
Abstract
Here we describe a metastatic hepatic cholangiocarcinoma (cholangiocellular carcinoma) in a 14-y-old Beefmaster cow that was euthanized because of depression and progressive weight loss. Gross changes included coalescing, white-to-yellow, firm-to-hard nodules with central areas of necrosis and mineralization that effaced much of the hepatic parenchyma, omentum, mesentery, ruminal serosa, and diaphragm. A fresh sample of a hepatic nodule was submitted for a modified acid-fast (MAF) stain during autopsy to rule out tuberculosis. The MAF stain was inconclusive, and the sample was subsequently submitted for a PCR assay for Mycobacterium spp. Histologically, all nodules consisted of a neoplastic proliferation of epithelial cells surrounded by extensive areas of desmoplasia, consistent with a metastatic cholangiocarcinoma. PCR for Mycobacterium spp. was negative. Although the histologic diagnosis in our case was metastatic hepatic cholangiocarcinoma, gross changes were strikingly similar to those described in cases of tuberculosis, highlighting the need to remain vigilant in the identification of zoonotic and suspected foreign animal diseases during autopsy to protect human health.
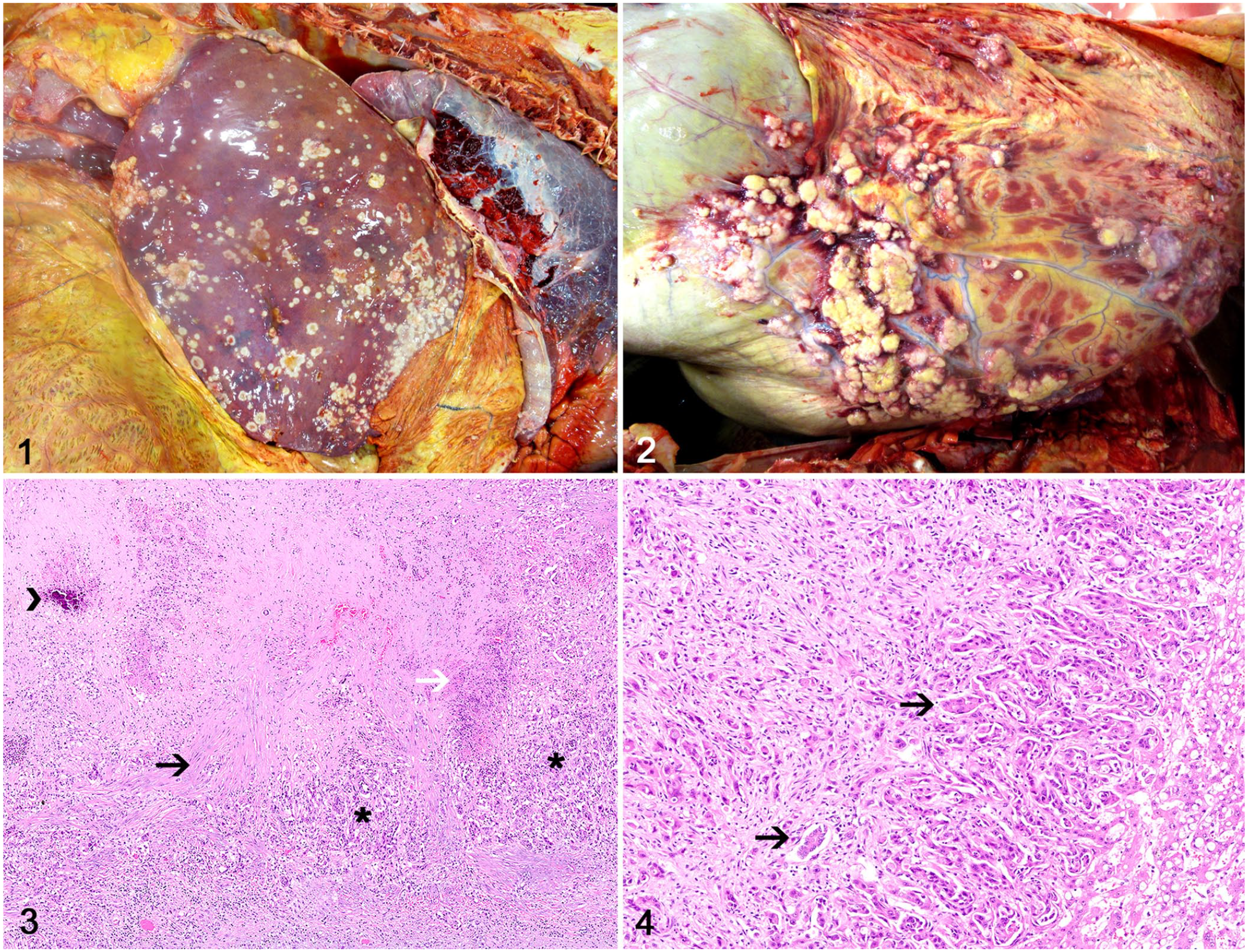
A 14-y-old Beefmaster cow was euthanized and submitted to autopsy after a 2-wk history of depression and progressive weight loss. The cow was from the state of Georgia, United States, had no travel history, and was the only affected individual in a herd of 13 cows. Grossly, the carcass was in poor body condition, with readily visible bony prominences and scant subcutaneous adipose tissue stores. The hepatic parenchyma was almost completely effaced by numerous, coalescing, white-to-yellow, firm-to-hard nodules of 5–25-mm in diameter that often had a central depression (Fig. 1). Similar nodules were present throughout the omentum, mesentery, ruminal serosa, and diaphragm (Fig. 2). Nodules had a yellow cut surface with granular areas of necrosis and a gritty consistency (mineralization). No other pathologic changes were observed.
Widespread cholangiocarcinoma in a cow.
Given the suspicion of tuberculosis, the autopsy was interrupted, and an impression smear of a hepatic nodule was immediately collected and submitted for a modified acid-fast (MAF) stain. The MAF technique used was a modified Kinyoun carbolfuchsin protocol (Aerospray TB Stainer, ELITechGroup; AFB acid fast control slide, Thermo Fisher). 13 However, the mineralization within the nodules interfered with the stain technique, and although positive and negative control samples stained correctly, no interpretation could be assigned for the diagnostic sample, and the diagnosis remained inconclusive at the time of autopsy.
Given the gross lesions and the inconclusive MAF stain results, a potential enhanced exposure risk to a possible zoonotic disease was considered. All personnel involved with the autopsy (veterinary students, anatomic pathology resident, and autopsy technicians) were informed about the suspicion of a potential case of tuberculosis, encouraged to seek information about the diagnosis as soon as the following day, and were dismissed from the autopsy room. Tissue samples (liver, rumen, omentum, mesentery, diaphragm, thoracic lymph node, and lung) were quickly collected by the pathologist and placed in 10% buffered neutral formalin, and the carcass was promptly disposed of according to the Athens Veterinary Diagnostic Laboratory (Athens, GA, USA) special biosafety guidelines. A sample of liver was also held frozen. Students and staff involved in the autopsy were using adequate personal protective equipment including boots, nitrile gloves, face shields, surgical face masks, and scrubs or disposable coverall suits. All instruments, tables, floors, and coolers (including walls and floor) were subsequently cleaned and disinfected using a solution of quaternary ammonium compound, degreaser, and bleach. In addition, footbaths were in use by the autopsy room access doors. The frozen sample from the liver was submitted for testing of possible Mycobacterium spp. using 2 PCR tests targeting the 16S rRNA and the heat-shock protein 65 (HDP65) gene immediately after the autopsy was completed.15,17
Formalin-fixed tissue samples were processed routinely for histology and embedded in paraffin wax one day after autopsy. Tissue sections (5 μm) were stained with hematoxylin and eosin and examined histologically 2 d after autopsy. Histologically, all nodules consisted of a neoplastic proliferation of epithelial cells arranged in small nests or ducts (Fig. 3) that were surrounded by dense or edematous areas of desmoplasia (Fig. 4). Neoplastic cells had abundant, polygonal, eosinophilic cytoplasm with distinct cell margins. Nuclei were round and had finely stippled chromatin with 1–3 nucleoli. There was moderate anisocytosis and anisokaryosis. The mitotic count was 4 per 2.37 mm2 (equivalent to 10 FN22/40× fields). Many of the nodules had extensive central areas of necrosis and mineralization. Vascular invasion by neoplastic cells was observed in the liver. No other lesions were observed. The PCR for Mycobacterium spp. was reported negative one day after autopsy.
Although the histologic findings were consistent with a metastatic cholangiocarcinoma affecting multiple abdominal organs, 19 the gross lesions in our case were strikingly similar to those described in cases of bovine tuberculosis, and mandated immediate (during autopsy) investigation into the possibility of a mycobacterial infection.8,12,16 Georgia is designated as an accredited bovine tuberculosis–free state by the U.S. Department of Agriculture. 9 However, infection is still present in wildlife species, such as deer, 18 which could represent a source of infection to domestic animals and humans. 7 For this reason, any suspect case must be tested, and positive results must be reported to the State Veterinarian’s office. 9 Therefore, it is of paramount importance that suspect cases are tested during gross examination in order that the necessary precautions can be conducted to avoid human exposure to a potential zoonotic infection. The State Veterinarian was not contacted in our case because a negative PCR for Mycobacterium spp. was reported ~24 h after the autopsy.
Primary hepatic neoplasms are rarely described in cattle.1,2,4-6,11,19 Although most cases occur as incidental findings in the slaughterhouse,1,3,6,10 tumors can occasionally lead to clinical signs associated with hepatic failure.11,19 The clinical signs in our case were nonspecific but likely associated with the presence of tumors in the liver and other abdominal organs. 19 In cattle, hepatocellular neoplasms are more frequently reported than cholangiocellular neoplasms.5,19 Hepatocellular adenomas and carcinomas typically consist of single, well-demarcated, dark-red to brown masses that efface one hepatic lobe or multiple masses distributed throughout the liver.5,19 In addition, diffuse hepatocellular carcinomas efface the entire hepatic parenchyma.5,19 Hepatocellular carcinomas can metastasize to regional lymph nodes, mediastinal lymph nodes, lungs, and spleen.1,10,19
Cholangiocellular adenomas are exceedingly rare and are characterized typically as a single, well-demarcated, yellow tumor.2,4 As evidenced by our case, cholangiocarcinomas (cholangiocellular carcinomas) can occur as multiple, irregular, yellow, firm nodules distributed throughout the parenchyma.5,11,19 Metastases have been reported in regional lymph nodes, lungs, and peritoneum.1,19 In our case, full characterization of metastatic sites was not completed as a result of the rapid inspection and disposal of the carcass after suspicion of tuberculosis. However, other than the previously mentioned primary and metastatic lesions, gross inspection did not reveal lesions in other organs.
Tuberculosis is a chronic infectious disease with a worldwide distribution that affects many animal species, including humans. 14 Bovine tuberculosis is caused by Mycobacterium tuberculosis var. bovis. 14 The clinical signs in affected cattle vary according to the location of the lesions, but are typically associated with infection of the respiratory or gastrointestinal tracts.7,8 The classic caseous granulomas that are characteristic of tuberculosis are yellow-to-white, firm nodules that frequently undergo necrosis and mineralization. Caseous granulomas associated with respiratory infection occur mainly in the mediastinal lymph nodes and lungs, but can also affect mesenteric lymph nodes in cases of infection resulting from ingestion of contaminated milk, food, or water.8,12,16 Widespread lesions in the liver, kidneys, mammary gland, or central nervous system are rare but can occur after dissemination from a primary lesion, 12 as suspected during autopsy in our case.
Footnotes
Acknowledgements
We thank the Bacteriology Laboratory personnel for their technical assistance with the modified acid-fast stain and PCR.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.