
Abstract
Objective
Unilateral lambdoid synostosis (ULS) is characterized by posterior plagiocephaly with a complex cranial and facial asymmetry. The occipital switch (OS) technique is commonly used to correct the posterior vault deformity, while the occipital neo-bandeau (ON) has been proposed as an adjunct to improve cranial vault proportions. The purpose of this study was to compare post-operative differences in craniofacial morphology between OS and OS + ON in ULS.
Design
A retrospective review of three-dimensional images obtained pre-operatively and at 1-year post-operatively.
Setting
Tertiary care pediatric institution.
Patients, Participants
Twenty-four patients with ULS.
Interventions
Thirteen patients received OS, and 11 received OS + ON.
Main Outcome Measure(s)
Craniometric measurements included anterior, posterior, and height asymmetry ratios; turricephaly index; and nasal and chin deviation.
Results
Both cohorts demonstrated significant post-operative improvements in anterior, posterior, and height asymmetry, as well as nasal and chin deviation (P < 0.05). The OS + ON cohort demonstrated a significant post-operative increase in the turricephaly index (P = 0.039), which was also significantly greater than in the OS-alone group in the intergroup comparison (P = 0.037).
Conclusions
OS with or without ON results in significant improvements in the posterior cranial vault and facial symmetry in patients with ULS. The addition of ON resulted in a significantly greater increase in cranial height, suggesting a role in patients with vertical deficiency.
Introduction
Unilateral lambdoid synostosis (ULS) is the rarest form of craniosynostosis, accounting for only 1-5% of all cases, and is characterized by posterior plagiocephaly with associated cranial vault, base, and facial asymmetries.1–3 Surgical correction aims to restore cranial symmetry, normalize intracranial volume, and mitigate stigmatizing features. Several operative techniques have been described for the management of ULS, including cranial vault remodeling, suturectomy with helmeting, springs, or distractors, and occipital switch (OS) procedures.4–6 The OS technique has gained popularity due to its ability to directly address posterior vault asymmetry by transposing the affected and unaffected occipital segments, thereby improving cranial shape and symmetry.7–14
The occipital neo-bandeau (ON) has been proposed as an adjunct to posterior cranial vault remodeling to enhance expansion and address vertical cranial deficiencies.15–19 While the theoretical advantages of combining OS with ON include improved cranial height and cranial vault morphology, the impact of this modification on morphologic outcomes has not been characterized. The purpose of this study was to compare craniometric outcomes in patients with ULS undergoing OS with or without ON using three-dimensional imaging analysis. We hypothesized that the addition of ON would result in improved cranial vault proportions, particularly in the vertical dimensions, without significant perioperative differences.
Methods
A retrospective review was conducted of patients with ULS who underwent either OS alone or OS + ON, following institutional review board approval from ***. The diagnoses of all patients were confirmed using pre-operative computed tomography scans. All patients had three-dimensional craniofacial images obtained pre-operatively and at 1-year post-operatively. No included patients had previous operative intervention, genetically identified syndromic craniosynostosis, or other congenital or acquired craniofacial pathology. Virtual surgical planning was performed pre-operatively. One surgeon performed OS in all patients, and a second surgeon performed OS + ON in all patients.
Three-dimensional craniofacial images were analyzed using the 3dMD Vultus (3dMD, Atlanta, GA) using our previously described methods.
9
Asymmetry ratios were selected to normalize for age-related variation in the patient cohort. Images were registered in the Frankfort horizontal, and a plane was chosen for each asymmetry measurement. For the anterior and posterior asymmetry ratios, an axial plane was defined from the glabella through the occipital protuberance (
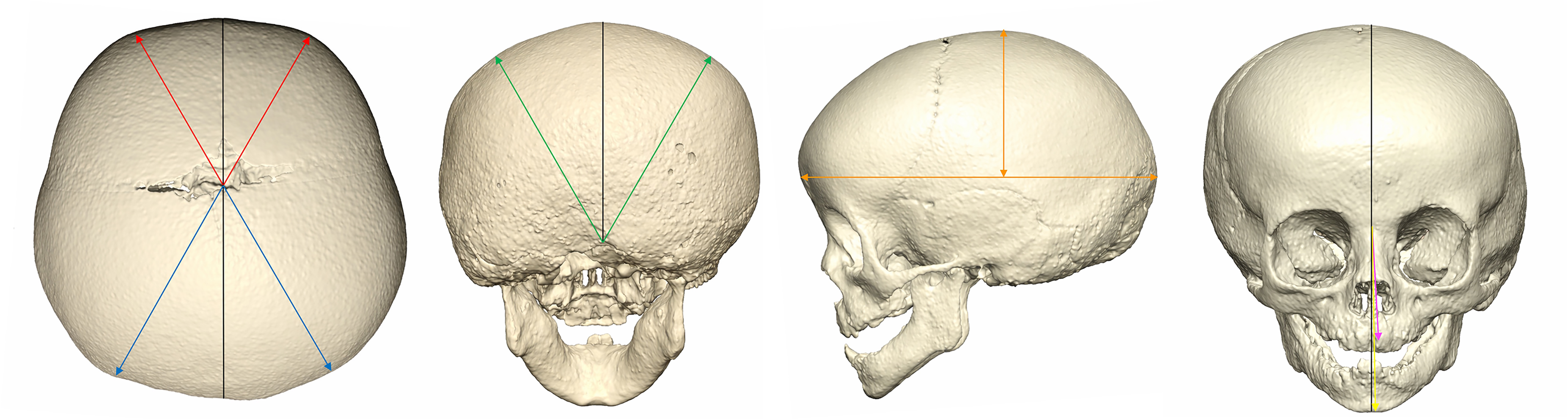
Craniometric measurement of patients with unilateral lambdoid synostosis. Anterior (Red) and posterior (Blue) asymmetry ratio (contralateral distance divided by ipsilateral distance). Height (Green) asymmetry ratio (contralateral distance divided by ipsilateral distance). Turricephaly index (Orange) (height divided by length). Nasal (Pink) and chin (Yellow) deviation (angle from midline to nasal tip and chin point).
All measurements were performed in duplicate by two authors and assessed for inter- and intra-observer reliability using Cohen's Kappa analysis with strong reliability (k = 0.83; k = 0.84). Statistical analyses were conducted with SPSS version 29 (IBM Corp., Armonk, NY). Pre- and post-operative measurements were compared with paired-sample t-tests, while comparisons between surgical groups were conducted with two-sample t-tests. Statistical significance was defined as P < 0.05.
Occipital Switch Cranioplasty Technique
All patients underwent OS using the same technique (
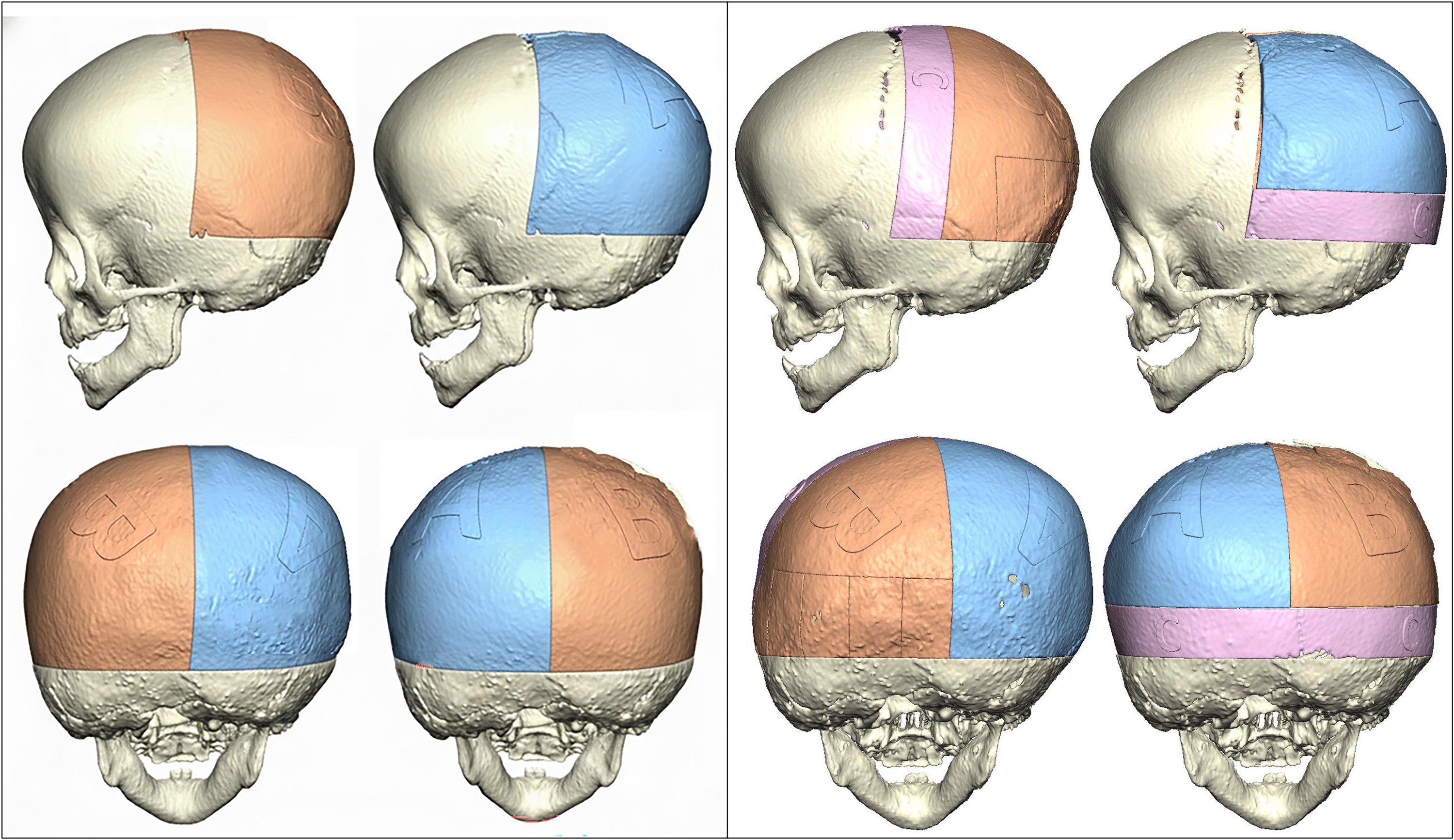
Occipital switch cranioplasty technique (Left) and occipital switch cranioplasty with occipital neo-bandeau technique (Right): Non-synostotic occiput (A), synostotic occiput (B), occipital neo-bandeau (C).
Results
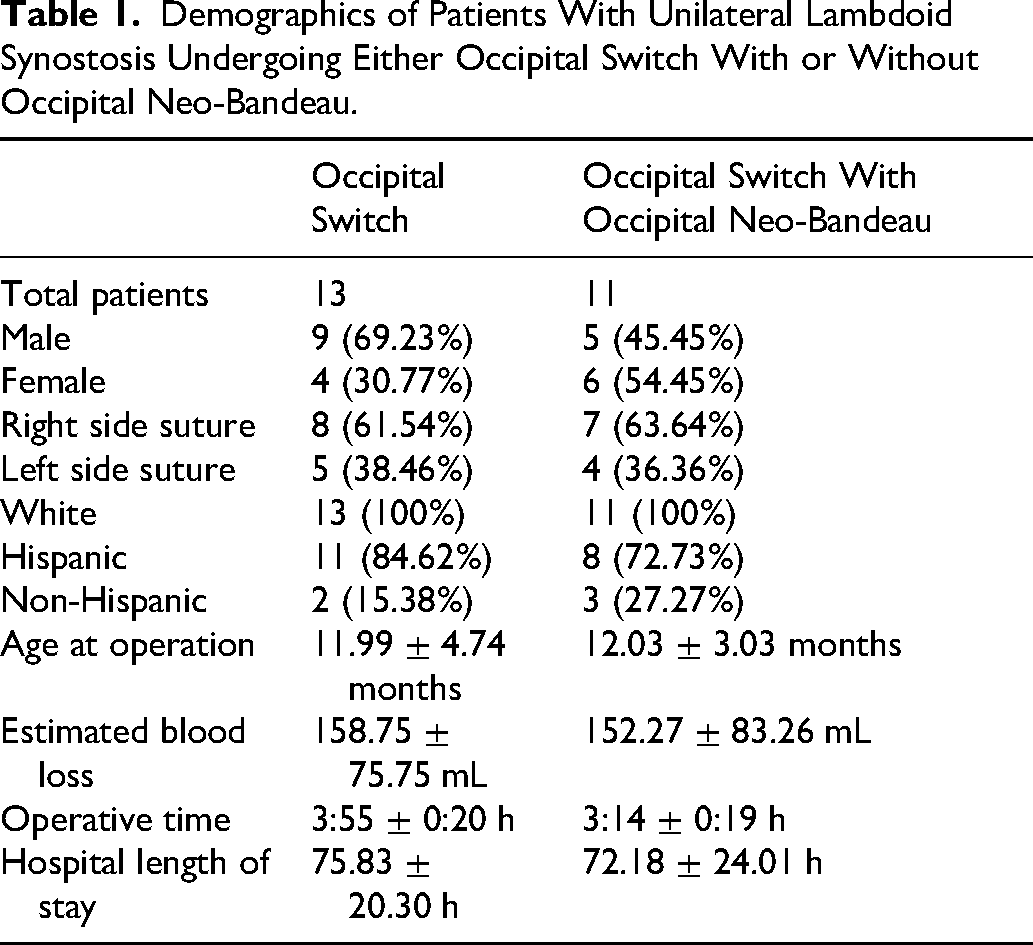
A total of 24 patients with ULS were included in the analysis: 13 underwent OS, and 11 underwent OS + ON (
Demographics of Patients With Unilateral Lambdoid Synostosis Undergoing Either Occipital Switch With or Without Occipital Neo-Bandeau.
In the OS group, significant post-operative improvements were observed in anterior asymmetry (P = 0.019), posterior asymmetry (P = 0.011), and height asymmetry (P = 0.040) (
Pre-Operative and Post-Operative Craniometric Measurement Comparison of Patients With Unilateral Lambdoid Synostosis Undergoing Either Occipital Switch With or Without Occipital Neo-Bandeau.
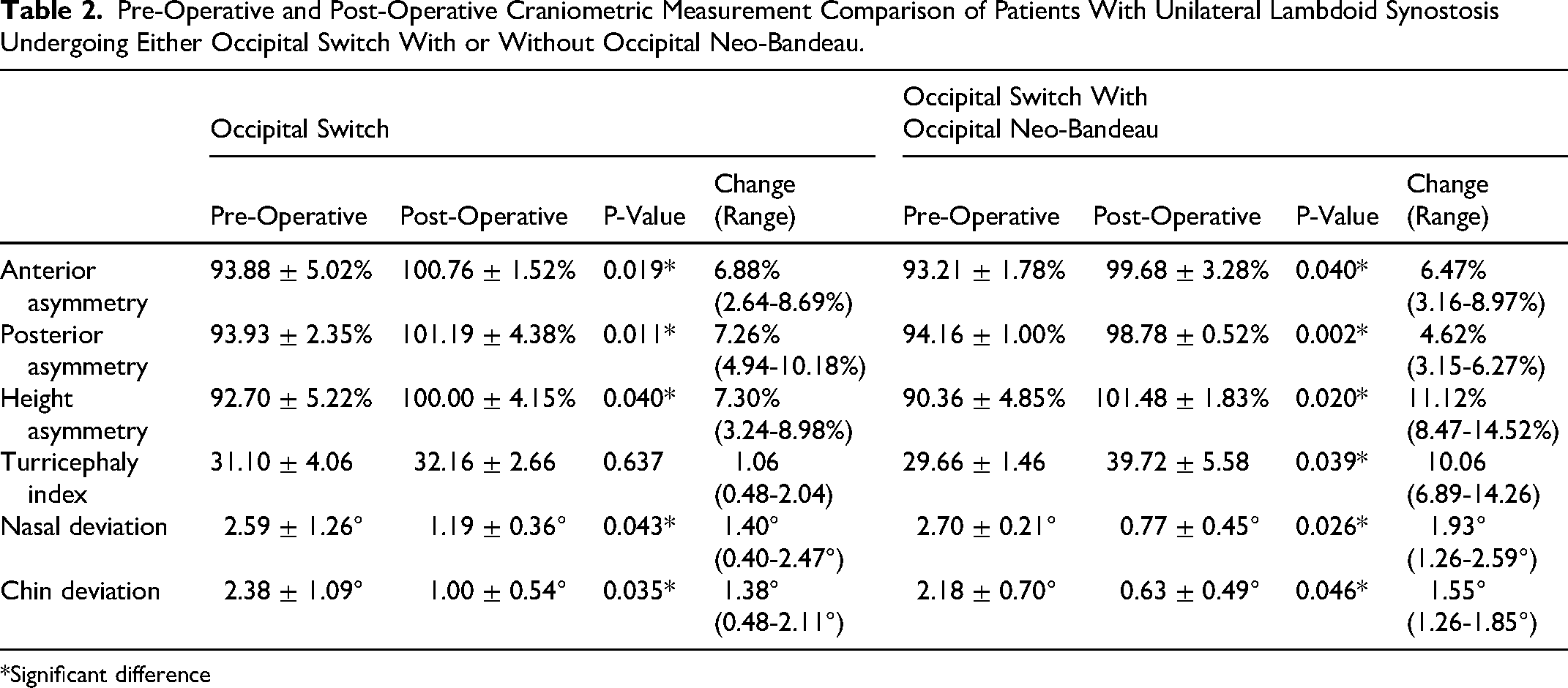
*Significant difference
Pre-operative craniometric measurements did not differ significantly between the OS and OS + ON cohorts for any variable (
Surgical Technique Craniometric Measurement Comparison of Patients With Unilateral Lambdoid Synostosis Undergoing Either Occipital Switch With or Without Occipital Neo-Bandeau.
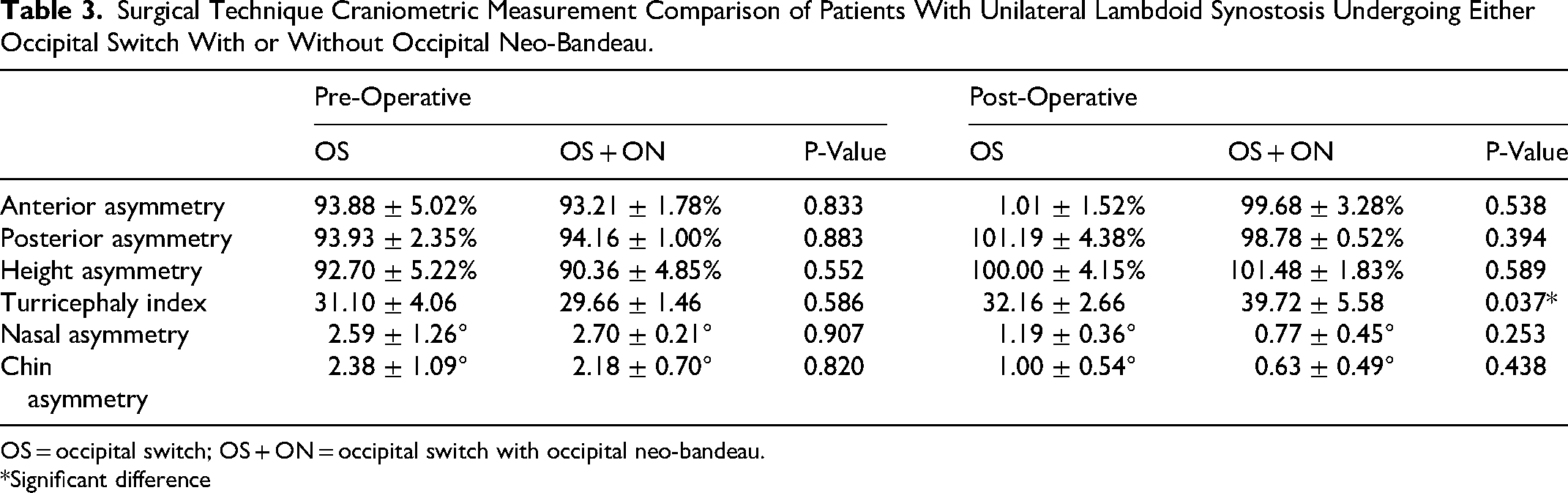
OS = occipital switch; OS + ON = occipital switch with occipital neo-bandeau.
*Significant difference
Discussion
ULS represents a rare and complex form of craniosynostosis, with deformity extending beyond the posterior cranial vault to involve the entire calvarium, cranial base, and facial symmetry.1–3 Although several operative techniques have been described, comparative outcome data remain limited.4–6 Historically, posterior vault deformities caused by lambdoid suture fusion were recognized as challenging because of the resulting complex cranial asymmetry. In response, more extensive posterior vault remodeling techniques were developed, including the OS, in which the posterior calvarial bones are removed, halved, and rotated to correct posterior plagiocephaly and reestablish symmetry.7–14
Smartt et al demonstrated that OS effectively reduced craniofacial asymmetry and provided better outcomes than non-operative management. 7 Subsequently, Elliott et al showed that while OS restores calvarial shape, there is a limited impact on cranial base morphology. 10 Nguyen et al further demonstrated improvements in the cranial vault and facial symmetry at 2 years following OS. 8 Anterior craniofacial improvements following OS were also shown by our group, in frontal asymmetry, nasal deviation, and chin deviation. 9 Long-term follow-up of patients undergoing OS for ULS by Ng et al found that most did not require revision surgery with good esthetic and functional outcomes. 14
An ON harvested from a biparietal donor site and rotated posteriorly to the occiput has been utilized in various posterior cranial vault remodeling techniques.15–19 The ON is rotated downward to improve projection and add posterior height by replacing the affected occiput.15–17 In this study, we evaluated three-dimensional craniometric outcomes following OS with or without ON to determine whether adding ON provides a measurable benefit over OS alone. Our findings demonstrate that both techniques result in significant improvements in posterior vault symmetry and facial midline alignment, while the addition of ON is associated with increased post-operative cranial height.
Both surgical cohorts demonstrated significant improvements in anterior, posterior, and height asymmetry, highlighting the effectiveness of the OS technique in addressing the characteristic posterior plagiocephaly associated with ULS and in improving overall calvarial morphology. These improvements were accompanied by significant reductions in nasal and chin deviation, suggesting that correction of posterior vault asymmetry also resolves facial deformities. Our findings align with previous studies demonstrating improvements in anterior craniofacial features without direct intervention, believed to be driven by growth and remodeling.7–9
The main finding of this study was a significant increase in the turricephaly index observed in patients undergoing OS with ON, both in the pre- to post-operative comparison and relative to the OS-alone cohort. This suggests that ON increases cranial height by rotating the neo-bandeau into the inferior occipital position. While increased cranial height may be desirable in select patients with pre-operative vertical deficiency, these findings support a selective approach to adding ON based on individualized cranial morphology. Following posterior vault remodeling, inadequate correction or growth restriction may lead to constriction of cranial height.14,20 Thus, we believe that increased posterior height through OS + ON will lead to improvements in long-term cranial proportions, which will be evaluated in future studies. Additionally, operative time was shorter in the OS + ON cohort, without differences in blood loss or length of stay, suggesting that adding ON does not increase perioperative morbidity.
Relevant to this discussion is the fact that ULS stands apart from other single-suture “non-syndromic” synostoses in that the involved suture extends so low on the cranial base that many neurosurgeons understandably do not feel it is safe to address it at the level of the mastoid bossing. This may impact growth and morphological outcomes, as well as the selection of surgical technique. It has been the senior surgeon's observation (***) that, for example, strip craniectomy for this condition, even when performed quite early, does not result in enough shape improvement to justify its inclusion as a recommended surgical option and at this point only employs open calvarial reconstructive techniques such as the one described here.
This study has several limitations, including its retrospective design and relatively small sample size. Given the rarity of ULS, these constraints are typical but limit statistical power. Additionally, post-operative imaging was limited to 1 year, precluding assessment of long-term growth-related changes and stability of correction. Differences in surgeon between OS and OS + ON may further confound comparisons. Future studies with larger, multi-institutional cohorts and longer follow-up are warranted to compare surgical techniques. Incorporation of patient and family-reported outcomes and neurodevelopmental metrics may also provide valuable insight into the functional implications of differing posterior cranial vault interventions.
Conclusions
OS is an effective technique for correcting cranial vault asymmetry and associated facial deviation in patients with ULS. The addition of ON results in increased post-operative cranial height. These findings suggest that OS alone provides reliable correction for most patients, while ON may be selectively employed to address specific vertical cranial deficiencies. Our three-dimensional analysis supports a tailored surgical approach based on individual cranial morphology.
Footnotes
Ethical Approval and Informed Consent Statement
Institutional review board approval was granted for the current study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.