
Abstract
An adult female Cape porcupine (Hystrix africaeaustralis) was presented because of marked abdominal distension, acute dyspnea, and lethargy. Physical examination and standard radiographs revealed marked and diffuse gaseous dilation of the stomach and intestines of undetermined origin. The porcupine died despite medical therapy and surgical intervention. Postmortem examination revealed chronic fungal (Aspergillus flavus) rhinitis. Given that rodents are obligate nasal breathers, the rhinitis likely resulted in substantial upper airway obstruction leading to aerophagia.
Keywords
Aspergillosis is a mycosis that affects a diverse range of animal hosts.2,4,5,8 Aspergillus spp. are ubiquitous saprophytic fungi, and humans and animals are exposed regularly through the inhalation of hundreds of conidia on a daily basis.5,8 These fungi are considered opportunistic pathogens that may cause either localized sinonasal infections or disseminated infections, including pulmonary involvement in mammals.4,5,8 Aspergillus rhinosinusitis, also called sinonasal aspergillosis (SNA), has been reported primarily in humans, 13 dogs, 5 and cats, 4 in which the diagnosis and treatment of the disease remains challenging.4,5 Herein we describe a case of Aspergillus rhinitis in a Cape porcupine (Hystrix africaeaustralis) with an unusual clinical presentation, and the challenges associated with the antemortem diagnosis of this condition in a large rodent species.
A 17-y-old, 13 kg, female Cape porcupine, housed at the Zoo de Granby (Quebec, Canada), was found acutely lethargic, in sternal recumbency, and dyspneic. The animal was housed in a heated building with another Cape porcupine and had access to an outside enclosure. The indoor pen had a concrete floor covered with wood shavings and various enrichment items. The outside enclosure had a soil substrate and was shared with numerous meerkats (Suricata suricatta) when the weather was appropriate. The porcupines were fed daily with a combination of various vegetables and a mixture of rodent, primate, and canine pelleted foods. Physical examination was performed under general anesthesia, with ketamine and medetomidine IM. The porcupine received 100% oxygen (4 L/min) through a conical face mask during the procedure, and isoflurane supplementation towards the end of the procedure. The animal had low hemoglobin saturation (60–75%; >95% expected) associated with its dyspnea, which improved gradually over the course of the procedure. On physical examination, the porcupine had marked abdominal distension; a small diameter plastic polyurethane tube was inserted into the stomach to relieve the distension and to assess the presence of reflux. However, only 2–3 mL of fluid was recovered from the gastric tube. Radiographic examination revealed marked and diffuse gaseous dilation of the stomach and intestines without evidence of obvious obstruction (Fig. 1). A heterogeneous, partially mineralized structure of 5 × 4 cm was also observed in the left cranioventral abdomen adjacent to larger, discrete mineral densities assumed to be gravel. No obvious radiographic abnormality was noted in the nasal conchae or other sections of the skull. Ultrasonographic examination did not permit any further characterization of the abdominal structure in the left cranioventral abdomen given the presence of gas in the gastrointestinal tract. Hematologic and biochemical parameters were within reference intervals for this species. Empirical treatment was instituted with balanced crystalloid solutions during anesthesia; meloxicam once; trimethoprim–sulfadiazine q24h for 7 d; penicillin G benzathine–procaine q24h for 7 d; and metoclopramide q12h for 4 d.
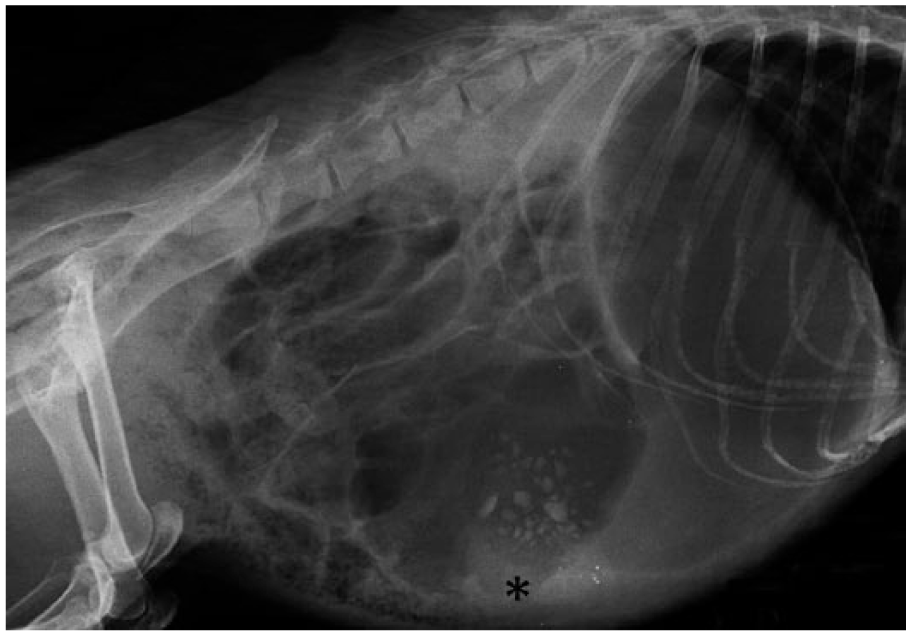
Marked and diffuse dilation of the gastrointestinal tract on a right lateral radiographic view in a Cape porcupine. A heterogeneous mass effect, believed to be caused by ingesta in the stomach, is also present in the cranioventral abdomen (asterisk).
The following day, the porcupine was in lateral recumbency with severe dyspnea and gaseous abdominal distension. The marked distension of the digestive tract and the suspicion of an abnormal abdominal structure motivated the need for an exploratory laparotomy to rule out causes such as intussusception, intestinal torsion, gastrointestinal foreign bodies, and digestive infiltrative disease. Anesthesia was induced as described previously. Following endotracheal intubation, the level of respiratory effort decreased dramatically. Given the suspicion of upper airway obstruction leading to aerophagia, endoscopic examination of the upper respiratory and digestive tracts was attempted prior to laparotomy. Flexible endoscopic examination of the oral cavity was unremarkable. The endoscopic evaluation of the nasal cavities was not possible because the diameter of the nares was too small to permit the entry of a 6.6-mm flexible endoscope or a 4-mm rigid endoscope. Orogastric intubation was performed to reduce gastric dilation prior to the exploratory laparotomy, and drained ~200 mL of green-tinged fluid from the stomach throughout the procedure. Preparation for a laparotomy was difficult because the skin was extremely delicate, and removal of the quills resulted in 2 small skin lacerations that were repaired. The quills were stabilized at their base connection with the skin and extracted vertically to avoid additional tears. A standard approach for a midline laparotomy was performed and revealed gaseous distension of intestines, marked enlargement of mesenteric lymph nodes, and significant thickening and multinodular appearance of ~15 cm of the jejunal wall. Biopsies of the jejunal wall and mesenteric lymph node were performed because there was suspicion of an infiltrative disease process. The heterogeneous mass identified on radiography was not located and was assumed to be artefactual or material within the gastrointestinal tract. Recovery was unusually long, and the porcupine regurgitated upon extubation. The regurgitated material was suctioned out of the oral cavity, but some ingesta were likely aspirated. Medical treatment was continued as initially prescribed; however, the porcupine was found dead the following day and was submitted for autopsy.
The most remarkable gross anatomic finding was marked and diffuse necrosis of the right and left nasoturbinates, maxilloturbinates, ethmoid turbinates, and olfactory nerves. Numerous, green plaques were noted on the mucosa of the left nasal cavity. One large plaque (15 × 7 mm), present in the medial meatus, invaded the wall of the left maxillary sinus (Fig. 2).The tracheal mucosa was diffusely erythematous. One fragment of straw was found in the primary left bronchus. Mandibular and mesenteric lymph nodes were hypertrophic. Tissues were fixed in 10% buffered formalin, embedded in paraffin, sectioned at 3 µm, stained with hematoxylin, phloxine, and saffron (HPS), and examined by light microscopy.
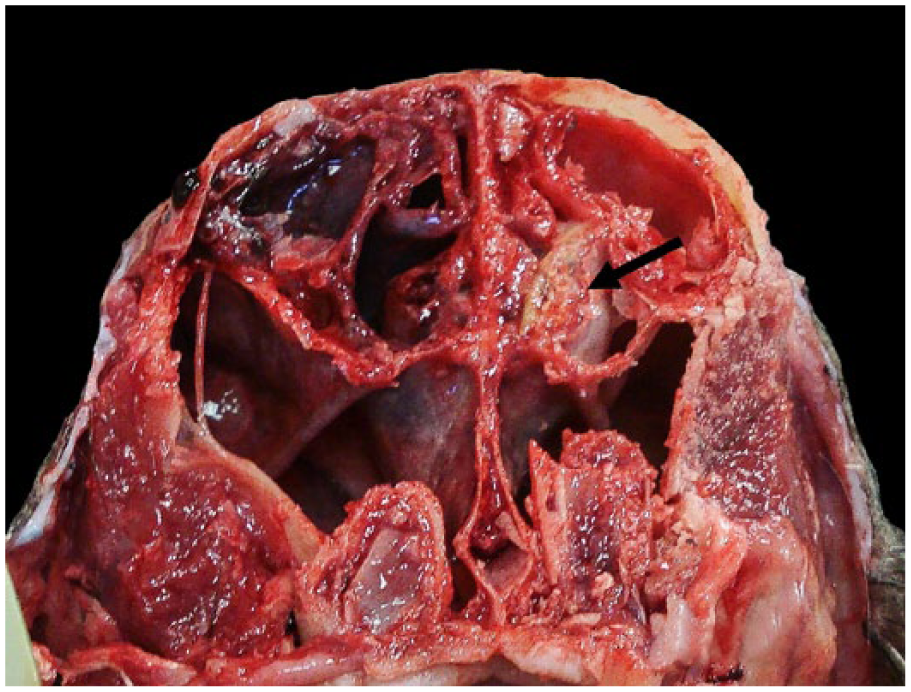
Marked destruction of the nasal turbinates in a Cape porcupine with congestion of the mucosa of the right nasal cavity and a fungal plaque in the left nasal cavity (arrow).
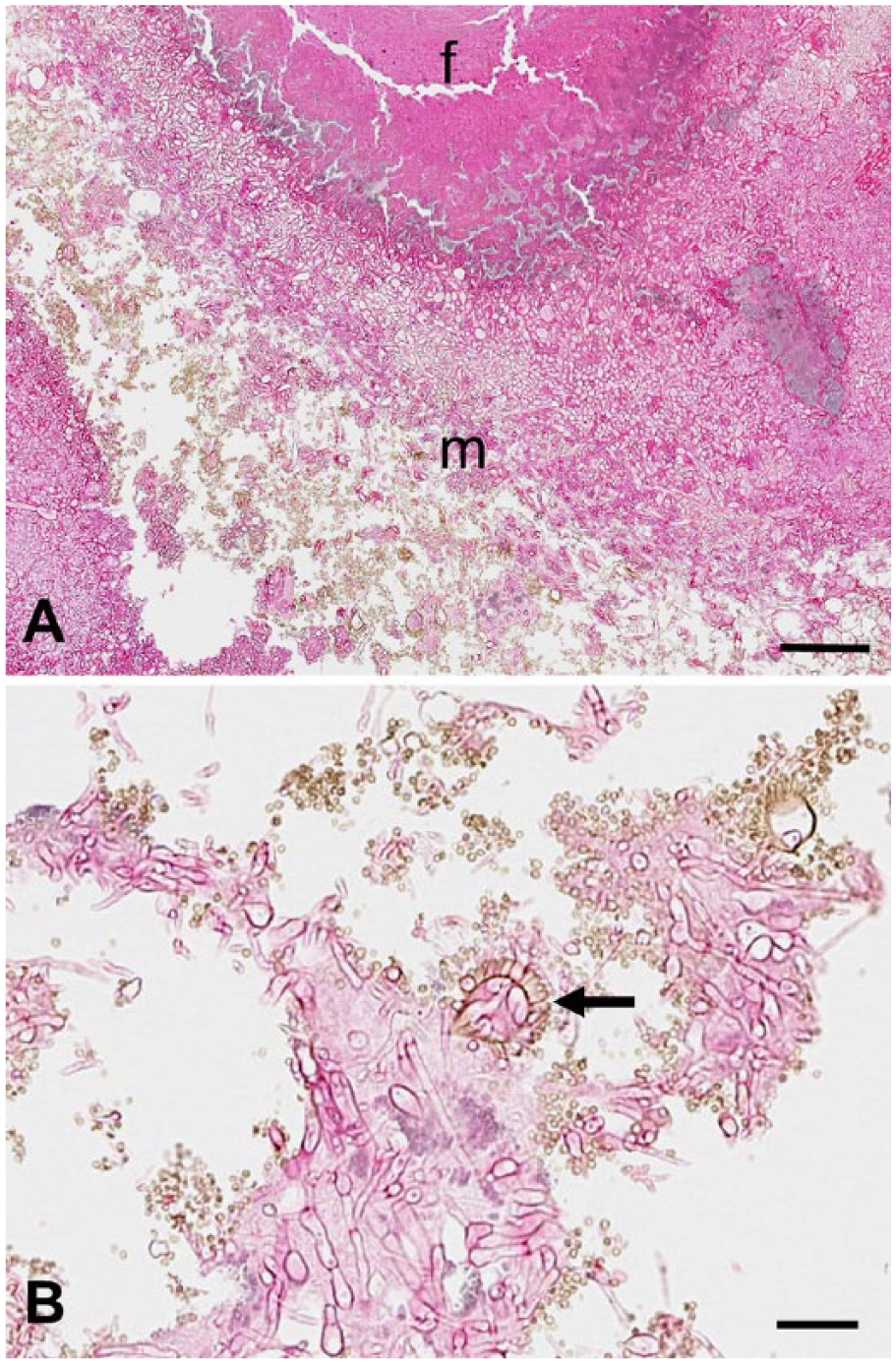
Histologic examination of the nasal turbinates revealed focally extensive ulceration of the mucosa associated with diffuse fibrosis and marked destruction of the turbinate bones. Examination of one of the plaques seen in the nasal cavities at gross examination showed a large aggregate of fibrin containing degenerate epithelial and inflammatory cells. Numerous branching and septate fungal hyphae were invading this fibrinous material (Fig. 3). Numerous conidia, often organized around vesicles, formed conidiophores showing characteristic morphology of Aspergillus spp. Colonies of gram-positive cocci were also present in moderate numbers. Other histologic findings noted were focally extensive tracheitis, multifocal mild aspiration pneumonia, and moderate lymphoid depletion and edema in the mandibular and mesenteric lymph nodes. No intralesional fungus or bacteria were seen in sections of the trachea and lung stained with periodic acid–Schiff and Brown-and-Hopps Gram stains. No significant changes were seen in other tissues. Tissue samples from the medial meatus submitted for fungal and aerobic bacterial cultures yielded Aspergillus flavus and a mixture of Pasteurella aerogenes and nonfermenting gram-negative bacilli. Aerobic bacterial culture from the bronchus yielded a mixture of Escherichia coli, Enterococcus sp., and alpha-hemolytic Streptococcus sp.
The final diagnosis was chronic ulcerative fibrinous fungal (Aspergillus flavus) rhinitis with extensive turbinate destruction. Despite the severity of turbinate damage, only superficial invasion by fungal hyphae was detected, which is a finding typically seen in canine SNA. 5 The P. aerogenes and nonfermenting gram-negative bacilli present in the cultured turbinates were likely secondary contaminants. Most likely, the degree of partially occlusive rhinitis significantly impacted normal respiration in this animal. The initial presentation of acute dyspnea could be explained either by the severe inflammation with subsequent progressive occlusion of the nasal cavities and/or by detachment of fibrinous fungal plaques causing mechanical obstruction. Given that rodents are obligate nose breathers as a result of the close apposition of the epiglottis to the soft palate, 7 partial or complete obstruction of the nasal cavities can be fatal. Short-term oral breathing induced by nasal occlusion causes significant respiratory insufficiency in mice. 14 Additionally, aerophagia has been induced experimentally in rodents and rabbits (another obligate nose breather) by obstructing the nasal passages. 10 Therefore, gaseous distension of the stomach and the intestines of this porcupine was likely the result of aerophagia secondary to the inspiratory dyspnea. Other causes of gastrointestinal gaseous distension such as obstruction or torsion were eliminated as potential etiologies during the exploratory laparotomy. However, idiopathic paralytic ileus or dysbiosis (with or without concurrent aerophagia) cannot be completely excluded as possible causes of the gastrointestinal signs observed. The presence of E. coli, Enterococcus sp., and alpha-hemolytic Streptococcus sp. within the airways was probably a consequence of the acute aspiration event or colonization from the nasal cavity.
Although a few cases of pulmonary or disseminated fungal diseases have been reported in porcupine species,1,3,9 fungal rhinitis has not been reported previously in a large rodent species, to our knowledge. A few case series of environmentally linked fungal rhinitis have been reported in laboratory rats.11,12 Additionally, rabbits and rodents have been frequently used as models of fungal rhinosinusitis for humans.6,15 Mammalian fungal rhinosinusitis is most often caused by Aspergillus spp. and more precisely by A. fumigatus. However, other species, such as A. flavus, are reported occasionally. 5
Although infections are commonly noted in immunocompromised patients,5,8 Aspergillus sp. can also be a primary pathogen, inducing rhinitis and/or sinusitis in immunocompetent individuals. 13 Predisposing factors of canine SNA remain unclear. However, facial trauma, nasal foreign bodies, and dental disease have been described as predisposing factors. 5 Regarding rodents and rabbits, ventilatory obstruction,6,15 foreign bodies (as carriers and local irritants), 11 concurrent infection (Sendaï virus), 11 and high environmental spore loads in corncob bedding 12 have been suggested as potential risk factors. None of these aforementioned risk factors was identified in our case; however, given the housing design and bedding, an undocumented exposure to high fungal spore counts cannot be excluded as a possibility.
Clinical signs in canine SNA commonly include chronic purulent nasal discharge, nasal pain, nasal planum ulceration or depigmentation, occasional sneezing, epistaxis, decreased appetite, depression, facial deformity, and epiphora. 5 Sneezing and nasal scratching, audible sniffing noises, inspiratory stridor, brown-black debris around the nostrils, and hemorrhages were observed in laboratory rats with Aspergillus rhinitis.11,12,15 In our porcupine, none of the reported signs of rhinitis, except dyspnea, were present, which did not facilitate the clinical diagnosis. Per observations by the keeper, the porcupine appeared to be clinically normal before its acute presentation. Only the inspiratory dyspnea might have indicated a potential upper respiratory tract problem. However, during the initial clinical presentation, the acute dyspnea was primarily thought to be related to pain because of the marked abdominal distension.
Despite years of research, establishing a diagnosis of canine SNA is still difficult. A combination of imaging (computed tomography [CT] or radiography), rhinoscopy or sinuscopy, biopsy with histopathology, cytology, fungal cultures, and serology is recommended to achieve a definitive diagnosis. 5 In our case, no skull abnormality was detected with conventional radiography, and access to a CT unit was not available. Furthermore, the acute presentation limited additional diagnostic procedures. In addition, postmortem examination confirmed that anterograde rhinoscopy could not be performed in this species of porcupine with the available endoscopic equipment given the narrowness of the nares. Even if the correct diagnosis had been established, appropriate treatment in the porcupine would have been a challenge; prolonged topical treatment via a catheter placed in the affected sinus is the recommended therapy in dogs 5 and would not have been accomplished easily in a porcupine.
Footnotes
Acknowledgements
We thank the technicians of the Animal Health Service and the dedicated keeper staff at the Zoo de Granby for their contributions to this case.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.