
Abstract
Objective
Strip craniectomy (SC) and fronto-orbital advancement (FOA) are 2 techniques for the management of unilateral coronal synostosis (UCS) that differ in timing and approach. However, the tempo and extent of postoperative changes in craniofacial features are less well understood. The purpose of this study is to evaluate the progression of craniofacial symmetry over time following SC or FOA in UCS.
Design
A retrospective review of 3-dimensional images obtained preoperatively and at 1- and 2-year postoperatively.
Setting
Tertiary pediatric institution.
Patients, Participants
Thirty-six patients with UCS and 36 control patients.
Interventions
Strip craniectomy with helmet or FOA.
Main Outcome Measure(s)
Three-dimensional craniometric asymmetry measurements.
Results
The SC group had significantly shorter operative time, less blood loss, and a shorter hospital length of stay. All craniofacial symmetry measurements significantly improved postoperatively in both groups (P < .05), except for orbital width asymmetry in the FOA group at both 1 year and 2 years postoperatively (93.63 ± 3.53%; 93.60 ± 7.41%). There was no significant difference in craniofacial asymmetry measurements between groups. The orbital width (95.15 ± 3.95%) and midface (96.12 ± 3.15%) asymmetry in the SC group remained significantly different from controls at 2 years postoperatively (P < .001; P < .001). The cranial asymmetry (96.43 ± 2.63%), orbital width asymmetry (93.60 ± 7.41%), and midface asymmetry (96.53 ± 1.61%) in the FOA group remained significantly different from controls at 2 years postoperatively (P = .009; P = .042; P = .015).
Conclusions
Strip craniectomy and FOA both improved craniofacial symmetry over time, though orbital width and midface differences persisted compared to controls at 2 years postoperatively. Fronto-orbital advancement also showed a persistent cranial asymmetry compared with controls.
Introduction
Several surgical techniques have been developed to address the craniofacial asymmetry associated with unilateral coronal synostosis (UCS).1,2 Traditional open cranial vault techniques, such as fronto-orbital advancement (FOA), involve the removal of the frontal bone and supraorbital bandeau, followed by direct reshaping and forward repositioning of the frontal bone.1–3 More recently, alternatives have been developed, such as strip craniectomy (SC), which involves releasing the fused coronal suture, with subsequent cranial remodeling guided by postoperative helmet therapy or, less commonly, distraction or springs.1,2,4–7
Fronto-orbital advancement and SC differ in timing, extent of osteotomies, and approach to correction.1,2 Fronto-orbital advancement is typically performed later in infancy, between 8 and 10 months of age, and provides immediate correction of orbital and frontal asymmetry. 8 In contrast, SC is generally performed in early infancy, around 3 months of age, and relies on the rapid cranial growth and postoperative helmeting to achieve gradual remodeling. 9 Due to its open approach and extent of osteotomies, FOA results in greater blood loss, longer operative times, and longer hospital admissions.2,10,11 While SC relies on compliance with postoperative helmet therapy. Furthermore, SC is associated with improved ophthalmologic outcomes and decreased need for strabismus surgery.2,12–14
Despite the use of both FOA and SC for correcting UCS, there is limited data directly comparing postoperative morphological outcomes between these techniques. Most existing studies focus on perioperative outcomes rather than on quantitative assessments of craniofacial symmetry and contour restoration over time.1,2 As a result, the tempo and extent of craniofacial symmetry achieved with SC versus FOA remain poorly characterized. The purpose of this study is to assess comprehensive craniofacial symmetry progression in patients with UCS following either SC or FOA, providing evidence to inform surgical decision-making and improve patient and family education and counseling.
Methods
A retrospective review was conducted of patients diagnosed with UCS who underwent either SC with helmet therapy or bilateral FOA, following approval by the University of Texas Southwestern Medical Center Institutional Review Board. Diagnoses were confirmed preoperatively with computed tomography scans. Patients with syndromic diagnoses, additional suture involvement, or other craniofacial anomalies were excluded. At our institution, infants with UCS presenting before 6 months of age are offered either SC or FOA, while those presenting later are offered FOA. All patients who underwent SC received postoperative helmet therapy for 23 h/d, beginning within 1 week after surgery and continuing for 1 year. All included patients reported compliance with the full protocol, each having between 2 and 3 helmets throughout the course. Individual age-matched control subjects were identified at each time point, with separate control groups created for the SC and FOA groups. Demographics and perioperative factors were compared between SC and FOA.
Three-dimensional craniofacial photographs were obtained and analyzed using the 3dMD imaging system (3dMD) as previously described by our group in patients with UCS (Figure 1). 15 Cranial asymmetry was defined as a vector analysis ratio of distances measured 30° from the midline. Brow projection asymmetry was defined as the angle between the Frankfort horizontal and a line intersecting the inferior orbit and supraorbital rim. Orbital vertical asymmetry was defined as the angle between a horizontal line and a line connecting the midpoints of the supraorbital rims. Linear measurements included orbital width (medial-lateral) and orbital height (inferior-superior) of the ocular aperture. Midface asymmetry was assessed from tragion to subnasale, while nasal and chin deviation were measured as the angle between these structures and the vertical midline. Frontal radial composites were generated with vector analysis landmarks placed at 15° intervals across half of the calvarium anterior to the bilateral tragus along with the frontal bar. Average head composites were created for UCS patients preoperatively and at all postoperative time points. All patients with right-sided UCS were mirrored so that all patients had left UCS for composite creation.
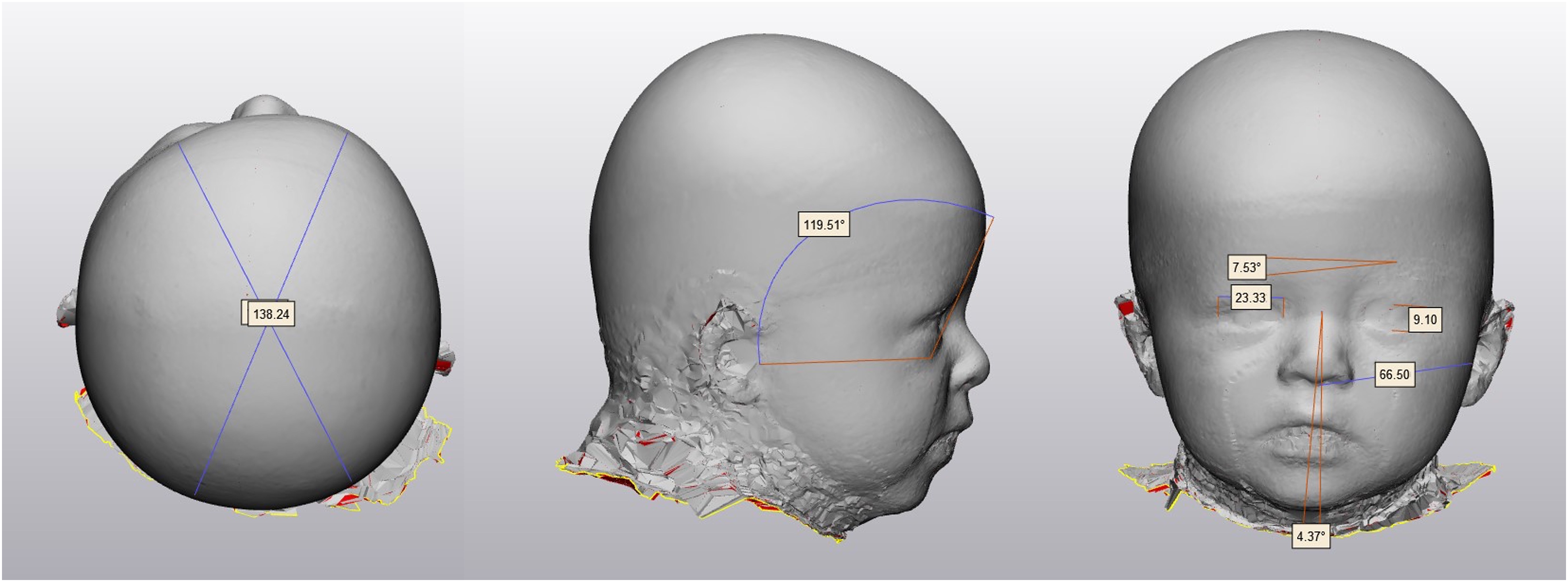
Unilateral coronal craniosynostosis craniometric measurements: cranial asymmetry index (left), brow projection asymmetry (middle), orbital width asymmetry, orbital height asymmetry, orbital vertical asymmetry, midface asymmetry, nasal deviation (right).
All measurements were performed in duplicate by 2 authors and assessed for inter- and intraobserver reliability using Cohen's Kappa analysis with strong reliability (k = 0.83; k = 0.84). Statistical analyses were conducted with SPSS version 29 (IBM Corp). Facial symmetry was assessed by comparing affected and unaffected sides using paired-sample t tests. Pre- and postoperative measurements were compared using paired-samples t tests, and comparisons between surgical groups and controls were conducted using 2-sample t tests. Statistical significance was defined as P < .05. To account for multiple comparisons, a Bonferroni correction was applied, with statistical significance determined using an overall α level of .05.
Fronto-Orbital Advancement
A bicoronal zigzag incision was made, and a flap was elevated in the subgaleal plane to approximately 2 cm above the orbital rims, then transitioned to the subperiosteal plane and extended to the fronto-zygomatic sutures bilaterally. The superior orbital rims were degloved to the fronto-nasal suture, and the fronto-zygomatic sutures were exposed. The bifrontal bone was outlined and removed. The bilateral superior orbital rim was removed as a bandeau with a lateral tongue-and-groove pattern. A spanning resorbable plate with lateral, medial, and cephalic extensions was secured to the bandeau with resorbable plates to facilitate lateral fixation. Closing wedge osteotomies were performed at points of maximal curvature to achieve symmetric contouring. The bandeau was molded to match the contralateral side and fixated medially and laterally with resorbable plates. The bifrontal bone was split along with the midline, mirrored, and contoured to the bandeau using relaxing kerfs and Tessier bone benders, then fixated with resorbable plates. Bone grafts were placed to fill residual gaps. No intervention involving the nasal bones was performed. The temporalis muscles were resuspended, the scalp was redraped, and the scalp was closed in a layered fashion.
Strip Craniectomy
A limited 4-cm incision was planned along with the affected coronal suture. The incision was made and carried through the galea, which was elevated in the midline from the anterior fontanelle to near the lateral orbital rim overlying the fused suture. The periosteum was then elevated to provide exposure. Epidural access was obtained just below the incision through 2 small holes created with a high-speed bur, and the intervening bone was removed. A 1-cm strip of bone was excised along with the length of the fused coronal suture. As dissection progressed along with the suture toward the skull base, a portion of the lesser wing of the sphenoid was removed near the orbit with care to avoid orbital violation. Bone removal extended from the anterior fontanelle to the skull base along with the coronal suture. The incision was then closed in a layered fashion.
Results
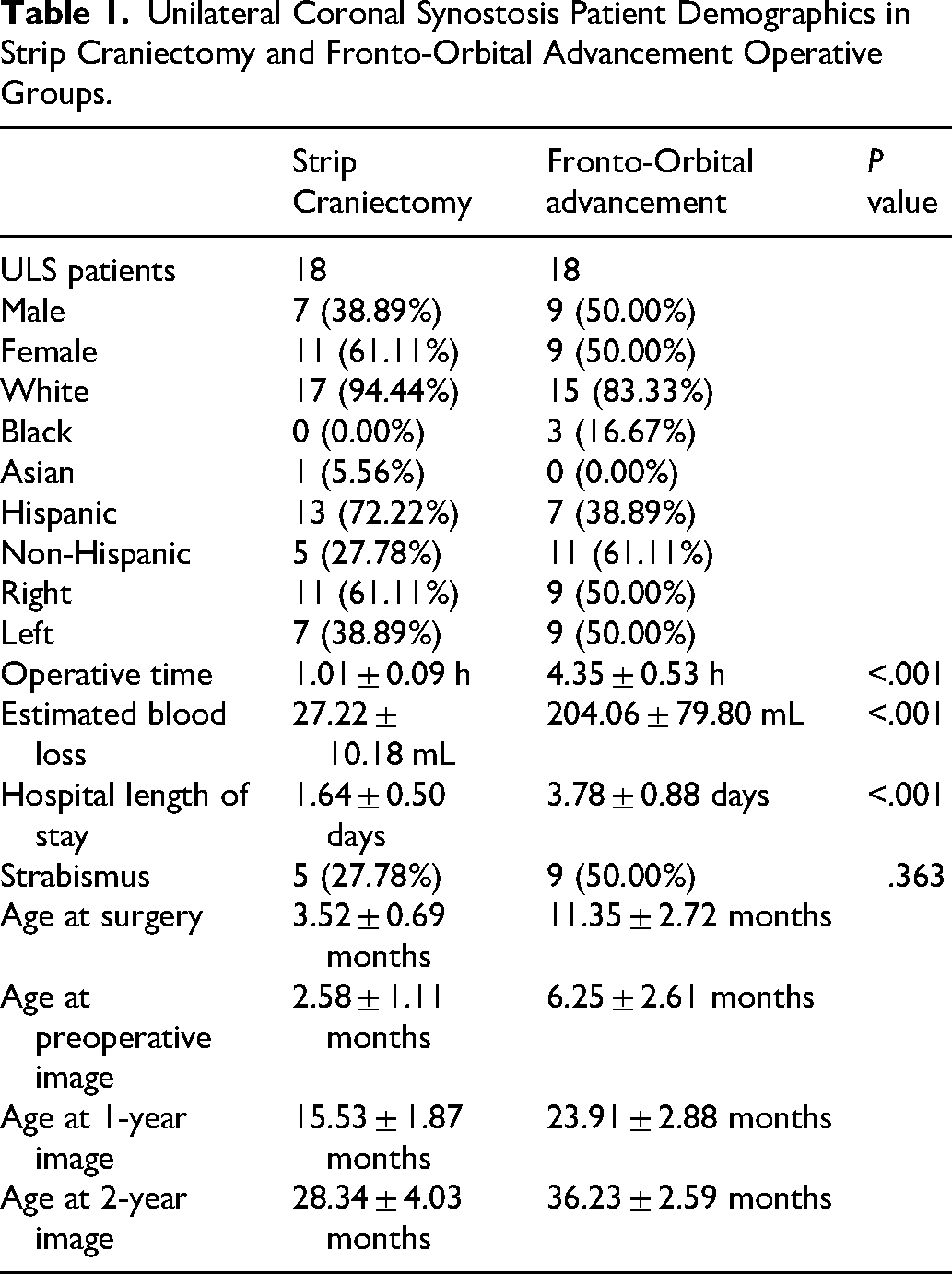
A total of 36 patients (18 SC, 18 FOA) were evaluated (Table 1). Demographics were similar, though the SC group had a higher proportion of Hispanics (72.2% vs 38.9%), and FOA included more Black patients (16.7% vs 0.00%). Strip craniectomy was performed at a younger age (3.5 vs 11.4 months) with significantly shorter operative time, lower blood loss, and shorter hospital length of stay (P < .001). No patients underwent a revision operation within 2 years following surgery. Strabismus was more frequent after FOA than after SC (50.0% vs 27.8%) within 2 years following surgery, but underpowered to determine significance. A sample size of 150 patients would be required for statistical significance with adequate power. Craniofacial composites of each surgical technique preoperatively, 1 year, and 2 years postoperatively show global changes (Figure 2). Forehead, orbit, nasal, and chin asymmetries demonstrate visible changes over time. Frontal radial composites of the forehead show the improvement in forehead symmetry that occurred across time points (Figure 3).
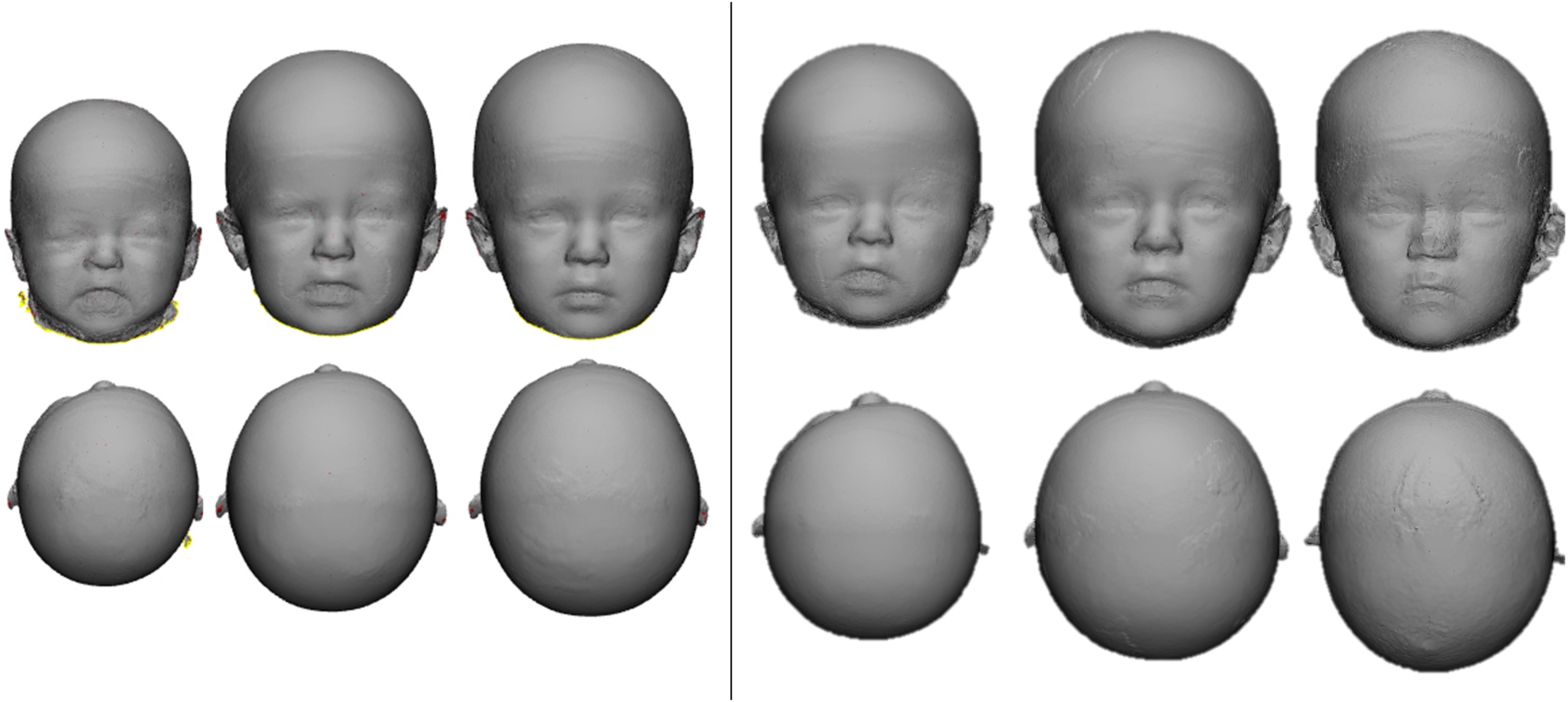
Unilateral coronal synostosis patient preoperative, and 1-year and 2-year postoperative composites in strip craniectomy (left) and fronto-orbital advancement (right) operative groups.
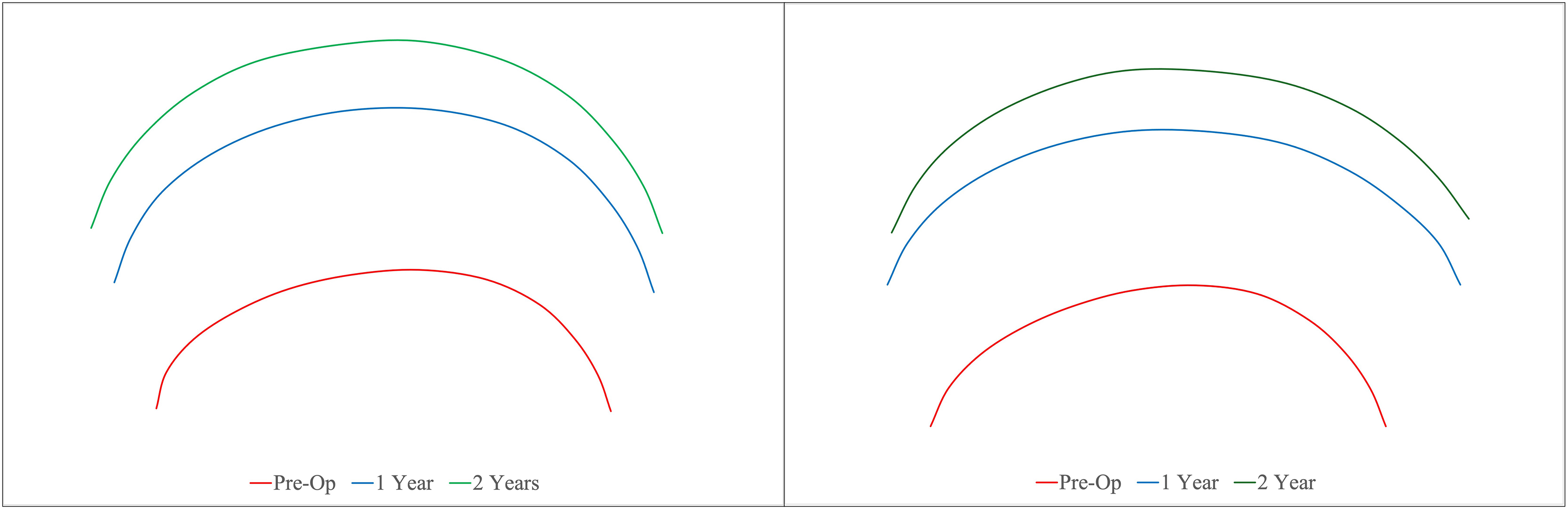
Unilateral coronal synostosis patient preoperative (red), and 1-year (blue) and 2-year (green) postoperative frontal radial composites in strip craniectomy (left) and fronto-orbital advancement (right) operative groups.
Unilateral Coronal Synostosis Patient Demographics in Strip Craniectomy and Fronto-Orbital Advancement Operative Groups.
Strip craniectomy and FOA patients demonstrated significant preoperative craniofacial asymmetry across all measurements (Table 2). By 1 year, both groups showed substantial improvement in cranial, brow, orbital, midface, nasal, and chin symmetry, with most parameters significantly improved from baseline. Changes were largely maintained or further improved at 2 years postoperatively. No statistically significant differences were observed between the 2 surgical groups at any postoperative time point. While cranial symmetry trended toward normal in the SC group at 2 years (98.7% vs 96.4%, P = .052), this did not reach significance. Similarly, orbital vertical asymmetry and chin deviation showed borderline differences but remained nonsignificant. Both surgical techniques achieved comparable long-term correction of craniofacial symmetry, with the greatest improvements occurring within the first postoperative year.
Craniofacial Asymmetry Comparison of Strip Craniectomy and Fronto-Orbital Advancement Operative Groups.
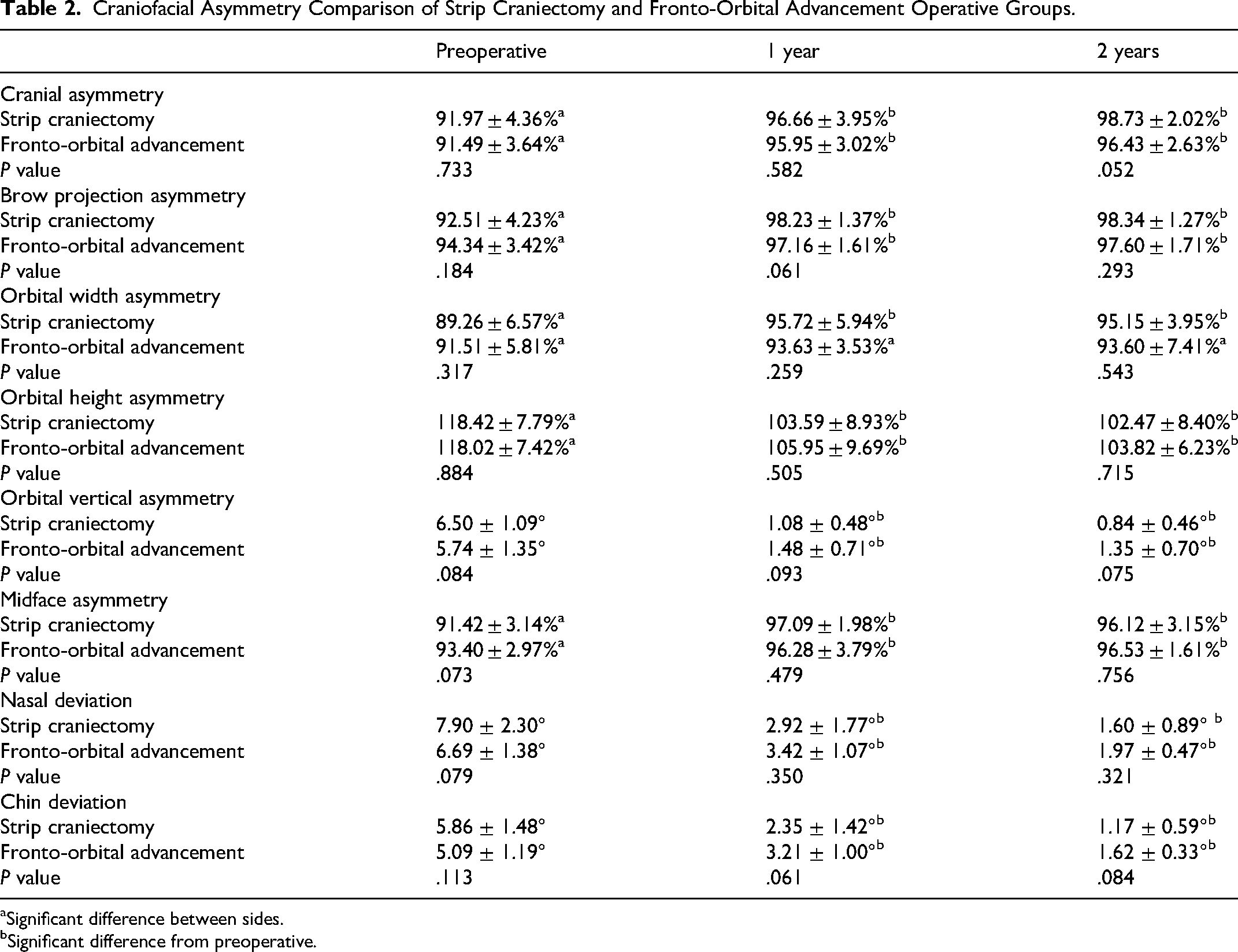
Significant difference between sides.
Significant difference from preoperative.
Preoperatively, patients undergoing SC demonstrated significant craniofacial asymmetry compared with controls across all measures (P < .001) (Table 3). By 1 year, SC patients showed marked improvement, with many parameters approaching control levels. However, significant differences persisted in orbital width asymmetry, midface asymmetry, and nasal and chin deviation (P < .01). At 2 years, cranial, brow, orbital height, and orbital vertical asymmetry in the SC group were no longer significantly different from controls. In contrast, orbital width and midface asymmetry remained significantly worse than controls (P < .001), while nasal and chin deviation differences resolved.
Craniofacial Asymmetry Comparison of Strip Craniectomy and Fronto-Orbital Advancement and Control Groups.
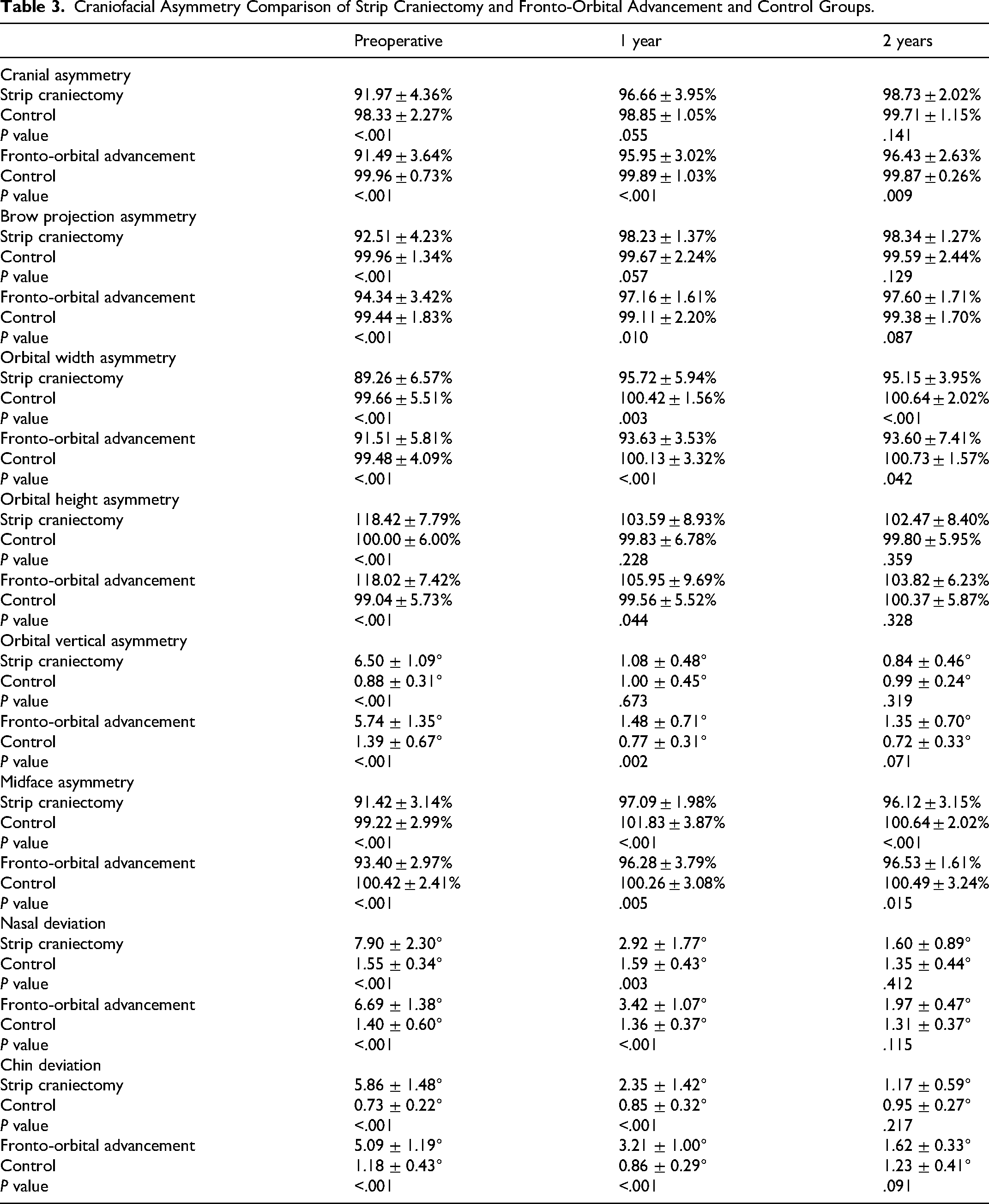
Fronto-orbital advancement patients demonstrated significant craniofacial asymmetry compared with controls preoperatively across all parameters (P < .001) (Table 3). At 1 year, FOA resulted in substantial improvements, but differences persisted relative to controls in cranial asymmetry, brow projection, orbital width, orbital height, orbital vertical asymmetry, midface asymmetry, nasal deviation, and chin deviation. By 2 years, FOA patients continued to show significant improvement from baseline, with several measures, such as cranial asymmetry, orbital width, orbital height, and midface asymmetry, remaining significantly different from those of controls. In contrast, brow projection, orbital vertical asymmetry, nasal deviation, and chin deviation were no longer statistically different.
Discussion
Unilateral coronal synostosis results in asymmetric growth and a complex craniofacial deformity.1,2 The cascade of dysmorphology in UCS is believed to originate from the cranial vault, progressing to the skull base, and finally to the facial structures.16–18 The result presents a reconstructive challenge, characterized by forehead and brow recession, a multifaceted orbital malformation, and midfacial hypoplasia, accompanied by nasal and chin deviation.19,20 The condition not only affects cranial morphology but also has potential implications for neurodevelopment, vision, and psychosocial well-being.19,20 The primary goal of surgical correction remains restoring cranial and brow symmetry, expanding the intracranial space, and optimizing aesthetic outcomes.
Fronto-orbital advancement has been the traditional and widely utilized surgical approach for correcting the craniofacial asymmetry associated with UCS.8,9,21 Fronto-orbital advancement provides direct correction through reshaping of the frontal bone and supraorbital bandeau with advancement on the affected side to address the cranial vault and orbital deformities. 3 However, FOA has been associated with inadequate correction of orbital dysmorphology and relapse in the frontal bone and supraorbital shape.22–27 The underlying causes of these irregularities have not been definitively established. However, FOA relies on the union of 2 surgically devascularized segments, the repositioned frontal bones, and the bandeau itself. It is therefore not unexpected that the interface between these devascularized segments may exhibit impaired growth or contour irregularities, a phenomenon observed by many surgeons.22–27
More recently, techniques with less extensive osteotomies, such as SC, have emerged as alternatives to traditional FOA for the treatment of UCS.1,2,4–7 Strip craniectomy involves suture release through small incisions, typically performed in early infancy, followed by passive or active molding with helmeting, springs, or distraction devices.1,2 At our institution, we utilize postoperative cranial molding helmet therapy to guide skull growth and symmetry. The SC technique requires shorter operative time and results in less blood loss and lower transfusion requirements than FOA.2,10,11 Patients typically spend less time in the hospital and are less likely to develop strabismus requiring extraocular muscle surgery.2,10–14
Strip craniectomy is becoming increasingly offered by craniofacial surgeons, with only 3.5% offering SC in UCS in 2019 compared to 50.0% in 2025.8,21 However, many surgeons have reported that a lack of evidence is the greatest obstacle to clinical decision-making in UCS. 8 While these perioperative benefits of SC in UCS have been well demonstrated, the comparison of the progression of craniofacial symmetry following SC and FOA has been less well defined.1,2 We performed a comprehensive morphological comparison between techniques over the first 2 years following surgery and with age-matched controls.
In both techniques, the preoperative asymmetry of the cranial vault improved significantly following surgery. In line with our findings, Varagur et al found no significant difference in forehead volume asymmetry between FOA and SC in school-age children with UCS. 28 The correction in symmetry achieved following FOA remained stable through 2 years postoperatively. However, at both time points, the cranial vault remained significantly more asymmetric than in age-matched controls. Multiple factors likely impact cranial vault symmetry, including technical variations and segment positioning, as well as intrinsic changes in cranial growth following frontal bone devascularization. The lack of growth following FOA can lead to a relapse of the flattened forehead appearance.22–24 The relapse following FOA has led some surgeons to perform overcorrection to attempt to mitigate these effects.29,30 Routine overcorrection was not used in our approach and remains controversial, as excessive advancement may result in persistent frontal over projection, fronto-bandeau contour mismatch, or abnormal orbital projection, particularly given the variability of craniofacial growth following surgery. Additionally, the asymmetry of the forehead is significantly associated with both parent and physician-reported desire for revision surgery, with reported reoperation rates ranging between 10.8% and 46.9% following FOA in UCS.1,24,28,31,32
In contrast to the FOA cohort, the cranial symmetry in SC continued to improve over time, even after the completion of helmet therapy, and was not statistically significantly different from controls. While Elawadly et al demonstrated continued improvements in cranial symmetry at 6 months following SC, our study demonstrates continued improvement in cranial symmetry even after helmet therapy has been completed. 33 These findings suggest a maintained ability for growth and remodeling following SC. Compared to FOA, SC is performed at an earlier age and thus has greater growth potential, potentially leading to variation in cranial symmetry between the 2 interventions.
The complexity of the orbital malformation in UCS results from elevation of the affected-sided lesser sphenoid wing, leading to elevation, retrusion, and rotation of the supraorbital rim.25,34 The brow projection symmetry significantly improved following both SC and FOA. At 2 years following surgery, both groups had brow projection symmetry that was not significantly different from that of controls. Our findings align with those of Tan et al, who found no difference in supraorbital projection symmetry between FOA and SC in 22 patients with UCS at approximately 3 to 4 years postoperatively. 35
The resulting orbital aperture on the affected side is increased in height and narrowed compared to the patients’ contralateral side, and to the ipsilateral side in controls, before surgical intervention. The orbital height decreased significantly following both surgical techniques and returned to similar levels to those of the controls at 2 years postoperatively. The orbital width significantly improved following SC but remained significantly different from controls. Following FOA, significant improvements in orbital width were not observed, and it also remained significantly different from the controls. An early release following SC may allow for more opportunity for remodeling, owing to the orbit widening. However, both techniques remain insufficient in normalizing the orbital width by 2 years postoperatively. The lack of sufficient improvement may be due to orbital alterations being linked to subcranial alterations that are not directly affected by these techniques and may have more limited remodeling and growth capacity. In our experience, the residual difference in orbital width is relatively mild clinically and not indicated for revision. Our findings are consistent with the study by Domeshek et al, who looked at the orbital index, a ratio of height and width, at 1 year following either FOA or SC and found similar improvements between techniques, but the asymmetry did not completely resolve. 36
The alterations in the cranial base are believed to be a result of the coronal suture fusion and can lead to subcranial alterations in the middle and lower face.16–18 Midface deficiency was observed on the affected side, and residual asymmetry persisted following both surgical techniques. The alteration in the maxilla is also shown through the nasal deviation, and the chin deviation demonstrates further mandibular deviation. Fronto-orbital advancement and SC both significantly reduced nasal and chin deviation, but these effects were not normalized compared to controls until 2 years postoperatively. These findings suggest that subcranial alterations may have a more limited remodeling capacity than upper facial and cranial deformities. Persistent midfacial asymmetry in UCS following FOA has been well recognized and attributed to zygomatic and maxillary deficiency.29,37–42 Varagur et al also found no significant difference between FOA and SC in midfacial asymmetry or nasal deviation in school-age children with UCS. 28 In contrast, Tan et al showed significant improvements in asymmetry in middle facial depth and nasal deviation following SC compared to FOA. 33
This study has several limitations. Although postoperative outcomes were evaluated through 2 years, longer-term follow-up is necessary to assess craniofacial growth and remodeling through skeletal maturity. While 3-dimensional imaging allows for serial assessments without radiation exposure, it does not accurately capture intracranial morphology or volumetric changes. Helmet compliance data were also based on caregiver reporting, which may introduce bias. Additionally, to achieve adequate power, future large multicenter studies should be conducted, as the current study is at risk of Type II errors. Finally, the outcomes reflect institutional approaches for SC and FOA, and variations in surgical technique among other surgeons may affect their findings.
Conclusion
Overall, patients undergoing either SC or FOA exhibited significant preoperative craniofacial asymmetry compared with controls across all parameters. By 1 year postoperatively, both surgical groups demonstrated marked improvement, with many measures approaching control values. However, subtle differences persisted, and outcomes diverged by 2 years. Strip craniectomy patients achieved near-control morphology in most features, though orbital width and midface asymmetry remained distinct. Fronto-orbital advancement patients likewise showed sustained improvement but continued to differ significantly from controls in cranial asymmetry, orbital width, and midface symmetry. These findings suggest that both SC and FOA can achieve substantial correction of deformity; however, the extent of remodeling differs between the 2 techniques. Recognition of these differences is critical for surgical planning, counseling families on expected outcomes, and refining long-term management strategies for patients with unilateral coronal craniosynostosis.
Footnotes
Ethical Approval and Informed Consent Statement
Institutional review board approval was granted for the current study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.