
Abstract
Objective
The Melbourne technique for total cranial vault remodeling aims to address all aspects of scaphocephaly in sagittal craniosynostosis. These features include anterior–posterior excessive length, anteriorly displaced vertex position, frontal bossing, vertex narrowing, and occipital bulleting. This study aimed to determine the progressive cranial changes that occur following the Melbourne technique for sagittal craniosynostosis.
Design
Retrospective review of 3-dimensional images collected preoperatively and postoperatively at 3 weeks, 3 months, 1 year, and 2 years.
Setting
Tertiary care pediatric institution.
Participants
Twenty-five patients with sagittal craniosynostosis.
Interventions
The Melbourne technique for total cranial vault remodeling.
Main Outcome Measure(s)
Head circumference, cephalic index, frontal bossing index, occipital bulleting index, vertex narrowing index, and vertex-nasion-opisthocranion (VNO) angle were evaluated.
Results
The cephalic index significantly increased postoperatively (P = .04) with a subsequent relapse at 3 months followed by progressively increased growth. The frontal bossing index significantly decreased postoperatively (P = .02) with a progressive decrease. The occipital bullet index had a relative decline postoperatively with relapse at 3 months, followed by a progressive decrease. The vertex narrowing index significantly decreased postoperatively (P < .001), with a plateau and slight relapse. The VNO angle showed a relative decline over time with a significant decrease by 1 year of age (P = .002).
Conclusions
The Melbourne technique improved the cephalic index, frontal bossing, vertex narrowing, occipital bulleting, and vertex positioning at 2 years of age. Cephalic index and occipital bulleting showed slight relapse at 3 months, followed by progressive improvement over time.
Keywords
Introduction
Sagittal craniosynostosis due to premature suture fusion leads to multiple deformational features, creating the scaphocephalic phenotype.1,2 The combination of frontal bossing and occipital bulleting creates increased cranial length while a decrease in width leads to vertex narrowing and temporal pinching.3–5 Additionally, the cranial vertex is displaced anteriorly, with some patients having resultant turricephaly.6,7
While the reported incidence of papilledema in single-suture craniosynostosis remains low, preventing the development of increased intracranial pressure remains a strong indicator of surgical intervention.8,9 In sagittal craniosynostosis, the rates of increased intracranial pressure have ranged from 1.84% to 9.7% of patients. 10 However, increased rates have been shown in patients treated after one year of age. 11
The ideal surgical intervention provides resolution of all the deformational aspects of sagittal craniosynostosis while increasing intracranial volume. While previously described techniques have successfully shortened and widened the cranial vault, they do not directly address the other defining deformations.12–14 The Melbourne technique for total cranial vault remodeling described in 2008 by Greensmith et al aimed to address the entire constellation of features. 15
The technique involves an intricate pattern of osteotomies with rotation of cranial segments combined with barrel staving and out fractures designed to address all features of scaphocephaly.15,16 The initial cohort of 30 patients achieved subjective improvement with limited complications. 15 The cephalic index increased by 12.9% at an average postoperative period of 11 months. A subsequent study of 33 patients showed an 11.1% improvement in the cephalic index postoperatively. 16 Additionally, these patients exhibited a decrease in cranial length, width, and head circumference but remained significantly different from controls.
Progressive alterations occur due to growth and remodeling following total cranial vault remodeling.17–21 However, previous studies have yet to evaluate the results of cranial vault remodeling with the Melbourne technique beyond the one-year postoperative period. Implementing 3-dimensional (3D) photography allows for repeated image capture over time without radiation exposure. The purpose of this study was to utilize 3D imaging to evaluate progressive cranial changes that occurred over 2 years following the use of the Melbourne technique for sagittal craniosynostosis.
Methods
A retrospective review of patients with sagittal craniosynostosis who underwent cranial vault remodeling with the Melbourne technique was completed following institutional review board approval by the University of Texas Southwestern Medical Center. All patients presenting with sagittal craniosynostosis are offered the option of cranial vault remodeling. Strip craniectomy with helmet therapy is provided as an alternative in patients less than 5 months of age. Total cranial vault remodeling with the Melbourne technique is preferred after the age of 5 months. The ideal operative age is greater than eleven months. Intraoperative blood transfusions are considered in all patients undergoing cranial vault remodeling in an attempt to match the estimated volume of blood loss.
Three-dimensional (3D) facial photographs were acquired using a 3dMD imaging system (3dMD). Images were obtained preoperatively and postoperatively at 3 weeks, 3 months, 1 year, and 2 years. Virtual 3D-derived models were analyzed using 3dMD Vultus (3dMD). Head circumference, cephalic index, scaphocephalic index (SCI), frontal bossing index (FBI), occipital bullet index (OBI), and vertex narrowing index (VNI) were measured automatically using the 3dMD Vultus Craniometrics calculator (3dMD).22–24 Landmarks at the sellion and bilateral tragions were used to create a baseline axial plane to orient all 3D images.
Head circumference was measured at the most convex portion of the forehead and occiput on a plane parallel to the baseline axial plane (Figure 1). The cephalic index was measured as the width between the bilateral eurion, divided by the length of the head at the level of the glabella, multiplied by 100 (Figure 1A). 3 The SCI, FBI, OBI, and VNI, 4 3D measures of cranial surface morphology, were evaluated based on previously published techniques and were compared to control population cutoff points and percentiles.22–24 The control values are based on normocephalic patients with even age and sex distribution for characterization of standard head shape.22–24 The vertex-nasion-opisthocranion (VNO) angle is a measure of vertex anterior–posterior deviation 6 and was measured on sagittal view 3D images using ImageJ (Figure 1). Statistical analysis was performed to calculate mean and standard deviations, which were compared using 2-sample t tests with a P-value of <.05. A linear trend line and R2 were calculated for each measurement.
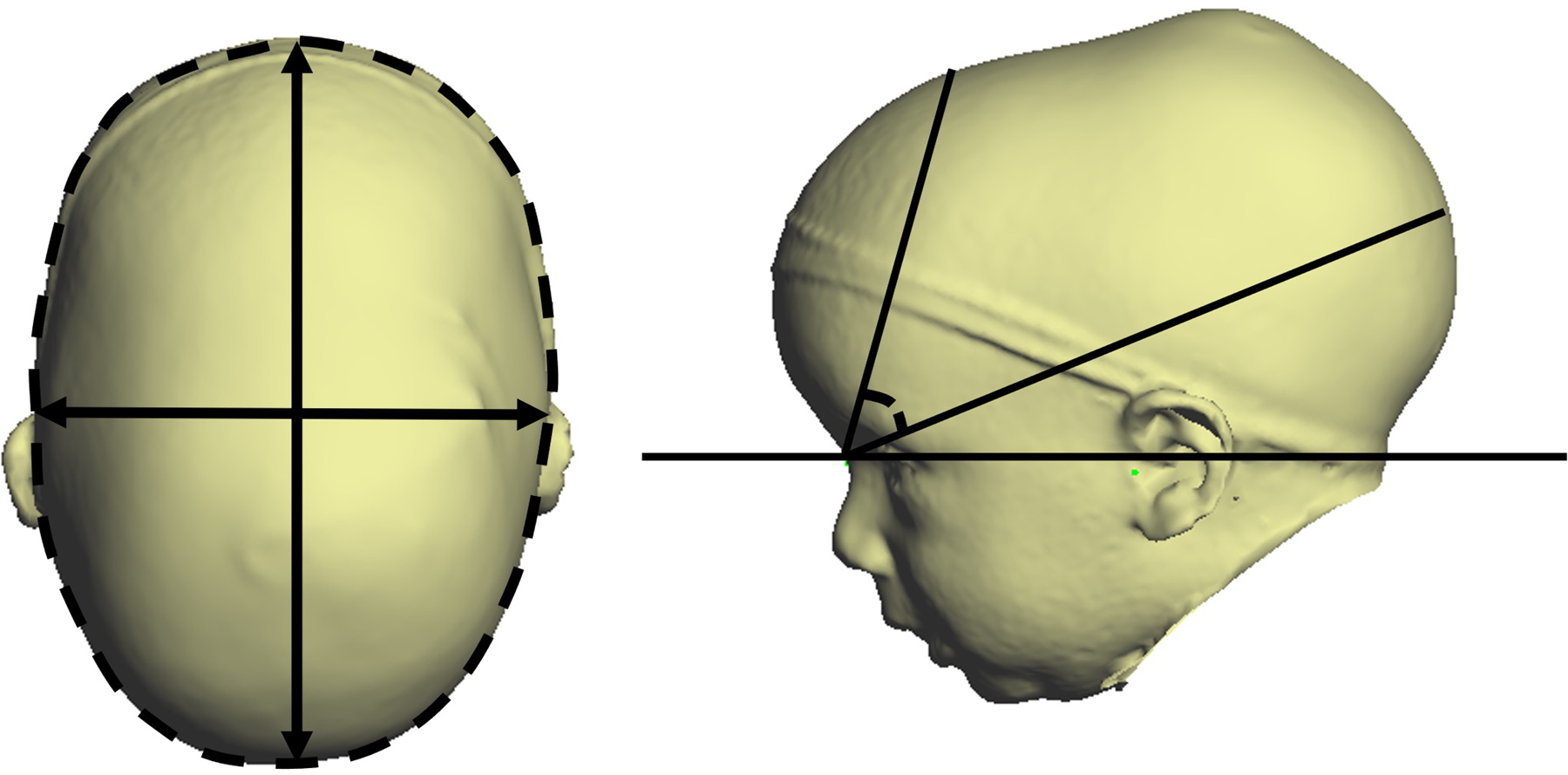
Cephalic index (left) and vertex-nasion-opisthocranion (VNO) angle (right).
Results
A total of 25 consecutive patients with sagittal craniosynostosis were included (Table 1). The patients were 80% male and 20% female. The racial and ethnic backgrounds included 72% white, 20% Hispanic, and 8% black patients. The average age at surgery was 12.7 months (range 9.13-22.35 months). Operative time averaged four and a half hours. The average blood loss was 220 cc. All patients received an intraoperative transfusion; on average, they received 195 ccs. No patients received postoperative blood transfusions. The average hospital length of stay was three and a half days postoperatively. All patients underwent ophthalmological screening pre- and postoperatively, and no patients were identified to have papilledema.
Sagittal Craniosynostosis Patient Demographics.
The average head circumference was 46.81 ± 2.02 cm preoperatively, which significantly increased at 3 weeks after surgery to 49.58 ± 2.00 cm (P < .001) (Figure 2A). Control 50th percentile head circumference for each age time point provided for comparison. 25 The circumference progressively increased and was 50.82 ± 1.57 cm at 2 years postoperatively. Preoperatively, the cephalic index was, on average, 73.36 ± 4.09 and significantly increased to 75.70 ± 3.47 at 3 weeks following surgery (P = .04) (Figure 2B). Control range for cephalic index provided for comparison. 26 At 3 months postoperatively, the cephalic index had a relative relapse to 74.83 ± 3.38 cm; however, by 2 years, the cephalic index increased to 76.30 ± 2.50. The preoperative VNO angle was 59.35 ± 3.80° indicating anterior vertex displacement. The VNO decreased over time and was significantly decreased to 55.76 ± 2.61° by 1 year postoperatively (P = .002) (Figure 2C).
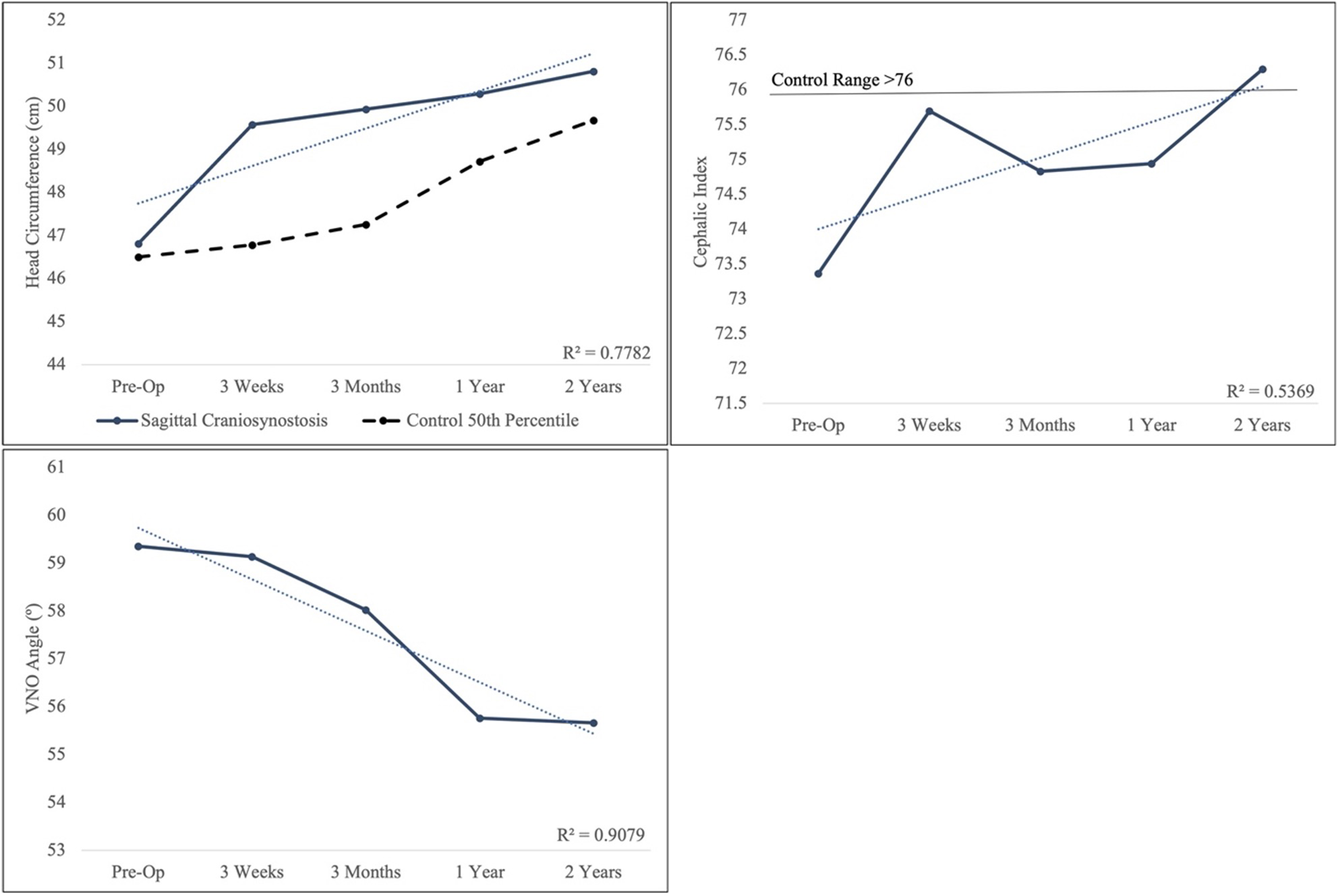
Head circumference (A), cephalic index (B), and vertex-nasion-opisthocranion (VNO) angle (C). The dotted line represents linear trend line and R2.
Before surgery, the SCI was 66.50 ± 5.27, which is >100th percentile compared to controls (Figure 3A). 23 A significant increase to 76.02 ± 4.22 was seen at 3 weeks postoperatively (P < .001). The index had a subsequent minor relapse at 3 months but rose to 77.22 ± 3.90 by 2 years following surgery, equivalent to the 99th percentile of controls. The FBI of patients before surgery was 1.01 ± 0.09, which falls into the 98th percentile of controls (Figure 3B). 23 By 3 weeks after surgery, the index significantly decreased to 0.95 ± 0.07 (P = .02). The index progressively decreased to 0.92 ± 0.08 at 2 years, equivalent to the 83rd percentile of controls. Preoperatively, the OBI was 1.16 ± 0.11, equivalent to the 87th percentile of controls (Figure 3C). 23 The index initially decreased at 3 weeks, followed by a slight relapse by 3 months. The index then progressively decreased to 1.10 ± 0.07 by 2 years, which falls in the 70th percentile of controls. The VNI was 1.44 ± 0.14, which is in the 97th percentile of controls (Figure 3D). 23 The index significantly increased to 1.58 ± 0.10 by 3 weeks after surgery (P < .001). This was followed by a relative plateau and a minor relapse ending at 1.56 ± 0.11 by 2 years, falling in the 86th percentile of controls.
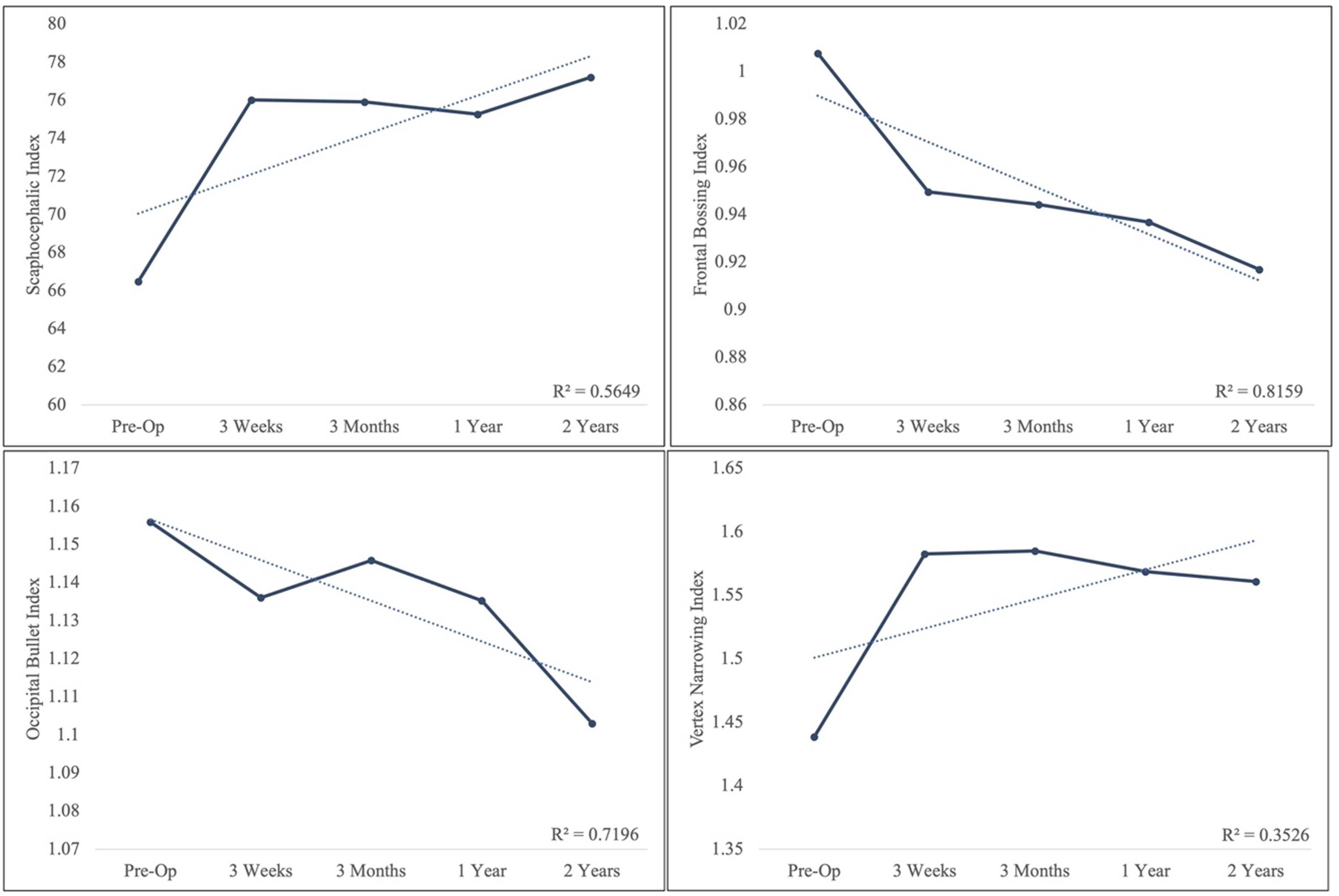
Scaphocephalic index (A), frontal bossing index (B), occipital bullet index (C), and vertex narrowing index (D). The dotted line represents linear trend line and R2.
Discussion
Various techniques have been implemented for the treatment of scaphocephaly. Strip craniectomy procedures remove a strip of bone at the involved suture. Postoperatively, the cranial form is remodeled using springs or a molding helmet. The benefit of this technique includes positive outcomes with decreased blood loss, operative time, and length of hospital stay.27–31 These procedures, however, require rapid postoperative cranial remodeling and growth and thus are only effective in early infancy. 32 Patients commonly present outside of this critical window and are not candidates for this procedure.
Other craniectomy techniques, such as the pi pattern, immediately decrease cranial length while simultaneously performing vertex widening.33–40 However, the technique typically does not directly address frontal bossing or occipital bulleting. Alternatively, cranial remodeling techniques using springs or distraction have been developed.41–52 These devices allow for a more gradual correction but require a secondary operation for hardware removal.
While many techniques for scaphocephaly aim to increase cranial width while decreasing length, the Melbourne craniofacial unit described an alternative technique that additionally addresses the anteriorly displaced vertex, frontal bossing, and bulleting of the occiput typically seen in sagittal craniosynostosis.15,16 Additionally, the posterior movement of the vertex and widening of the parietal bone flaps allow for significant intracranial volume expansion, decreasing the risk of ICP elevation.15,16
In this technique, the frontal bone segment is remodeled with barrel staving and rotation of the segment before replacement. 15 This cohort showed a significant decrease in frontal bossing following surgery, which progressively improved until 2 years of age. At 2 years of age, the FBI was within the 83rd percentile of control patients. 23 Yen et al modified the pi procedure with the addition of frontal craniotomy and demonstrated the benefits of direct intervention for frontal bossing. 18 There were improvements in anterior prominence of the forehead, bossing angle, and horizontal bossing ratio in those who received frontal craniectomy. Direct frontal remodeling has also been shown to have benefits as an adjunct to the H craniectomy and total cranial vault remodeling techniques.53,54 In contrast, others have argued that direct frontal intervention is not required as spontaneous remodeling occurs following intervention isolated to the middle and posterior cranial vault.17,21,31,55 This variation is likely due to the age of the patients undergoing reconstruction and the intrinsic ability to remodel with growth.
In the Melbourne technique, the occipital bulleting deformity is addressed directly with removal and barrel staving, followed by superior and anterior translation. 15 A bandeau is taken from behind the anterior fontanelle, rotated 180°, and flipped 90° to form the new occiput. 15 The bandeau commonly encompasses the location of the vertex. The combination of steps, in turn, eliminates the anteriorly displaced vertex and creates a posterior vertex. Our findings demonstrate these changes with a decreased OBI and VNO angle. The occipital bulleting did undergo a slight relapse at 3 months of age, followed by a progressive decrease up until 2 years of age. In contrast, the VNO angle experienced a more gradual reduction over time, with a plateau at 1 year of age. Hopper et al's modifications of the pi procedure with a low occipital osteotomy with verticalization demonstrated the benefit of direct occipital intervention by resolving bulleting by 2 years of age. 56
Parietal constriction leading to vertex narrowing has been shown to worsen with increasing patient age. 57 To address the vertex narrowing, bilateral parietal bone flaps are removed, rotated 180°, and flipped to the contralateral side. 15 These alterations lead to the expansion of the cranial vertex width. The VNI reflected these changes with a significant increase postoperatively. Toma et al, utilizing the Melbourne technique, had previously reported an increase in cranial width by 13.2% at 8.9 months following surgery. 16 While our study had similar findings, there was a gradual relapse in width, ending in the 86th percentile of controls at the 2-year postoperative period.
The increased cranial length in scaphocephaly is corrected by the combination of frontal and occipital barrel staving and repositioning in the Melbourne technique. In addition, the rotation and flip of the parietal bone flaps expand the cranial width. The decreased length and increased width lead to improvements in the cephalic index. Despite the limitations of the cephalic index, it remains the most widely evaluated metric.4,6,7,58 In our study, the cephalic index significantly increased postoperatively, followed by a relapse, but was 76.3 on average at 2 years postoperatively. The SCI additionally reflected these changes with a significant increase postoperatively, with the greatest improvement seen at 2 years postoperatively. The early relapse in values is possibly due to postoperative soft tissue swelling and edema that later self-corrected, negating the need for additional interventions.
The tendency for relapse in the cephalic index over time has previously been reported.13,19,59 Galiay et al evaluated 8 different techniques and found relapse over time despite the intervention. 13 Greensmith et al, in their retrospective review of 17 patients following the Melbourne technique, saw a 12.9% cephalic index increase from 64.6 to 77.5 at 11 months postoperatively. 15 In a follow-up study of 33 patients by Toma et al, the cranial index was shown to improve by 11.1% with no significant difference from controls postoperatively. 16
Modifications to the Melbourne technique have also been reported to reduce the number of craniectomies and to decrease blood loss.60–62 The average estimated blood loss with the Melbourne technique was between 445 and 460 cc (range, 200-850), which was higher than our average estimated blood loss of 220 cc.15,16 However, visual estimation is an unreliable method for evaluating intraoperative blood loss, possibly leading to variation between centers.63,64
A limitation of 3-dimensional photography is the inability to measure intracranial volume accurately. Intracranial volume is essential for understanding the ability for cranial expansion and the prevention of increased ICP. While no patients in the current study had signs of increased ICP on ophthalmologic examination and no patients required revision surgery, the changes in intracranial volume should be further investigated. The study's power is limited by the size of the patient cohort, and future studies should include larger cohorts to support these findings. Additionally, these patients will continue to grow and should be followed for morphological evaluation at skeletal maturity.
Conclusions
This study identifies significant progressive, long-term improvement in cranial morphology after performing the Melbourne technique for cranial vault remodeling in patients with sagittal craniosynostosis. The SCI significantly increased due to direct frontal and occipital remodeling. The FBI significantly decreased from the frontal remodeling. The OBI also showed a decrease from occipital remodeling. The parietal bone flap remodeling demonstrated a significant widening of the vertex. The reduction in cranial length and increased width significantly increased the cephalic index. The remodeling of the occiput with a bandeau significantly decreased the VNO angle due to the posterior displacement of the vertex.
Footnotes
Authors’ Note
Ethical Approval and Informed Consent Statements: The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of the University of Texas Southwestern Medical Center (STU 032018-067), with the need for written informed consent waived.
Authors’ Contribution
LMH and PSM involved in project design. LMH, KP, and RRH were involved in data collection. LMH, KP, RRH, AAK, and PSM were involved in data analysis and writing and preparation of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.