant No. 202107720090).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.