
Abstract
Objective
In managing sagittal craniosynostosis, strip craniectomy of the affected suture is commonly paired with barrel-stave osteotomies to allow for additional cranial remodeling. However, the effect of these osteotomies is not well-established. This study aimed to evaluate the effect of the length of barrel-stave osteotomies on outcomes in patients with sagittal craniosynostosis.
Design
A retrospective review of operative records and pre-operative and one-year post-operative three-dimensional images.
Setting
Tertiary care pediatric institution.
Patients
Forty-five patients with sagittal craniosynostosis
Interventions
Sagittal strip craniectomy and either long, medium, or short barrel-stave osteotomy lengths followed by helmet therapy
Main Outcome Measures
Operative and three-dimensional craniometric outcomes.
Results
Operative time, estimated blood loss, and hospital length of stay were significantly decreased in the short group (P = .003; 0.002; 0.027). The cranial index was normalized in all groups, but the long group was significantly lower (P = .007; 0.025). Head circumference was similar between groups. All indexes were within the normal percentiles in all groups. The medium group had a significantly decreased scaphocephalic index (P = .031; .035). The short group had significantly greater occipital bulleting than the medium group (P = .001). The long group had significantly greater narrowing than the short group (P = .036).
Conclusions
Strip craniectomy with the addition of long, medium, or short barrel staves all resulted in clinically successful outcomes. Our findings suggest that increased barrel-stave osteotomy length may not be necessary for a successful outcome while avoiding more extensive dissection, potential risk, increased operative time, and hospital length of stay.
Keywords
Introduction
Strip craniectomy for sagittal craniosynostosis involves the removal of a strip of bone adjacent to the fused sagittal suture, allowing for skull expansion with either helmet or spring-based molding. 1 Jimenez and Barone described the addition of barrel-stave “wedge” osteotomies extending laterally from posterior and paralleled to the coronal sutures and anterior and paralleled to the lambdoid sutures. 2 Since then, many modified techniques using strip craniectomy have been described,3–20 most commonly including barrel staves. 21
However, the effects of the length of the barrel-stave osteotomies have yet to be examined. Increased osteotomy length requires more extensive lateral dissection, potential risk, and increased operative and anesthesia time. This study investigates the effects of barrel-stave osteotomy length on surgical outcomes following strip craniectomy for sagittal craniosynostosis. We utilized three-dimensional photography to evaluate differences in post-operative outcomes.
Methods
A retrospective review of 45 consecutive patients with sagittal craniosynostosis who underwent strip craniectomy followed by helmet therapy was performed following institutional review board approval by the University of Texas Southwestern Medical Center. Immediate post-operative computed tomographic images were reviewed to determine barrel-stave length. The distance from the sagittal suture to the squamosal suture was identified as the maximum possible barrel-stave length, and patient cohorts were defined by the length of the osteotomy compared to the maximum. The three groups included long (>75%), medium (50-75%), and short (25-50%) (Figure 1). Patients with mixed barrel-stave osteotomy lengths were excluded. Three-dimensional photographs pre-operatively and at one year of age following strip craniectomy were collected for craniometric and three-dimensional image creation. Our previously described standardized helmet therapy was used in all patients. 22 Medical records were reviewed to collect demographic, diagnostic, and operative interventions. Head circumference and cranial index were measured.
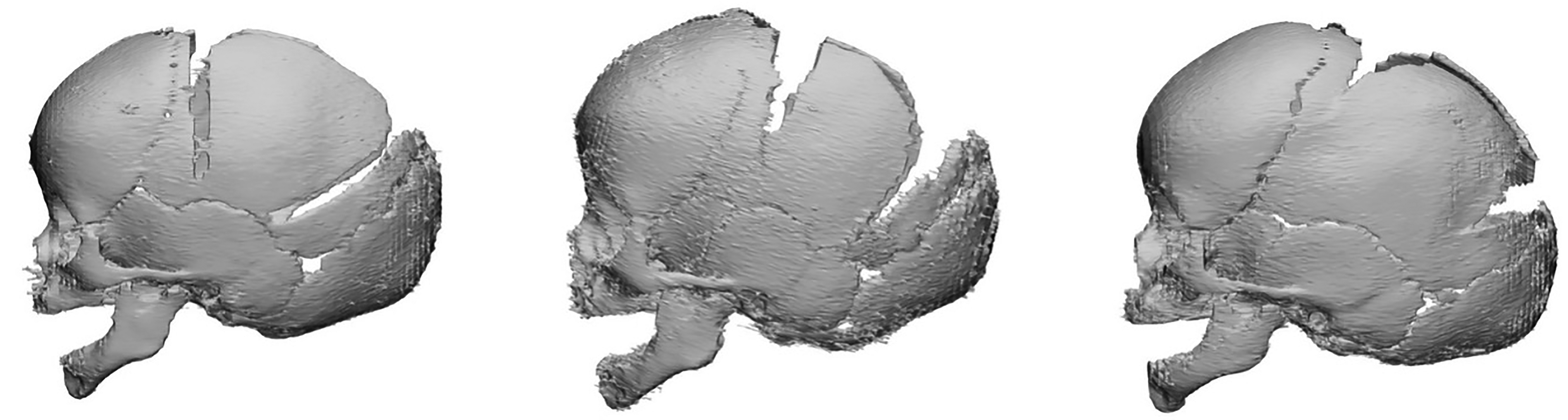
Strip craniectomy with barrel-stave lengths long >75% (left), medium 50-75% (middle), and short 25-50% (right).
Craniometric Measurements
The cranial index was calculated as width divided by length. Circumference was measured at the widest point on the head. Measurements were performed with standardized planes using 3dMD Vultus (Atlanta, GA). Scaphocephalic, frontal bossing, occipital bullet, and vertex narrowing index were evaluated based on previously published techniques.23–25 Briefly, the indices are calculated as regional abnormality divided by sellion protrusion. The frontal bossing index is calculated as anterior protrusion divided by sellion protrusion. The occipital bullet index is posterior protrusion divided by sellion protrusion. Combining the fontal bossing index and occipital bullet index creates the scaphocephalic index. The vertex narrowing index is the width protrusion divided by the sellion protrusion. These values are used to provide a percentile in comparison to normal control patient's cranial head shape.
Composite Heat Map Analysis
Composite pre-and post-operative head shape were created for heat map comparison to age matched controls using our previously described mathematical models.14,26,27 Warmer colors (red) indicate greater convexity compared to age-matched controls, and cool color (blue) indicate greater concavity compared to age-matched controls. Statistical analysis was performed to calculate totals, percentages, and averages with standard deviation.
Surgical Technique
Limited incision extended sagittal strip craniectomy with barrel-stave osteotomies was performed in all patients by a single surgeon. Incisions measuring approximately 4-centimeters in length were designed posterior to the anterior fontanel in a transverse orientation, as well as anterior to the lambda. Dissection was carried from anterior to posterior, as well as to posterior to anterior in the subgalea plane. The anterior fontanelle and single burr hole at the lambda were used for intracranial access. A bone window was created to allow for epidural dissection along the sagittal suture. Once this was complete, a 5-centimeter wide craniectomy was performed with bone scissors. Barrel stave wedge ostectomies were designed, extending from the lateral aspects of the central strip ostectomy towards the squamosal sutures between 1-2 cm in width. The length of the barrel stave was decided intra-operatively based on the safety of dissection and visualization while maintaining minimally invasive incision and exposure. The length was not based on the severity of the scaphocephalic deformity. The wedges were designed anteriorly to follow 5 mm behind the coronal sutures and, conversely, on the posterior aspect, angled anteriorly to parallel the lambdoid sutures.
Results
A total of 45 consecutive patients were included, with 15 patients in each of the three groups (Table 1). The age of operation was, on average, approximately three months in all groups. Operative time was significantly decreased in the short barrel-stave osteotomy group at under 2 h compared to the long and medium groups. The estimated blood loss and hospital length of stay were also significantly decreased in the short barrel-stave group. No patients had non-healing cranial defects. Age at pre-operative and post-operative imaging was similar between groups. No patients had non-healing cranial defects.
Strip Craniectomy with Barrel-Stave Osteotomy Length Groups.
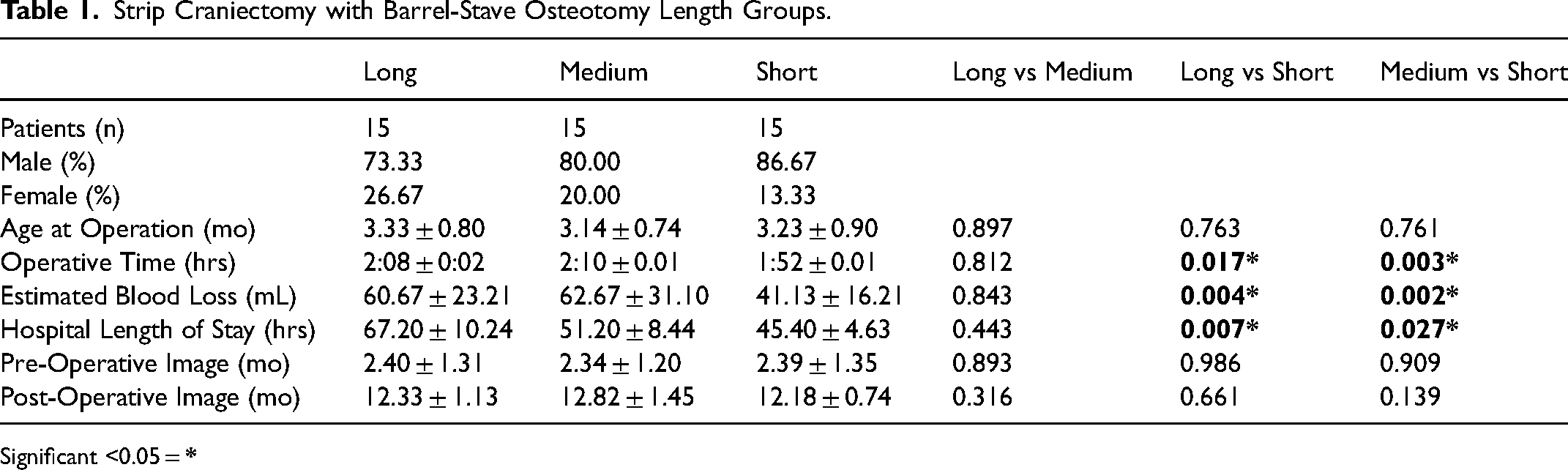
Significant <0.05 =
The average post-operative cranial index was within the normal range in the long, medium, and short barrel-stave groups (Table 2). The average cranial index in the long barrel-stave group was significantly lower than in the medium and short groups. The average post-operative circumference was similar in all groups. The scaphocephalic index of all groups fell within the 61 to 85th percentile of the control population. 23 The medium barrel-stave group had significantly decreased scaphocephaly than the long and short groups. The frontal bossing index averages were between the 90 and 96th percentile of the control population. There were no significant differences between the three groups. The occipital bullet index fell between the 66 and 87th percentile of the control population. The short barrel-stave group had significantly greater occipital bulleting than the medium group. The vertex narrowing index was around 30 to 50th percentile of the control population. The long barrel-stave group had significantly greater narrowing compared to the short group. However, with multivariable analysis accounting for pre-operative differences between groups only the
Sagittal Craniosynostosis Long, medium, and Short Barrel-Stave Length Craniometric Measurements.
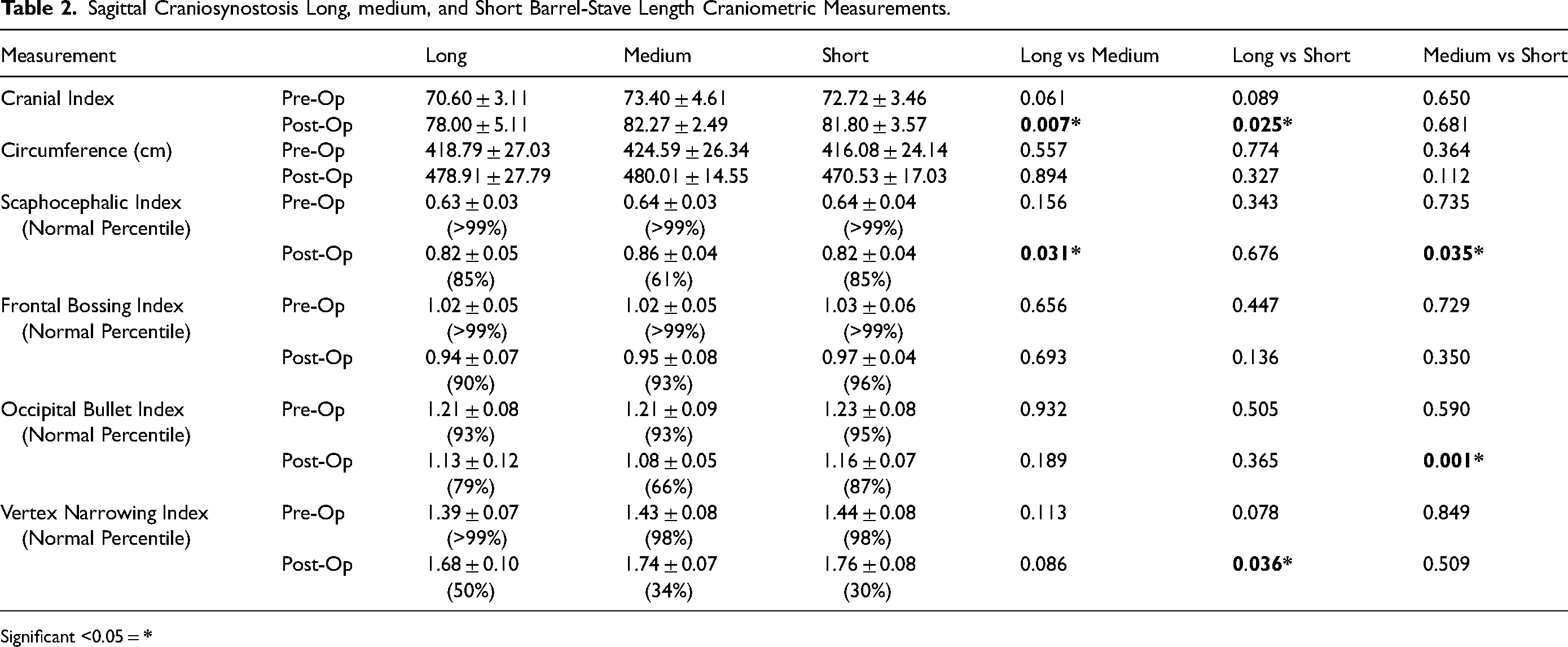
Significant <0.05 =
The pre-and post-operative composite heat map comparison to age-matched controls is shown in Figure 2. Pre-operative features are similar across the long, medium, and short barrel-stave groups. Intense warm colors indicated convexity of the forehead and occipital regions. The bi-temporal and parietal regions also have intense cool colors, indicating concavity. The post-operative images demonstrate similar improvements in all groups. Mild warm colors are present at the vertex. No intense warm or cool colors are present in the forehead, occiput, temporal, or parietal regions.
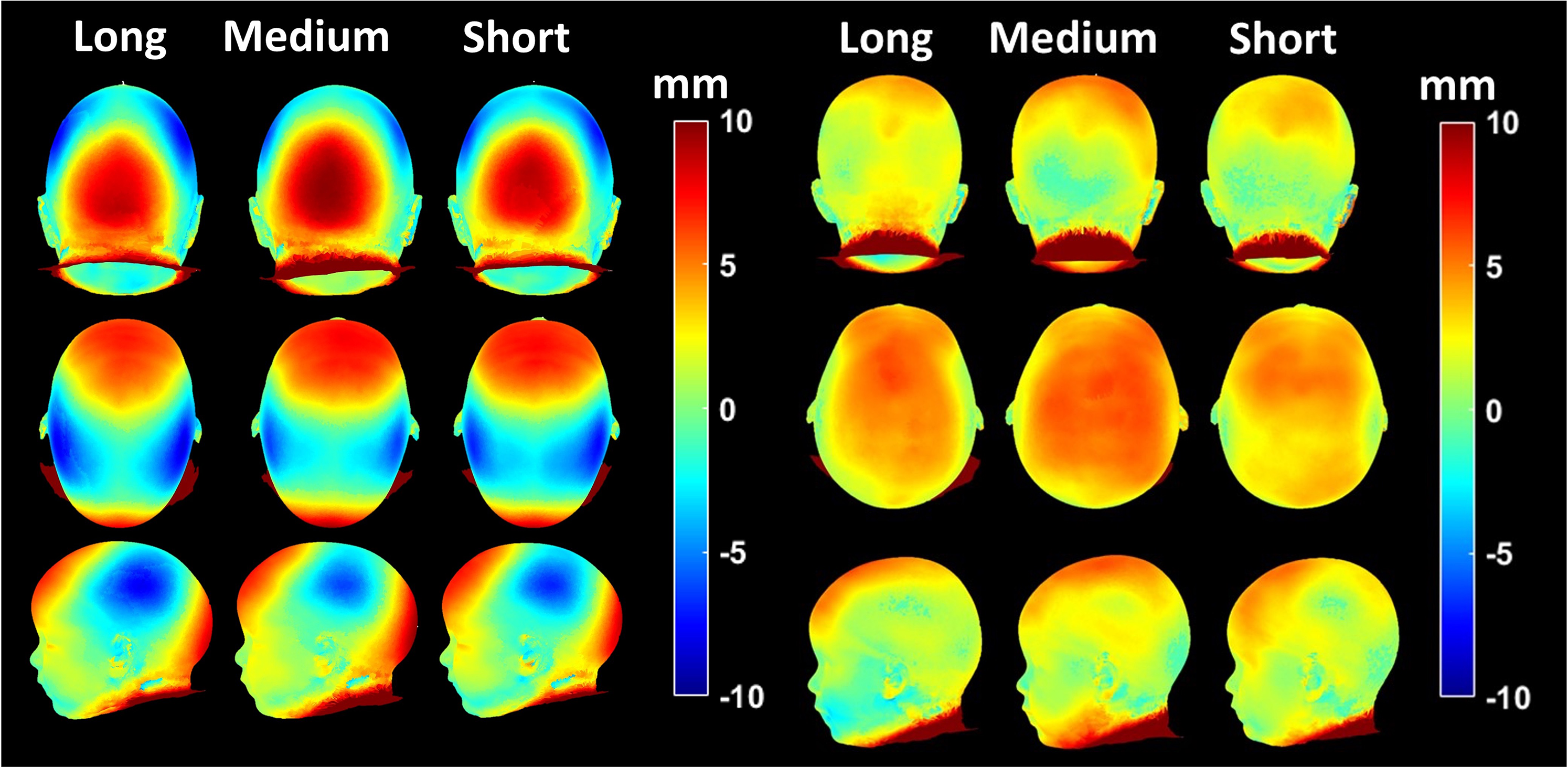
Sagittal craniosynostosis long, medium, and short barrel-stave pre-operative (left) and post-operative (right) composite heat maps. Warm colors represent areas of bossing, and cool colors represent areas of recession compared to controls.
Discussion
The treatment of sagittal craniosynostosis with strip craniectomy has undergone multiple variations since the initial descriptions by Jimenez and Barone and is commonly paired with post-operative helmet orthosis or springs.2,12,28 The addition of wedge or “barrel-stave” osteotomies by Jimenez and Barone included the use of blunt dissection of the dura and osteotomies with bone scissors from the lateral edge of the craniectomy towards the squamosal suture behind the coronal sutures and anterior to the lambdoid sutures. 2
Increasing the length of these osteotomies requires more extensive dissection toward the squamosal suture, potentially increasing the risk of injury. Our analysis identified significantly higher operative times due to the increased dissection time required. The longer barrel-stave length was also found to increase operative blood loss. Additionally, these patients had a significantly longer stay in the hospital. Therefore, increasing the barrel-stave length increases the risk of intra-operative bleeding, longer operative times, and longer post-operative hospital spending.
Currently, the length of the barrel-staves osteotomies varies widely in the literature.3–20 Regardless of the length, successful results have been reported, putting into question the benefit of extended osteotomies. The post-operative cranial index for studies utilizing the same barrel-stave pattern as ours ranges from 71.4 to 81.1.2–11 Our findings in all three groups were consistent with these findings, ranging from 78.0 to 82.3, indicating normalization of scaphocephalic head shape. While all groups had normalized post-operatively, the long-barrel stave group had the least correction of the width-to-length ratio.
While the cranial index has historically been the most frequently utilized outcome measure, multiple studies have addressed its limitations.23–25,29–31 Bins et al. have developed the scaphocephalic, frontal bossing, occipital bullet, and vertex narrowing indices to evaluate surface morphology in sagittal craniosynostosis quantitatively.23–25 In our analysis, the index measurements post-operatively in all three groups achieved percentiles falling within the range of normal patients. Frontal bossing had the least response to surgery and remained greater than the 90th percentile of controls in all three groups. No direct intervention occurs to the frontal bone during strip craniectomy, possibly leading to residual bossing. However, improvements with remodeling have been shown to occur over time.4,27,32 In contrast, the vertex narrowing had the greatest response, and results ranged from the 30 to 50th percentiles of control patients. The long barrel-stave group had increased residual vertex narrowing. Longer osteotomies lead to the separation of the parietal bones, possibly decreasing the intrinsic transmission of forces from the frontal and occipital regions during helmet remodeling. The medium barrel staves had the greatest global improvement with the correction of scaphocephaly, occipital bulleting, and vertex narrowing.
Three-dimensional composite heat map imaging allows for a global assessment of contour changes in our cohort of patients with sagittal craniosynostosis compared to aged match controls. The convexity of the forehead and occipital region indicates frontal bossing and occipital bulleting across the pre-operative groups. Additionally, the bilateral temporal and parietal regions are concave, indicating narrowing. A similar resolution of these features was shown in the post-operative composites. These findings are consistent with our previous work by Rizvi et al., who demonstrated these features in strip craniectomy with barrel-staving. 14 The greatest improvement in frontal convexity or bossing appears in the medium barrel-stave group. This group also has the least temporal and parietal concavity or vertex narrowing of the post-operative groups. However, the vertex convexity appears to be greatest in this group, indicating increased cranial height. These findings indicate that while the medium length barrel-staves provide the greatest improvement in decreasing the cranial length and increasing width at the expense of increasing height.
The overall findings in our patient cohort showed normalized results regardless of the barrel-stave length, with strip craniectomy, calling into question the utility of these osteotomies. A limitation of our study is the absence of a cohort without barrel-stave osteotomies. In a review of sagittal craniosynostosis patients who had undergone endoscopic strip craniectomy with or without barrel staves, Wood et al. showed no improvement in outcomes with the addition of barrel staves. 3 In a study by Dlouhy et al., the authors compared outcomes between wide strip craniectomy with barrel-stave osteotomies and narrow strip craniectomy without barrel-staving. 6 They showed equivalent clinical outcomes between techniques. Further investigation is needed to evaluate if the addition of barrel-stave osteotomies is needed. Another limitation of our study is the cohort size of only fifteen patients in each osteotomy group, limiting the power of statistical analysis. Additionally, while not significantly different, baseline differences exist between groups pre-operatively which may alter outcomes. Furthermore, our outcomes are followed out to one year of age, and further changes due to remodeling and growth may occur with increased long-term follow-up.
Conclusions
Strip craniectomy with the addition of long, medium, or short barrel staves in our cohort of patients with sagittal craniosynostosis all resulted in clinically successful outcomes. The craniometric measurements and indices were normalized in all three groups post-operatively. Heat mapping showed similar improvements in global head shape in all groups. Our findings suggest that increased barrel-stave osteotomy length may not be necessary for a successful operation and would avoid more extensive dissection, potential risk, increased operative time, and hospital length of stay.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent Statements
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of the University of Texas Southwestern Medical Center (STU 032018-067), with the need for written informed consent waived.