
Abstract
A 1.5-y-old spayed female Juliana pot-bellied pig was presented to the Purdue University Veterinary Teaching Hospital with a history of wasting and anorexia. Enlarged and partially mineralized lymph nodes were identified on radiographs and computed tomography scan. Generalized lymphadenomegaly and disseminated nodules in the lungs, liver, spleen, and kidneys were identified on postmortem examination. Histologic examination revealed caseonecrotic granulomas with numerous intracellular, acid-fast bacilli. Mycobacterium kansasii type II was identified as the etiologic agent by PCR amplification using universal Mycobacterium primers, direct sequencing of the PCR amplicon, and comparison to sequences in GenBank. We describe a case in a pot-bellied pig of mycobacteriosis caused by an atypical mycobacterial species and highlight the important role of laboratory testing in suspected cases of tuberculosis.
Mycobacterium kansasii was first described in 1953 in humans with disease conditions that resembled tuberculosis. 2 The organism is classified as a non-tuberculous mycobacteria and is considered an opportunistic pathogen, most noted for causing pulmonary disease in immunocompromised humans. 18 Under light microscopy, M. kansasii is an acid-fast positive bacterium that appears as a long, broad, and beaded bacillus. 2 The exact environmental origins of the bacterium are not completely known, although M. kansasii has been isolated from water sources. 19
Disseminated mycobacteriosis in pigs occurs primarily by infection from M. tuberculosis, M. bovis, and Mycobacterium avium complex (MAC; consisting of M. avium and M. intracellulare).12,14 Infections with MAC are the most common, particularly M. avium ssp. avium and M. avium ssp. hominissuis. The route of infection in pigs can be through inhalation, ingestion, or entry through cutaneous wounds. Cattle and birds are reservoirs and are a common source of infection for pigs. 14 Lesions typical of mycobacteriosis in pigs are granulomatous inflammation within lymph nodes and visceral organs, especially the lungs. Enlarged lymph nodes often have caseous foci and may contain areas of mineralization.5,10
A 1.5-y-old spayed female Juliana pot-bellied pig had a 4-mo history of weight loss, decreased appetite, nasal discharge, and dyspnea. Initial physical examination revealed depression and a poor body condition score of 1.5 of 5, decreased body weight (17.2 kg), muscle wasting, abnormal breath sounds and increased respiratory effort, nasal discharge, inappetence, and loose feces. Temperature and respiratory rate were within normal limits but tachycardia was noted (120 beats/min). Significant clinicopathologic findings included marked hypoproteinemia, anemia (decreased hematocrit, red blood cell count, and hemoglobin), leukocytosis characterized by a mature neutrophilia with a marked left shift and toxic neutrophils, and marked lymphopenia. No parasites were observed on quantitative fecal examination. Serum chemistry abnormalities included hypoglycemia, elevated urea and high-normal creatinine levels, hypercalcemia, hypochloremia, hypoproteinemia characterized by hypoalbuminemia and hypoglobulinemia, and elevated gamma-glutamyl transferase, creatine kinase, and aspartate aminotransferase. Standing laterolateral thoracic and skull radiographs revealed diffuse mixed bronchial and patchy interstitial lung patterns with a few ill-defined pulmonary soft tissue nodules, soft tissue opacification of the laryngopharynx region, and mandibular lymph node enlargement with faint dystrophic mineralization. Pre- and post-contrast computed tomography (CT; GE LightSpeed VCT 64-slice, General Electric, Milwaukee, WI) of the head and neck and delayed post-contrast CT of the thorax and abdomen revealed thoracic, subcutaneous, and abdominal lymphadenomegaly with stippled-to-peripheral, thin-rim mineralization and mild heterogeneous post-contrast enhancement (Figs. 1, 2). There was right renal aplasia and left renal hypertrophy with numerous renal cysts. The overall findings of mineralized lymphadenopathy, pulmonary infiltrates, and nodules with wasting were suggestive of bacterial (mycobacteriosis), fungal (e.g., cryptococcosis), or viral (porcine circovirus 2) disease, or more rarely neoplasia. Given the poor prognosis, the pig was euthanized and submitted for autopsy.
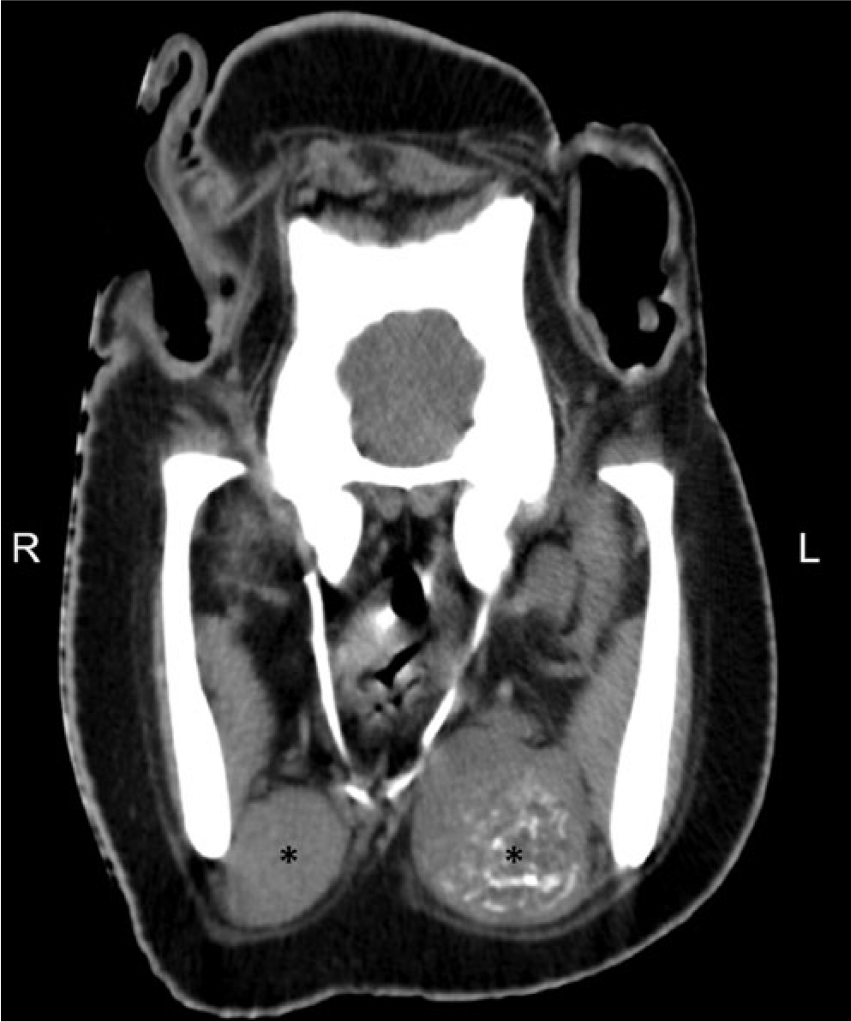
Lymphadenomegaly in a pot-bellied pig on computed tomography (CT) scan. Pre-contrast transverse CT image of the skull at the level of the mandibular ramus. The mandibular lymph nodes (*) are enlarged bilaterally with diffuse stippled mineralization of the left mandibular lymph node.

Post-contrast transverse computed tomography image of the thorax at the level of the first ribs showing enlarged cranial mediastinal lymph nodes (*) with peripheral hyperattenuating thin-rim mineralization; ∆ ascending aorta, ○ cranial vena cava.
At autopsy, the animal showed evidence of muscle wasting but had adequate adipose tissue. Mandibular, retropharyngeal, prescapular, inguinal, popliteal, tracheobronchial, caudal mediastinal, hepatic, mesenteric, and sublumbar lymph nodes were markedly enlarged; the largest of these was 7 cm in maximal dimension. On cut section, there was off-white to pale-tan mottling. Additionally, multiple lymph nodes contained gray-to-yellow, well-demarcated, central necrotic foci (Fig. 3). Pale-tan, firm, irregular, and raised nodules were present on the surface of all lung lobes and within the pulmonary parenchyma (Fig. 4). Remaining pulmonary parenchyma was red and heavy with multiple consolidated lobules. There was parietal and visceral pleural fibrosis with multiple fibrous adhesions between the lungs and thoracic wall. Fewer nodules with a smooth surface were identified within the liver, kidneys, and spleen.
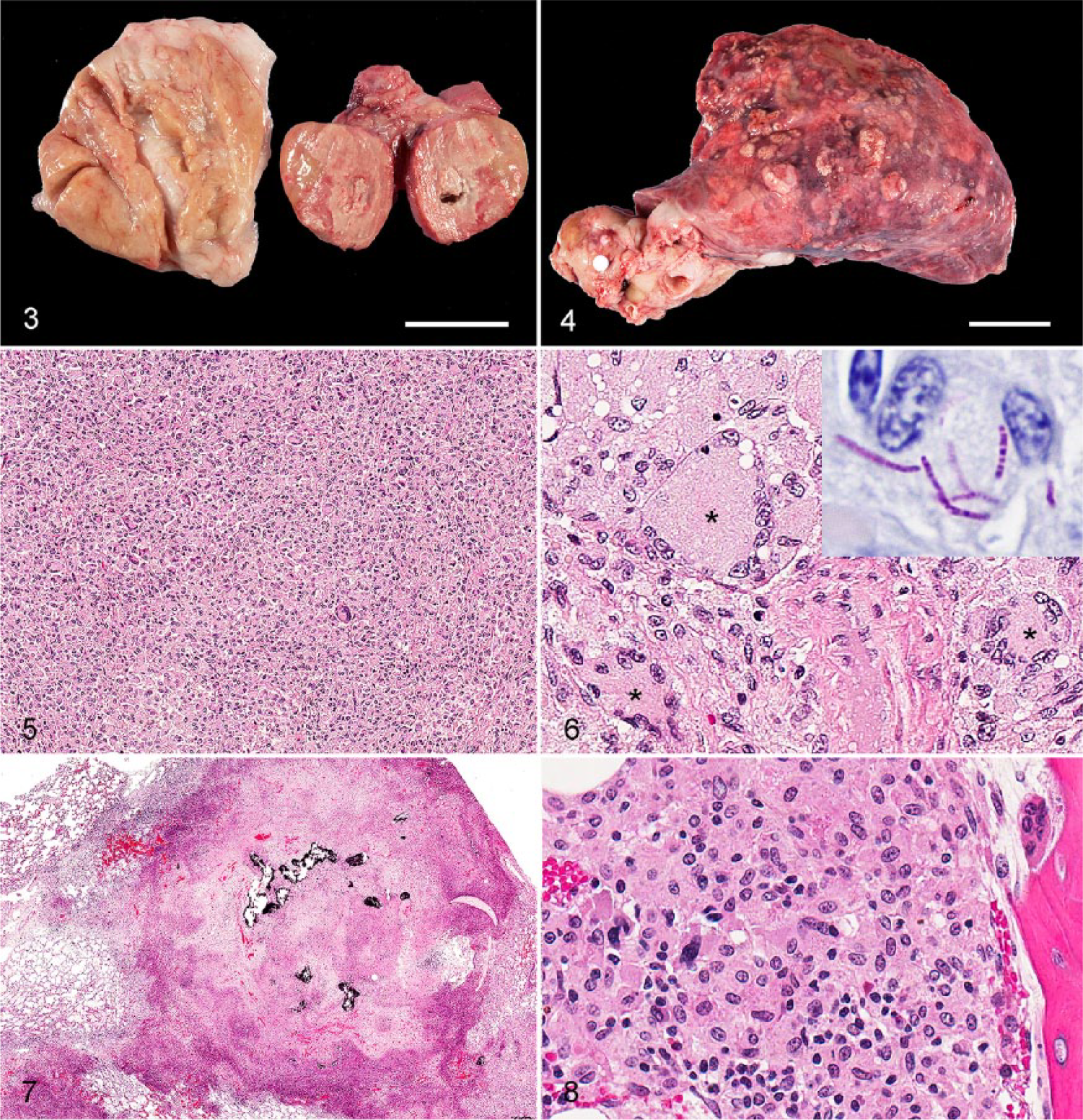
Mycobacteriosis in a pot-bellied pig.
Sections of lymph nodes, lungs, spleen, liver, left kidney, heart, stomach, small intestine, colon, bone marrow, brain, adrenal gland, and thyroid gland were fixed in 10% neutral-buffered formalin for 48 h and processed routinely for histology. Sections were stained with hematoxylin and eosin as well as Fite and Ziehl–Neelsen acid-fast stains. Samples of lymph node and lung were submitted to the National Veterinary Services Laboratories (NVSL) for culture.
Microscopically, nodal parenchyma was markedly expanded and largely replaced by infiltrates of epithelioid macrophages, which contained abundant, pale eosinophilic and finely vacuolated cytoplasm (Fig. 5). Numerous binucleate and multinucleate giant cells (MGCs) were also present (Fig. 6). MGCs had abundant eosinophilic and vacuolated cytoplasm and peripheralized nuclei. Large foci of caseous necrosis with islands of mineralized debris were also present.
Caseonecrotic granulomas effaced portions of the pulmonary, hepatic, splenic, and renal parenchyma (Fig. 7). In these organs, necrosis, mineralization, and lymphoid and neutrophilic infiltrates were more prominent than in the lymph nodes. Fibrosis surrounding granulomas was common in the lung. The visceral pleura was thickened by fibrosis and fibrinosuppurative inflammation. Suppurative bronchopneumonia was also identified. MGCs were abundant in hepatic granulomas. Multiple vessels within the kidney had fibrinoid necrosis of the vessel wall and were occluded by fibrin thrombi. A microscopic granuloma was also identified in the subendocardial myocardium of the interventricular septum. In sections of small intestine, the lamina propria was diffusely expanded by infiltrates of epithelioid macrophages, which multifocally extended into the submucosa and also partially effaced Peyer patches. The colon contained similar, but less severe, granulomatous inflammation within the mucosal lamina propria. Extensive granulomatous inflammation of the femoral bone marrow consisted mostly of epithelioid macrophages and a few lymphocytes and granulocytes (Fig. 8). Osteoclastic activity was apparent in the affected areas.
Both Ziehl–Neelsen and Fite acid-fast stains of lymph nodes revealed numerous beaded acid-fast bacteria, of ~10 µm, within the cytoplasm of macrophages. Fite acid-fast stain of colon also identified many intrahistiocytic acid-fast bacteria; a low number of intracellular acid-fast organisms were seen within nodules of the spleen, liver, lungs, and kidney using both acid-fast stains. Bacteria were not identified with Gram stain. These findings were consistent with mycobacterial species.
DNA was extracted at the Washington Animal Disease Diagnostic Laboratory from a formalin-fixed, paraffin-embedded lymph node sample, as described previously 8 (QIAamp DNA mini-kit, Qiagen, Valencia, CA). A 210-bp portion of the 16S-23S ribosomal internal transcribed spacer region was amplified, as described previously, 15 and sent to an outside vendor for sequencing (Genewiz, South Plainfield, NJ). Basic Local Alignment Search Tool (BLAST) was used to analyze the consensus sequence, and matched that of M. kansasii type II, at 100% sequence identity with GenBank accession AB232368. The sequence from this pot-bellied pig was input as GenBank accession MF959700. M. kansasii was also detected by molecular analysis of bacterial culture isolate from the submitted samples at NVSL. Our case of disseminated mycobacteriosis in a pet pot-bellied pig was suspected based on radiographic, CT, gross and histologic findings, and was confirmed by special stains, positive mycobacterial cultures, and sequencing techniques.
Few reports exist of isolation of M. kansasii from swine.1,5,14,16 In only 2 of these reports was the isolate associated with a corresponding lesion;5,14 however, histopathology was not performed in either of these reports. Descriptions specifically of mycobacteriosis in pot-bellied pigs are rarer. Three pot-bellied pigs were affected in an outbreak of mycobacteriosis caused by Mycobacterium bovis at a wild animal park. 17 The pigs had disseminated pulmonary granulomas with caseous necrosis, and M. bovis was isolated from the lungs and thoracic lymph nodes. However, to our knowledge, published reports of M. kansasii infection in pot-bellied pigs do not exist.
Among atypical mycobacteria, M. kansasii is a common isolate in cases of pulmonary mycobacteriosis in humans, and infection is typically seen after a predisposing pulmonary disease has occurred. 3 Disseminated disease is uncommon, but is most often seen in immunocompromised humans. 3 The disease state most commonly associated with infection by M. kansasii is acquired immunodeficiency syndrome caused by human immunodeficiency virus. M. kansasii usually causes disease in the later stages of acquired immunodeficiency syndrome (AIDS).3,18 The rate of infection by M. kansasii in humans with AIDS is ~0.5% per year. 11 Non-tuberculous mycobacteria are frequent isolates of infections in humans who are recipients of solid organ transplants, and M. kansasii is a common non-tuberculous mycobacterial isolate in both kidney and heart transplant recipients. 6 In one review, infection by M. kansasii in kidney transplant recipients most commonly involved the lungs, skin, and synovium. 4 The exact mode of transmission to humans has not been defined, and person–person transmission has not been demonstrated. It is thought that atypical mycobacteria are ingested, inhaled, or implanted. Aerosolization of small droplets is thought to be the cause of pulmonary disease in humans from sources such as potting soil dust and bathroom showers. 9
Little is described about disease and pathogenesis of M. kansasii in veterinary species, but it has been isolated from multiple domestic and non-domestic species. 13 Given that infection with M. kansasii in humans typically produces disease only in immunocompromised individuals, decreased immune function could have played a role in the severe disseminated disease that was present in our case. No history of prior illness or disease was reported in this particular animal that may have caused immunosuppression, and the pig had been vaccinated appropriately and dewormed. The owner reported that the pig was spayed at 1 y of age and began losing weight and developed intermittent nasal discharge over the ensuing months. The pig reportedly received several short courses of antimicrobials, but this only temporarily resolved the nasal discharge. Suppurative bronchopneumonia, consistent with a bacterial etiology, was present in our case at admission; however, this lesion was considered to be secondary to disseminated mycobacterial disease. No evidence of viral infection was identified microscopically. However, testing for viral agents was not performed in our case. Therefore, an underlying viral infection cannot be ruled out.
Types I and II are the most commonly isolated subtypes of M. kansasii. Type I is only isolated from humans; type II (sequenced in our case) is isolated from both humans and the environment, either of which may have been the source of infection in our case. 7 This animal was a pet with little outdoor exposure; therefore, a human in the household was initially considered as a possible source of infection. However, annual tuberculin skin tests on the pig’s owner were consistently negative. Furthermore, historically, M. kansasii has not been considered zoonotic. 9 Most atypical mycobacteria are opportunistic pathogens that inhabit the environment in ecosystems shared by humans and animals, and soil and water sources are thought to be the reservoir for the agent. 20 Therefore, another potential source of infection was the hospital environment at the time this pig was spayed. The pig was healthy prior to the spay procedure; its health progressively declined in the 4 mo following this procedure. Nosocomial infections have been reported in humans with atypical mycobacteriosis. 9 No environmental or respiratory samples were collected or tested and therefore a definitive source of infection was not determined.
Footnotes
Acknowledgements
We thank the NVSL for their contribution to this case in culturing tissue samples and sequencing Mycobacterium kansasii. We thank the ADDL Histology Laboratory staff for their technical support.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.