
Abstract
As a pathologist, postmortem examination of the equine carpus can be daunting. The anatomy is complex and oftentimes, small or subtle lesions have significant impact on lameness and secondary lesions such as catastrophic musculoskeletal fractures and other injuries. In performance horses, particularly racehorses, the carpus is a common site of injury and source of lameness. Given the predisposition of racehorses to developing carpal disease, familiarity with clinically relevant anatomy and common developmental, degenerative, traumatic, and inflammatory processes are imperative for thorough postmortem examination. Our aim is (1) to provide a concise summary of clinically relevant anatomy and function that serves as a guide for postmortem evaluation of the equine carpus, and (2) to review common carpal injuries and diseases in actively training, racing, or retired racehorses, including developmental lesions (incomplete ossification, osteochondromata), infectious and inflammatory lesions (septic arthritis and tenosynovitis), and degenerative and traumatic lesions (degenerative and traumatic osteoarthritis, osteochondral fragmentation, and polyostotic catastrophic “breakdown” fractures). Representative gross and histologic images are presented along with corresponding antemortem and postmortem diagnostic images, and a review of current scientific literature pertaining to the pathogenesis of these equine carpal lesions.
Keywords
Introduction
The carpus has complex anatomic and functional components comprising 2 stacked rows of cuboidal bones that articulate with the distal end of the radius and proximal end of the metacarpus, providing hinge-like movement of the proximal 2 joints, 20 and planar movement of the distal joint in the dorsal–palmar direction. 18 Carpal lameness is most common in active and retired racehorses, where repetitive forces sustained during racing and training likely exceed normal physiologic stresses and strains, resulting in degenerative changes that often lead to performance-limiting lameness and injury. 81 In over 4,000 postmortem examinations on horses from California racetracks between 1991 through 2006 (84% Thoroughbreds, 10% Quarter Horses, and 2% Standardbreds), carpal fractures were identified in the California Postmortem Program initiated by the California Horse Racing Board, to be the second and third most common cause of fatal musculoskeletal injury in Quarter Horses and Thoroughbreds, respectively. 77 Moreover, surgery and iatrogenic injections performed to manage carpal lameness and injury are associated with carpal infections (i.e., septic arthritis and tenosynovitis). 69
Although somewhat controversial, developmental abnormalities involving endochondral ossification or conformation have been reported to predispose to lameness that can impact future performance.2,5 Knowledge of functional carpal anatomy and common lesions associated with carpal lameness, traumatic injury, and inflammatory processes is important to guide postmortem dissection and evaluation. Our objective in this review is to provide diagnostic pathologists with a succinct reference of clinically relevant anatomy and review of diseases and lesions most commonly encountered in the carpi of racehorses.
Anatomy
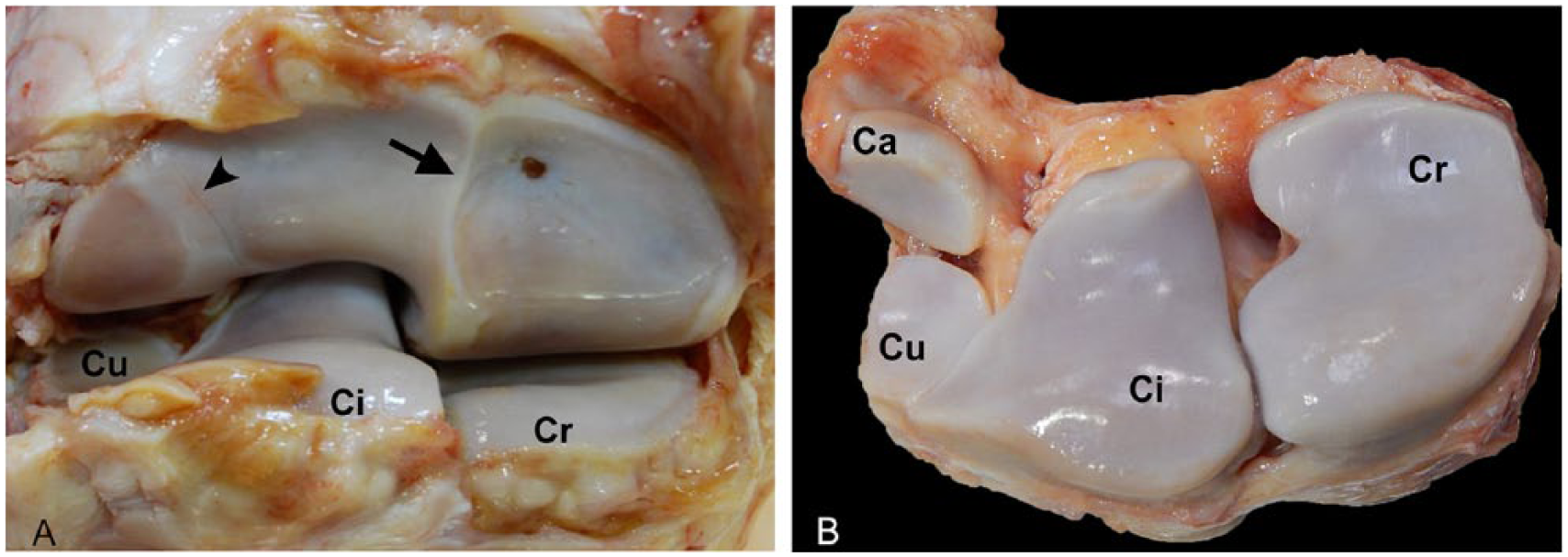
The equine carpus incorporates 3 joints from proximal to distal: the antebrachiocarpal (radiocarpal; Fig. 1), middle carpal (Fig. 2A–C), and carpometacarpal joints (Fig. 2D). Carpal bones comprise 7–9 cuboidal bones that include, from medial to lateral: the radial (Cr), intermediate (Ci), ulnar (Cu), and accessory (Ca) carpal bones forming the proximal row of carpal bones; and the second (C2), third (C3), and fourth (C4) carpal bones forming the distal row, with the first carpal bone reported in 25–50% of horses, and the fifth carpal bone rarely present (1–3%).51,70,71Although intercarpal articular surfaces exist between lateral and medial, and dorsal and palmar aspects of individual carpal bones, the most commonly reported and treated lesions pertain to the dorsoproximal and dorsodistal articular surfaces of the antebrachial and middle carpal joints.64,70
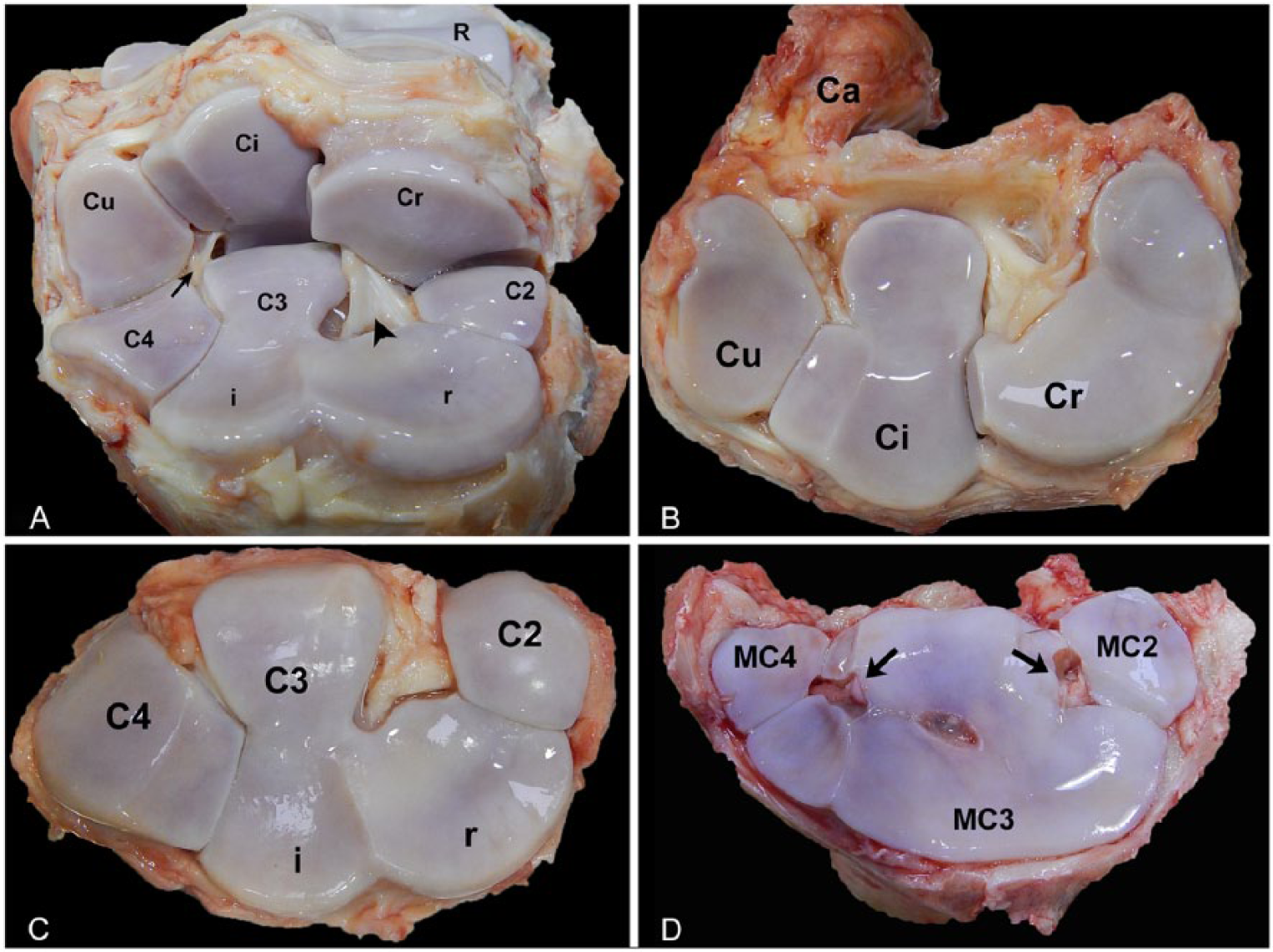
In the standing horse, the carpus is maintained in full extension; however, in 2-dimensional kinematic studies of the trot, the carpus shows an average range of motion in the sagittal plane of 89.5 ± 5°, divided into swing and stance phases that include a large component of flexion in the swing phase (average 83.5°) and a smaller component of extension in the stance phase (average −6.0°). 4 Three-dimensional kinematic studies confirm the predominant rotational motion of flexion-extension in the sagittal plane; however, we have also identified small components of internal rotation, and dorsal displacement of the metacarpus relative to the radius, which with higher speeds could produce larger compressive and shear forces that may increase the risk of injury. 18 The extensive attachments of the medial and lateral collateral ligaments to the distal radius, carpal bones, and proximal end of the metacarpus confine movement to the sagittal plane. Overextension is prevented by the palmar carpal ligament, formed by thickening of the palmar aspect of the joint capsule, which, along with the flexor retinaculum, extends from the palmar aspect of the accessory carpal bone to the palmaromedial aspect of the joint. 20 Together, the palmar carpal ligament and flexor retinaculum form the palmar annular carpal ligament that encloses the flexor tendons as well as medial and lateral neurovascular structures. 60 The palmar carpal ligament is also the origin of the accessory ligament of the deep digital flexor tendon (inferior, or distal, check ligament). Interosseous ligaments, including the dorsal, transverse, and medial/lateral palmar intercarpal ligaments maintain carpal bone alignment and prevent hyperextension. 84 Transverse intercarpal ligaments are difficult to visualize during routine postmortem examination and carpal disarticulation. However, the medial and lateral palmar intercarpal ligaments are easily identified by maintaining the middle carpal joint in partial flexion while partially disarticulating by incising over the dorsal joint capsule (Fig. 2A).
Because of the anatomic complexity of the carpus, often 5–7 standard radiographic projections (dorsopalmar, lateromedial, both dorsolateral–palmaromedial and dorsomedial palmarolateral obliques, flexed lateromedial, and flexed dorsoproximal–dorsodistal “skyline” views) are considered necessary for satisfactory evaluation in the live horse.64,74 Although not necessary, in our experience, if available, antemortem carpal radiographs or other forms of diagnostic imaging such as computed tomography (CT), magnetic resonance imaging (MRI), or ultrasound can prove quite useful during postmortem evaluation by their ability to reveal small, yet often clinically significant osteochondral fragments or non-displaced and/or incomplete fracture planes that may be difficult to discern on gross inspection. Digital files of antemortem radiographs can be obtained from the referring veterinarian via email, or good quality radiographs can be acquired postmortem of either the intact carpus or disarticulated rows of carpal bones to help identify lesions.
Antebrachiocarpal joint
The articulating surfaces of the antebrachiocarpal joint allows for the greatest degree of flexion in the carpus. 20 In full extension, the medial parasagittal ridge of the distal end of the radius separates the radial and intermediate facets of the radius, and the lateral groove formed by the fusion of the styloid process of the ulna with the radius separates the articular facets of the Ci and Cu. 33 In flexion, a proximodistal step is formed by the distal displacement of Cr relative to Ci, thus the mnemonic “i is high” (Fig. 1). The shape of the ulnar carpal bone can vary, and occasionally small osseous bodies are associated with the distal palmar aspects of this bone.51,71 Findings from radiology 71 , MRI, and histology 51 of these small osseous bodies in non-lame horses were compatible with clinically insignificant anatomic variation or chondro-osseous metaplasia at the origin of the lateral palmar intercarpal ligament, 51 rather than palmar osteochondral fragments associated with fractures in the dorsal aspects of the carpal bones, 27 or avulsion of the lateral palmar intercarpal ligament from the ulnar carpal bone. 7
Middle carpal joint
The articular surface of the middle carpal joint is different than the antebrachiocarpal joint, with the proximal surfaces of C2, C3, and C4 having concave dorsal as well as convex palmar profiles that are reciprocal to the distal articular surfaces of Cr, Ci, and Cu (Fig. 2A–C). 73 C3 is the largest of the 3 bones in the distal row and is “L” shaped with 3 distinct regions: the palmar portion that is rarely injured, and the dorsal portion that is divided by a distinct sagittal ridge into radial (medial) and intermediate (lateral) facets, which are frequently injured in racehorses.54,64 As mentioned above, the medial and lateral palmar intercarpal ligaments that span the proximal and distal rows of carpal bones are important structures that, in conjunction with the collateral ligaments, prevent dorsal displacement of the proximal row of carpal bones. 84 The medial palmar intercarpal ligament originates from the distolateral surface of the radial carpal bone and inserts on the proximal palmaromedial surface of the third carpal bone and the proximal palmarolateral surface of the second carpal bone, forming a sheet-like band divided into variably defined fiber bundles. 85 The lateral palmar intercarpal ligament typically forms a triangular band of unbundled fibers that originates on the distal portion of the palmaromedial surface of the ulnar carpal bone with a few fibers attaching to the palmarolateral surface of the intermediate carpal bone, and predominantly inserts on the proximal palmarolateral surface of the third carpal bone, with a few fibers inserting on the palmaromedial surface of the fourth carpal bone. 85 Despite their relatively small size, inspection of these intercarpal ligaments is imperative because lesions, including avulsion fractures, 7 and degeneration or partial to complete ligamentous tears, are reported as significant sources of carpal lameness and instability, and are often concurrent with carpal osteochondral “chip” and bi-articular “slab” fractures.14,28,35,47,58,87
Carpometacarpal joint
In contrast to the antebrachiocarpal and middle carpal joints, the carpometacarpal (CMC) joint is considered a low motion joint, with the distal row of carpal bones remaining in contact with the proximal extremity of the metacarpus. 72 The CMC joint is composed of the distal surfaces of C2, C3, and C4, which articulate with the proximal ends of the third metacarpus (MC3) flanked medially and laterally by the second (MC2) and fourth (MC4) metacarpi, respectively 72 (Fig. 2D). In addition to the medial and lateral collateral ligaments that extend from the distal end of the radius to the proximal part of the metacarpi, small medial and lateral intercarpal ligaments originate between C2 and C3, and between C3 and C4, inserting between the articulation of MC2 and MC3, and between MC3 and MC4, respectively (Fig. 2D). 51 Because the CMC joint communicates with the middle carpal joint, one should be aware that septic arthritis within the middle carpal joint may give rise to septic arthritis in the CMC joint. Moreover, clinical interpretation of diagnostic analgesia performed at the proximal aspect of the metacarpus (e.g., high 4-point block) can be difficult because of the medial and lateral distopalmar synovial outpouchings that extend along the axial aspects of the proximal ends of MC2 and MC4 in the region of the origin of the suspensory ligament. 25 In a study of cadaver limbs, nearly all CMC joints had a variable articulation between C3 and MC3, whereas only 3 of 200 joints did not have a measurable articulation between C3 and MC3. 63 Lesions in the CMC region, including desmitis of the origins of the suspensory ligament and accessory ligament of the deep digital flexor tendon, 15 syndesmopathies between the metacarpal bones, intercarpal ligament, and osseous abnormalities between C2/C3 and MC2/MC3, and lesions consistent with bone marrow edema of the medial aspects of the carpal and metacarpal bones, 59 can be difficult to identify radiographically or ultrasonographically, necessitating nuclear scintigraphy and/or MRI to diagnose. 50 In our experience, the CMC joint is difficult to disarticulate for gross examination, and unless indicated in the history, is not often disarticulated during routine postmortem examination.
Carpal canal and carpal sheath
The carpal canal is located along the palmar aspect of the carpus, confined by dense fascia (the palmar annular carpal ligament, or carpal flexor retinaculum) that forms a complex subdivided tunnel-like structure extending from the proximal margin of the accessory carpal bone to the proximal metacarpus. 60 The carpal flexor tendon sheath (carpal sheath) encloses the tendons and synovial sheaths of the flexor carpi radialis, superficial and deep digital flexor tendons, as well as neurovascular structures including the medial and lateral palmar nerves, the palmar branches of the median artery and vein, and radial artery and vein. The sheath extends 8–10 cm proximally from the antebrachiocarpal joint and distally to the proximal third or middle of the metacarpus. 20 Lameness associated with the carpal sheath is often the result of compression of the soft tissue structures contained within the lumen that can arise from effusion caused by idiopathic synovitis or trauma-associated intrathecal hemorrhage (e.g., accessory carpal bone fracture), space-occupying lesions (e.g., distal radial osteochondromata), diseases of tendons and ligaments contained within the sheath, or diseases of the palmar annular carpal ligament itself caused by orthopedic overload or hyperextension injury.21,30,60,88
Developmental lesions
In young foals (i.e., <2 mo of age), cuboidal bones of the carpus are incompletely ossified and thus are inherently susceptible to injury. 3 Although the degree of ossification at birth varies among foals, neonatal carpal bones typically have a rounded appearance with thick radiolucent spaces that represent hyaline cartilage surrounding ossification centers of the carpal bones. Ossification is often incomplete, is best seen on a dorsopalmar radiograph (Fig. 3A), and can be difficult to discern grossly (Fig. 3B, 3C) or histologically in demineralized specimens. Although not the focus of this review, incomplete ossification also occurs in the cuboidal bones of the tarsus.
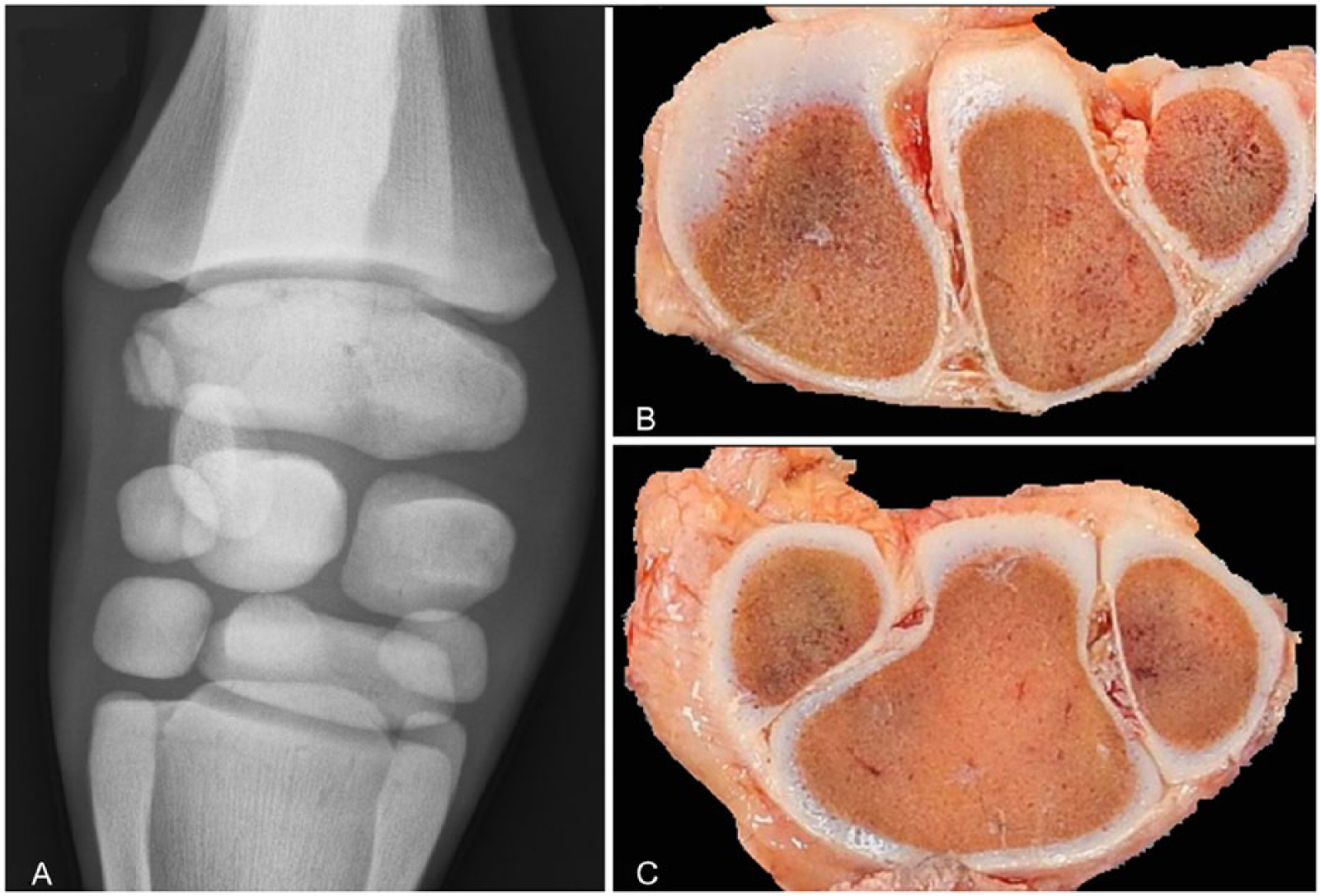
Incomplete ossification of the carpus in an immature foal.
In addition to leading to disrupting growth plates or increasing loads on joints, incomplete ossification of the cuboidal bones is one cause of angular limb deformities. Angular limb deformities are common, with one study of neonatal Thoroughbred foals reporting only 2 of 67 (3%) carpi having straight conformation and valgus angular deviations up to 4° considered normal. 67 Although a small proportion of angular deformities may “self-correct” in some foals, many are treated with a variety of therapies including hoof trimming, splinting, periosteal stripping, and transphyseal bridging, which are most effective if implemented prior to growth cessation of the distal radial physis by 60 wk of age. 62 Regardless, studies of the effect of angular limb deformities on future musculoskeletal problems show conflicting results as to impact on performance,2,5,83 whereas other carpal conformational deformities (e.g., “offset knees” conformation) have been associated with an increased risk of injury.2,64
Osteochondrosis is a well-documented equine developmental bone disease at multiple predisposed sites as a result of endochondral ossification. Osteochondrosis of the carpus is rare; however, osteochondrosis dissecans of the third and fourth carpal bones is reported in foals with angular limb deformities, 43 and subchondral cyst-like lesions (thought to be a manifestation of osteochondrosis) have been reported in the medial aspect of the distal radial epiphysis in 4 juvenile horses. 75
As mentioned above, osteochondromata are cartilaginous exostoses characterized by a radiolucent hyaline cartilage cap overlying endochondral bone that communicates with the medullary cavity of the parent bone. 78 Osteochondromata arising from defects of the perichondrial ring of the distal radial physis can grow and protrude into the carpal canal, leading to deep digital flexor tendinitis, synovitis of the carpal sheath, and lameness that could affect current, and potentially future, performance. Surgical removal of the mass with debridement of the deep digital flexor tendon results in a good prognosis, 88 and although malignant transformation of these lesions is not reported in horses to date, lesions are often submitted for evaluation as excisional biopsies (Fig. 4).
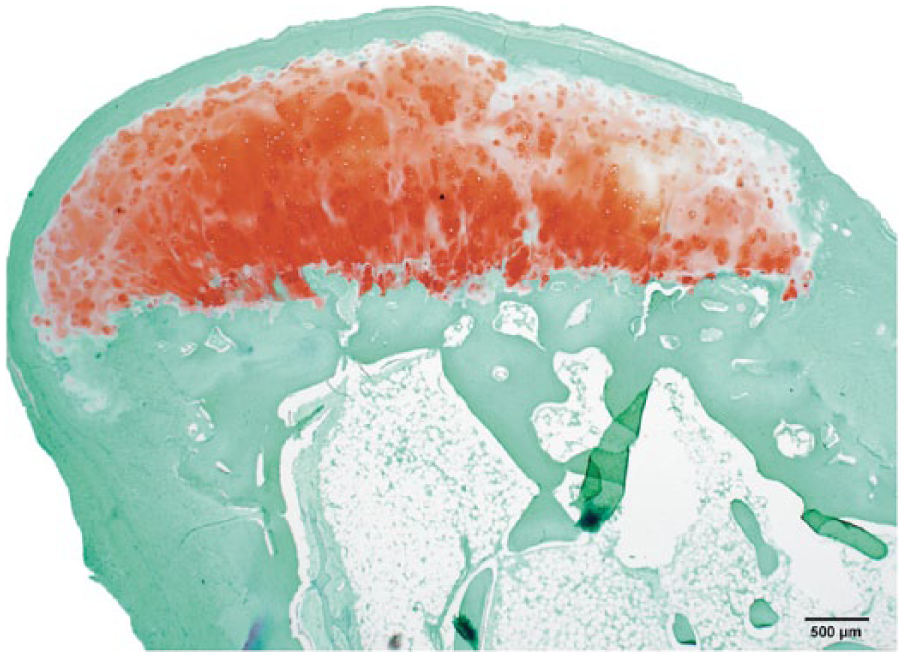
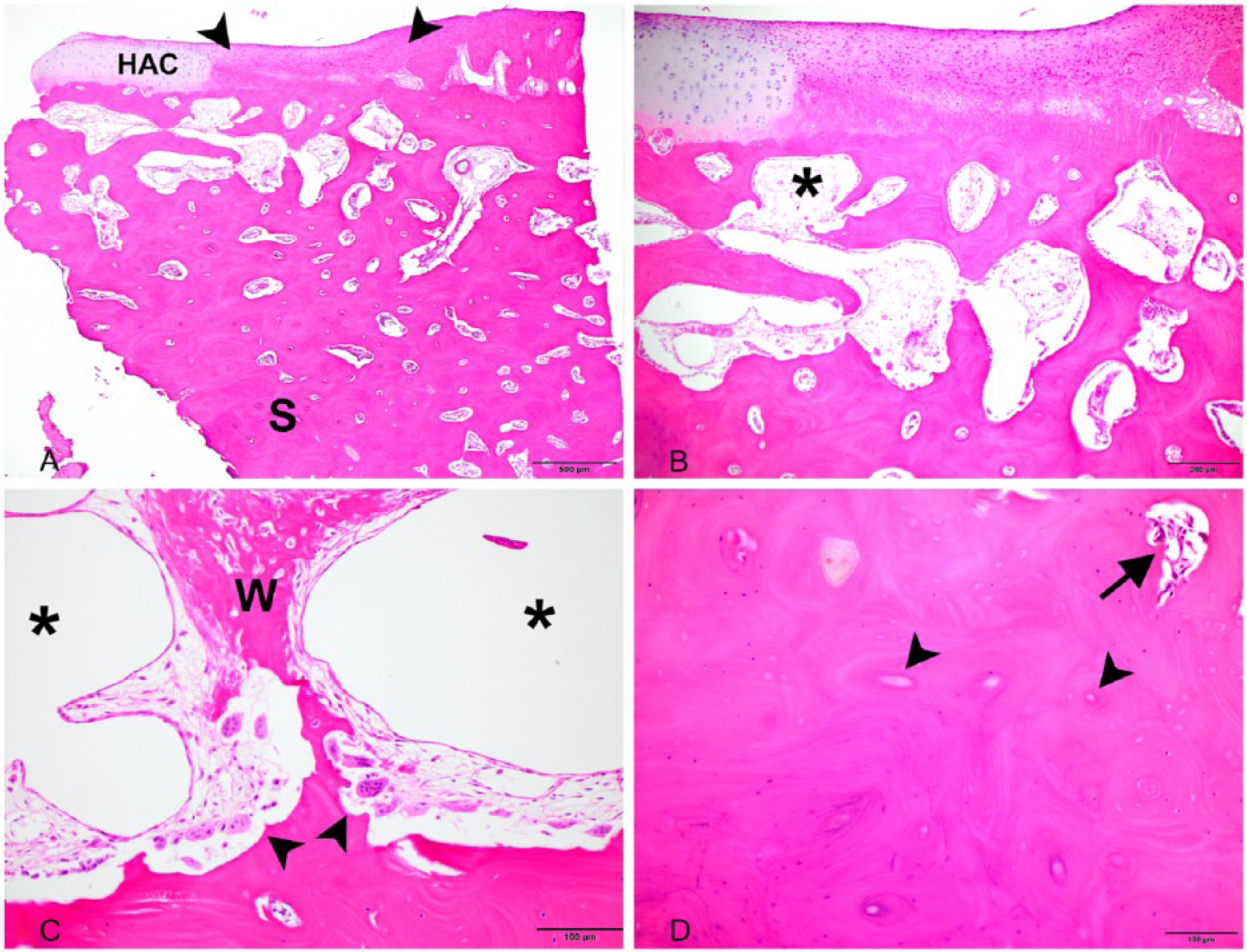
Osteochondroma composed hyaline cartilage (top) that caps outer compact and inner trabecular bone. This lesion was surgically excised from a mature animal, evidenced by complete closure of the growth plate. Safranin-O. Bar = 500 μm.
Septic arthrosynovitis and tenosynovitis
Septic arthrosynovitis or tenosynovitis of the carpal region can arise from hematogenous spread or introduction of bacteria into the joint or synovial sheath through a penetrating wound or iatrogenic injections and surgical procedures (Figs. 5, 6). In a study of 192 horses diagnosed with septic synovitis involving at least 1 synovial structure (joint or tendon sheath), 45 (18.4%) involved the carpus with 50% associated with surgery, 15.9% associated with iatrogenic injection, 4.3% associated with a penetrating wound, and 8.3% idiopathic. 69 In this study, the carpus was the most frequently infected structure postoperatively, and the third most frequently affected structure post-injection preceded by the tarsus and fetlock. Most common isolates comprised gram-positive bacteria (e.g., nonhemolytic and hemolytic Staphylococcus spp., beta-hemolytic and non–beta-hemolytic Streptococcus spp.) and gram-negative bacteria (e.g., Enterobacteriaceae family, Escherichia coli, and Pseudomonas spp.) with no bacteria isolated in 27% of cultures. 69 Septic arthrosynovitis or tenosynovitis is associated with joint or tendon sheath effusion and, with the exception of young foals, typically manifests as stiffness and reluctance to move, and severe lameness; pyrexia was observed in 54% of adult horses. 69 Synovial fluid in infected joints has reduced viscosity with increased turbidity, coinciding with fibrin and suppurative exudates, and can be yellow to orange-red or brown depending on whether hemarthrosis is present. The molecular inflammatory responses include production of prostaglandin-E2, matrix metalloproteinases, and proteoglycans that result in biochemical and biomechanical alterations with enzymatic degradation of the articular cartilage.44,53,66 Typical postmortem changes to intrasynovial structures include diffuse synovial hyperplasia and hyperemia, often with mats or strands of fibrin packed into synovial recesses, adhering to, or spanning the cartilage and synovial membranes. Articular cartilage also shows focal-to-diffuse yellowing and thinning, representing degeneration and atrophy, with ulcers and osteomyelitis extending into the subchondral bone (Fig. 6). Prolonged inflammation within the carpal sheath can result in “carpal canal syndrome,” a painful entrapment neuropathy that results from chronic effusion, whether the result of sepsis or trauma associated with distal radial osteochondromata, caudal radial physeal exostoses, carpal hyperextension injuries (with or without accessory carpal bone fractures), and injuries of the superficial or deep digital flexor tendons. 17
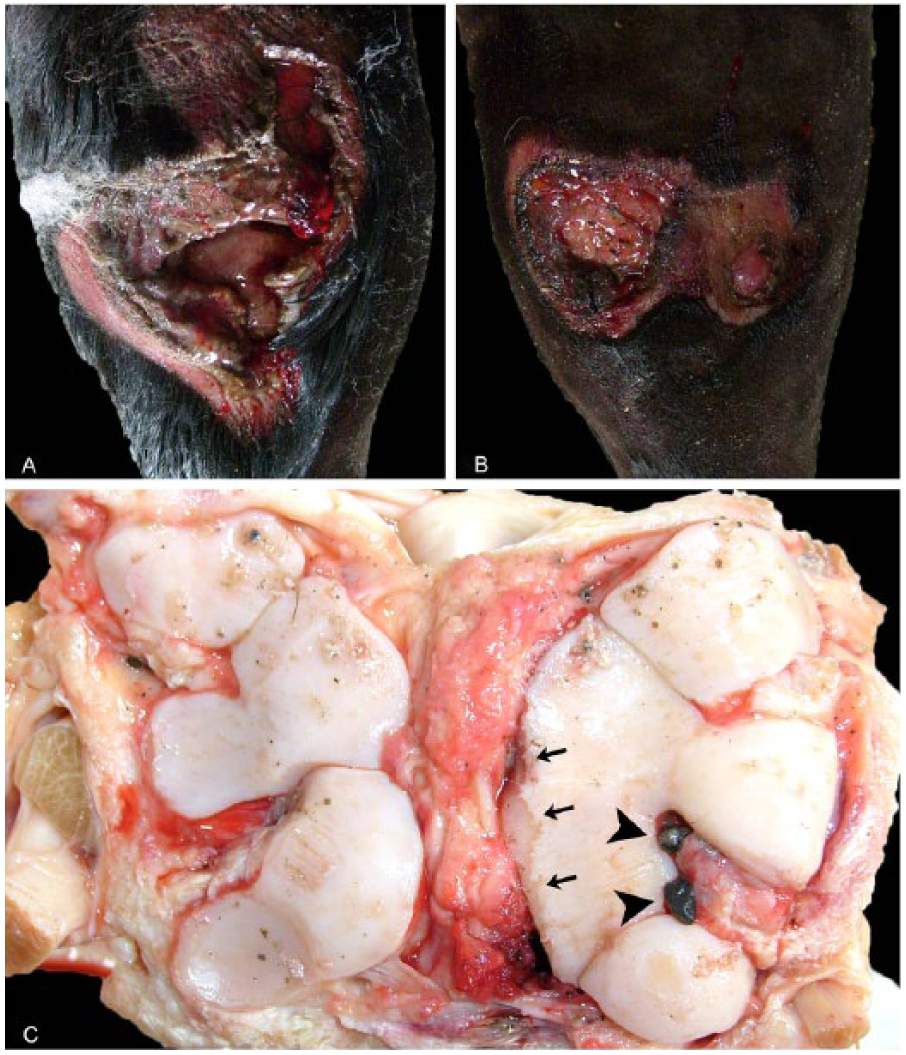
Septic carpi from a carriage horse that sustained an accident while driving in-hand.
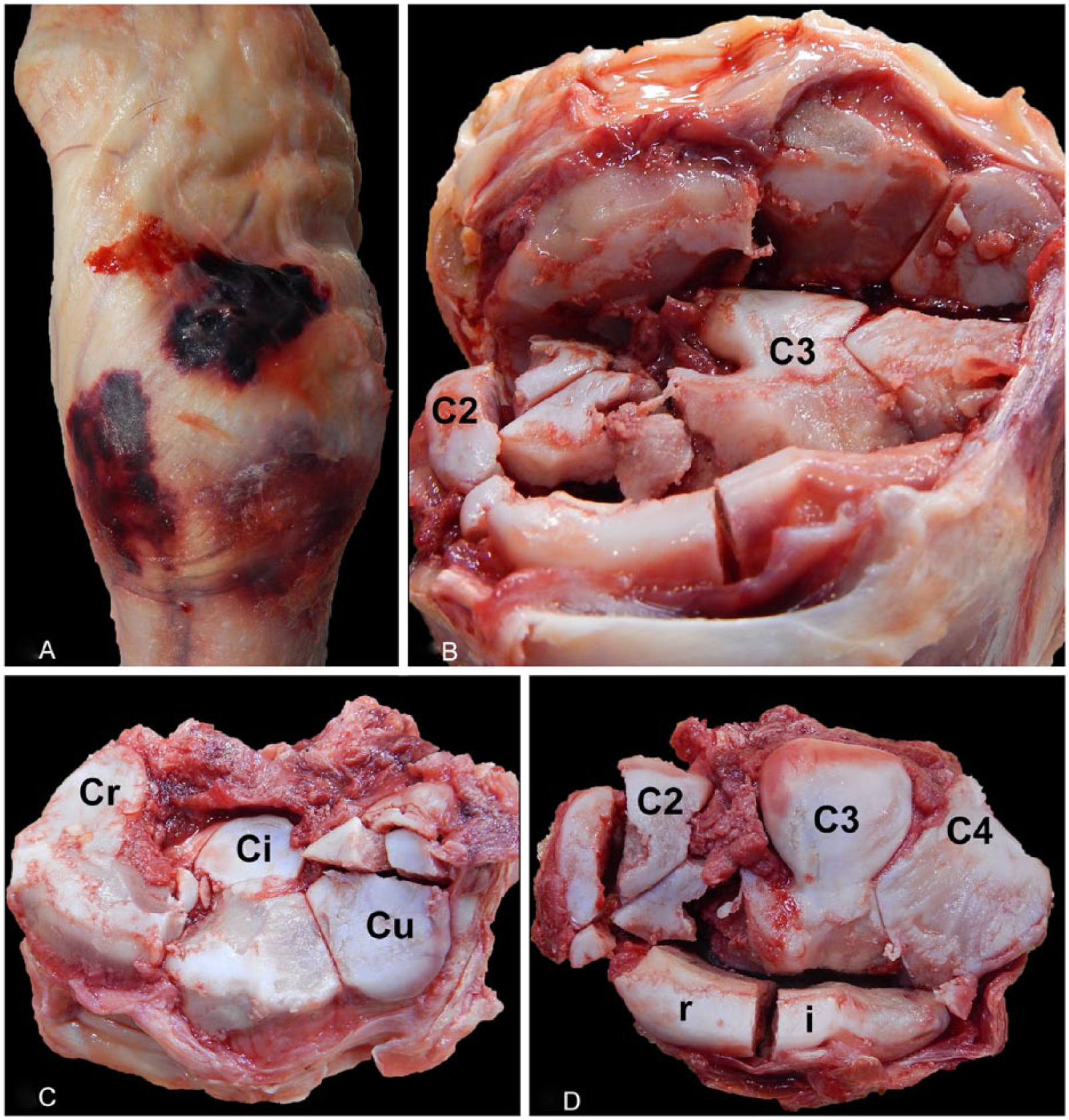
Disarticulated proximal and distal rows of carpal bones from a Thoroughbred racehorse that developed septic arthritis in the right middle carpal joint after having bilateral arthroscopic surgery to excise osteochondral “chip” fragments (
Degenerative osteoarthritis
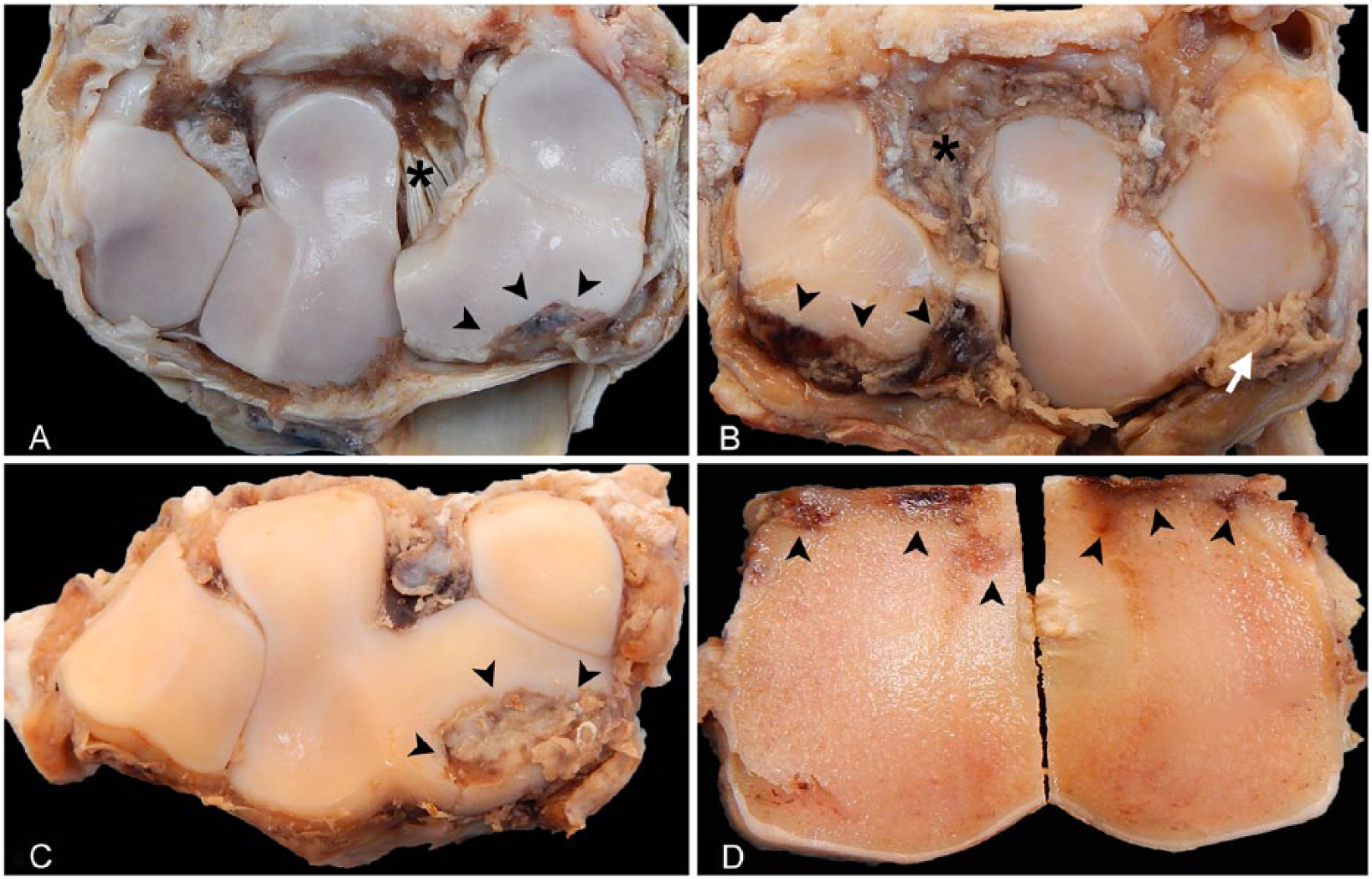
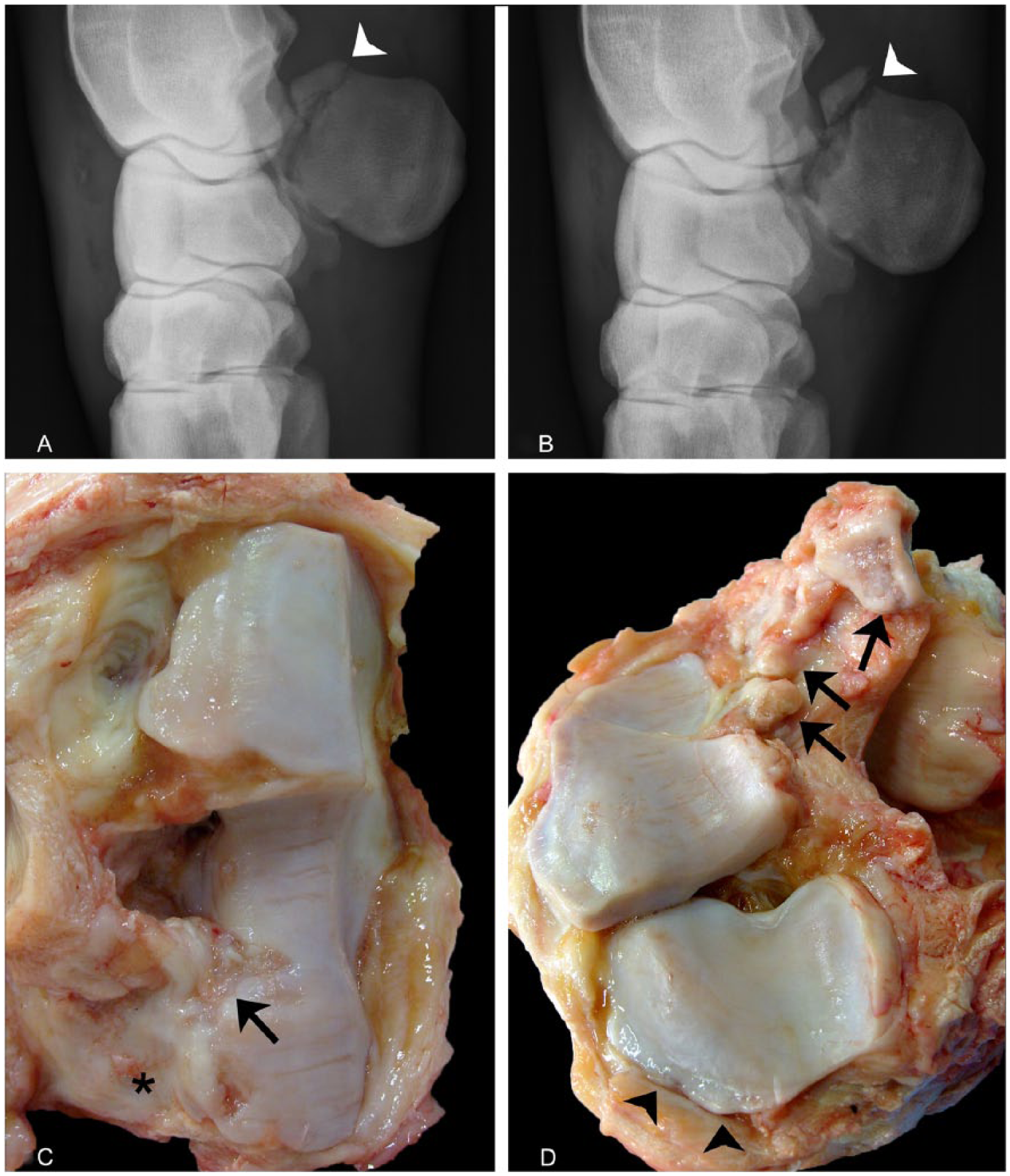
Although inflammation from sepsis is highly destructive to joints and synovial structures, rapidly advancing secondary degenerative changes can occur from prolonged non-septic inflammatory changes. “Spontaneous” degenerative osteoarthritis of the CMC joint (e.g., carpal spavin) predominantly occurs in older (>8 y old), non-racing Quarter Horses and Arabian horses, and has a guarded-to-grave prognosis given insidious yet severe, progressive narrowing of the medial aspect of the CMC joint space with osteolysis, bridging osteophytosis, periarticular soft tissue thickening, and effusion. 56 In contrast, most cases of degenerative carpal osteoarthritis occur in racehorses (Fig. 7). Thought to occur secondary to non-physiologic, repetitive loading of the carpal bones associated with poor anatomic conformation or perhaps certain training and racing practices, this “traumatic” form of osteoarthritis may produce abnormal remodeling and function of articular cartilage, subchondral bone, and synovium that lead to osteochondral fragmentation (Fig. 8) and eventual joint failure.1,36,90 With severe joint instability, chronic degeneration and progressive osteophytosis can result in “end-stage” osteoarthritis with partial-to-complete bridging ankylosis (Fig. 9). In addition to racehorses, non-equine athletes including humans and racing greyhounds experience repetitive post-traumatic osteoarthritis, manifesting, in advanced cases of degenerative osteoarthritis, as joint effusion with reduced viscosity of synovial fluid; synovial membrane hyperplasia and joint capsule fibrosis; articular cartilage fissures, erosions, and atrophy; and subchondral sclerosis, lysis, fracture, and osteophytosis.1,9,16,36
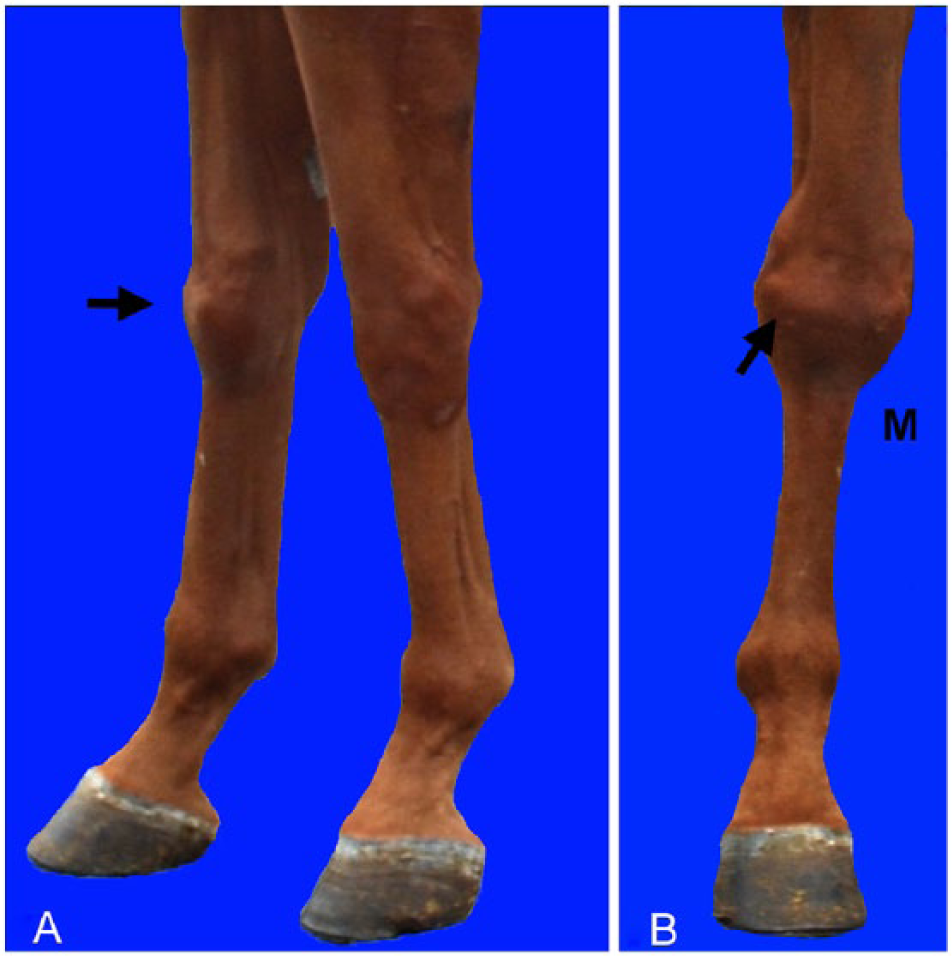
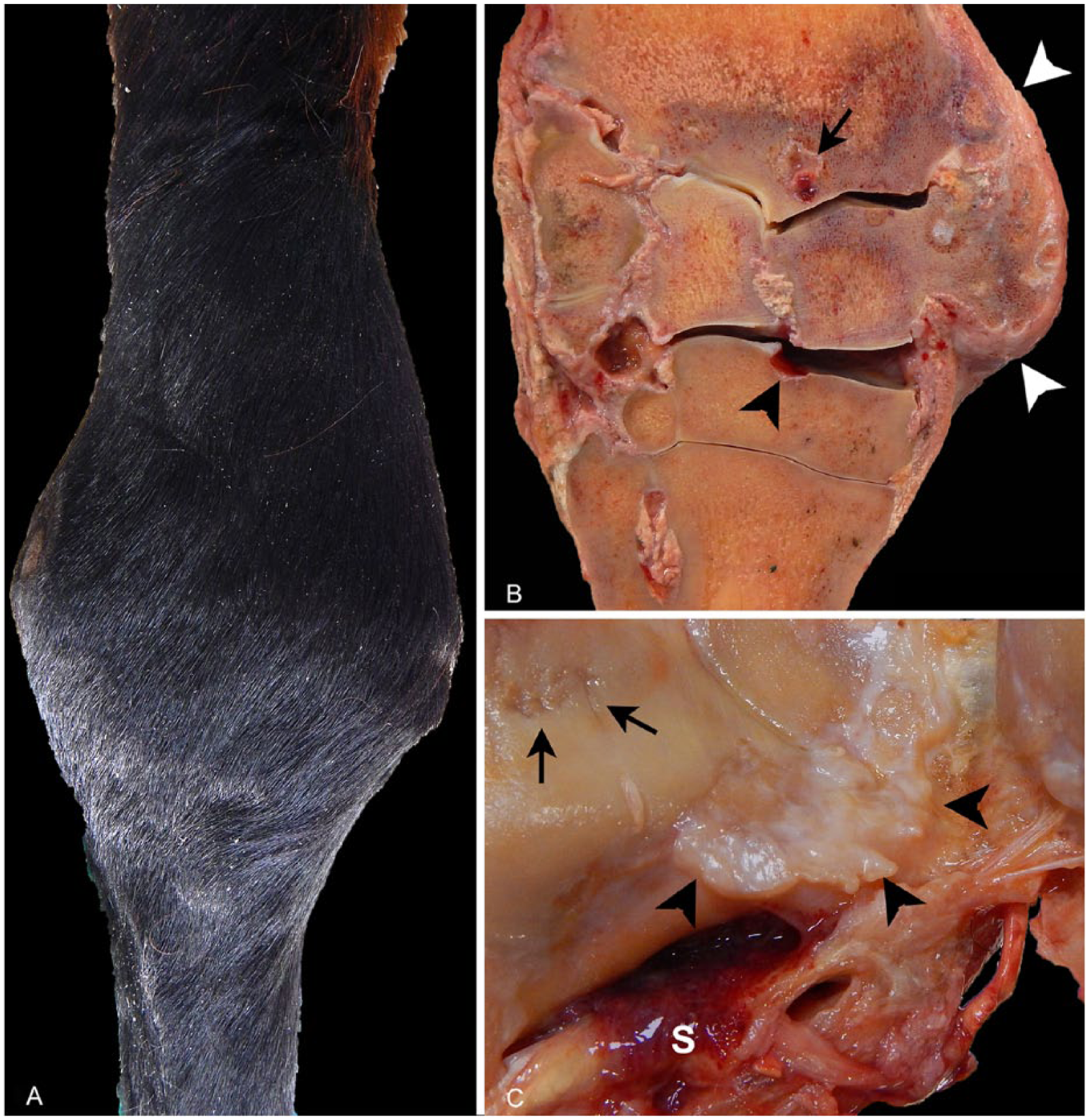
Chronic degenerative osteoarthritis in the right carpus of a Thoroughbred racehorse euthanized for severe intractable lameness of 1-mo duration. Antemortem photos show a bulging profile (arrows) seen dorsally
A collaborative initiative developed a standardized grading scheme, based on modified Mankin and OARSI (Osteoarthritis Research Society International) scoring systems, for characterization of macroscopic and microscopic lesions associated with experimental or naturally occurring osteoarthritis in horses. 41 Schemes were designed to assess all components of the joint, including lesions identified in the synovium (inflammatory infiltrates; hyperplasia; edema; and fibrosis), cartilage (superficial, partial to full-thickness erosions; fibrillation and fissures; chondrocyte necrosis and loss; chondrone formation; and changes to the extracellular matrix), and subchondral bone (splitting of the osteochondral matrix; subchondral bone disruption and collapse; and subchondral bone remodeling). 41 Although not necessary for routine postmortem exams, use of these schemes will provide meaningful comparisons among laboratories as well as experimental or naturally occurring osteoarthritis models.
Experimental induction of osteoarthritis has been achieved in horses by intra-articular injection of recombinant equine interleukin-1 beta or iatrogenic intra-articular osteochondral fragmentation and exercise. These established models of osteoarthritis allow the investigation of associated inflammatory profiles, assessment of biomarkers related to degeneration and remodeling, and better characterization of clinical and imaging parameters.26,36,66 Studies of naturally occurring osteoarthritic disease in racing Standardbreds did show correlation between advanced gross and microscopic lesions in the articular cartilage and subchondral bone, including erosions and loss of proteoglycan content within hyaline cartilage, cracks and collapse within mineralized cartilage, and subchondral bone pits with porosity correlating with lesion-specific increases in osteoclasts and volumetric decreases in bone density as determined by microcomputed tomography (micro-CT).10,39 Re-examination of the original micro-CT scans revealed acellular, high-density mineralized material that form patches below and protrusions above the mineralizing front of the mineralized cartilage in osteoarthritic C3. 40 These findings, which are not visible in demineralized preparations, standard radiography, or CT, coincide with similar high-density mineral protrusions identified within distal palmar/plantar third metacarpi/metatarsi of Thoroughbred racehorses in association with palmar/plantar osteochondral disease, that extend through vertical cracks within the articular mineralized cartilage, and microcracks within the subchondral bone and osteochondral junction in human osteoarthritic joints.13,23,46,82 A separate study in a different set of samples confirmed the presence of similar extruded mineralized matrix extending from cracks in the calcified cartilage into the deeper regions of hyaline cartilage, corresponding to sites of superficial hyaline cartilage erosion and fibrillation. 31 Other studies performed in carpal bones of both Thoroughbred and Standardbred racehorses identified subchondral bone sclerosis with increased mineral density, and increases in biochemical markers of bone turnover, corresponding to gross and histologic lesions of cartilage degeneration and osteoarthritis.22,79
Additional studies attempting to mimic early stages of “naturally occurring” repetitive impact trauma induced by conditioning exercise in 1.5–2-y-old Thoroughbred fillies showed significantly higher bone mineral density in C3, 24 as well as mechanical and morphologic differences in the hyaline and mineralized articular cartilage within sites that withstand high intermittent loads (e.g., dorsodistal Cr and Ci, and dorsoproximal C3).31 48,49 Yet a different study performed in young juvenile Thoroughbreds comparing the effects of pasture exercise versus controlled, conditioning exercise instituted from birth through 18 mo of age on opposing surfaces of cartilage and subchondral bone taken from Cr and C3 identified gross and histologic lesions involving osteochondral junctions and mineralized cartilage within both exercised and control groups, thus suggesting that “early” microscopic osteochondral lesions (e.g., localized disruption of the osteochondral junction, thickening of the mineralized cartilage with matrix texture changes and microcracks) may arise within sites predisposed to developing more advanced osteoarthritis, regardless of exercise program.37,38 Although much more is known regarding lesions associated with the development of equine osteoarthritis, clearly the results of the studies listed above incite additional questions necessitating further research into the predisposition and pathogenesis of equine osteochondral disease.
Osteochondral fragmentation and catastrophic carpal fractures
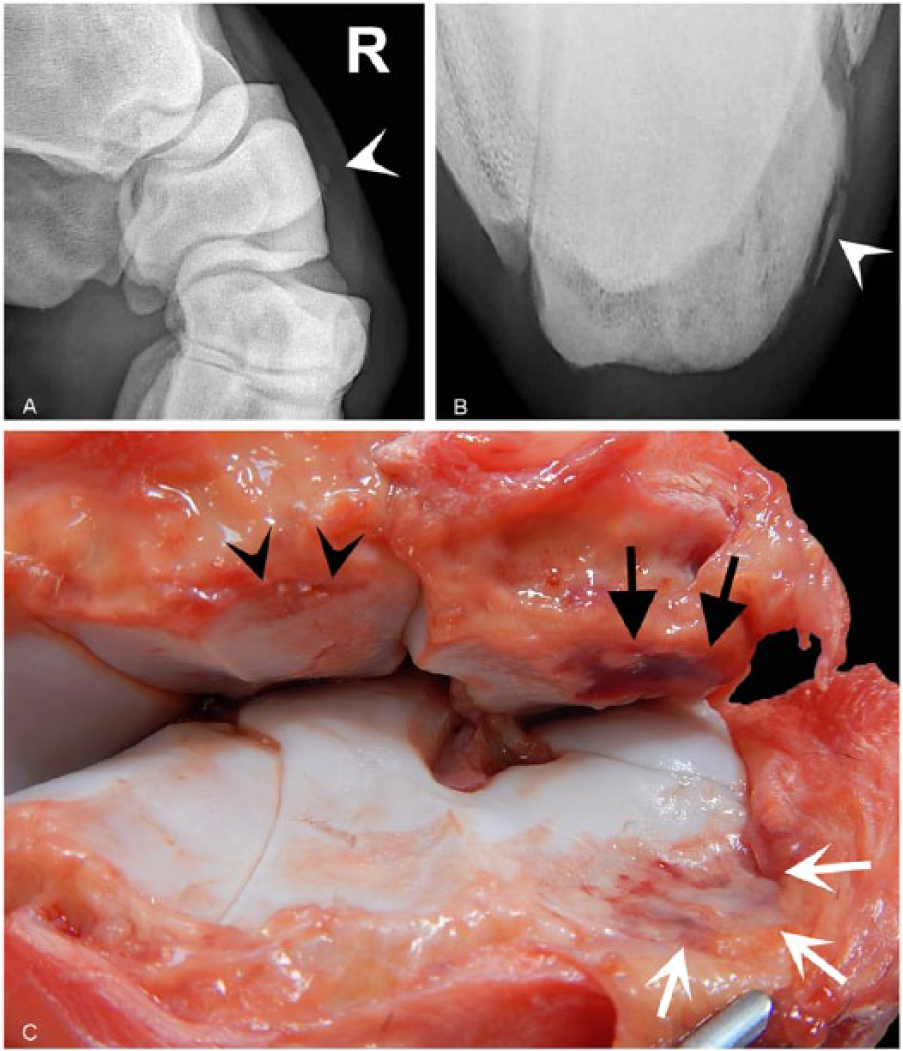
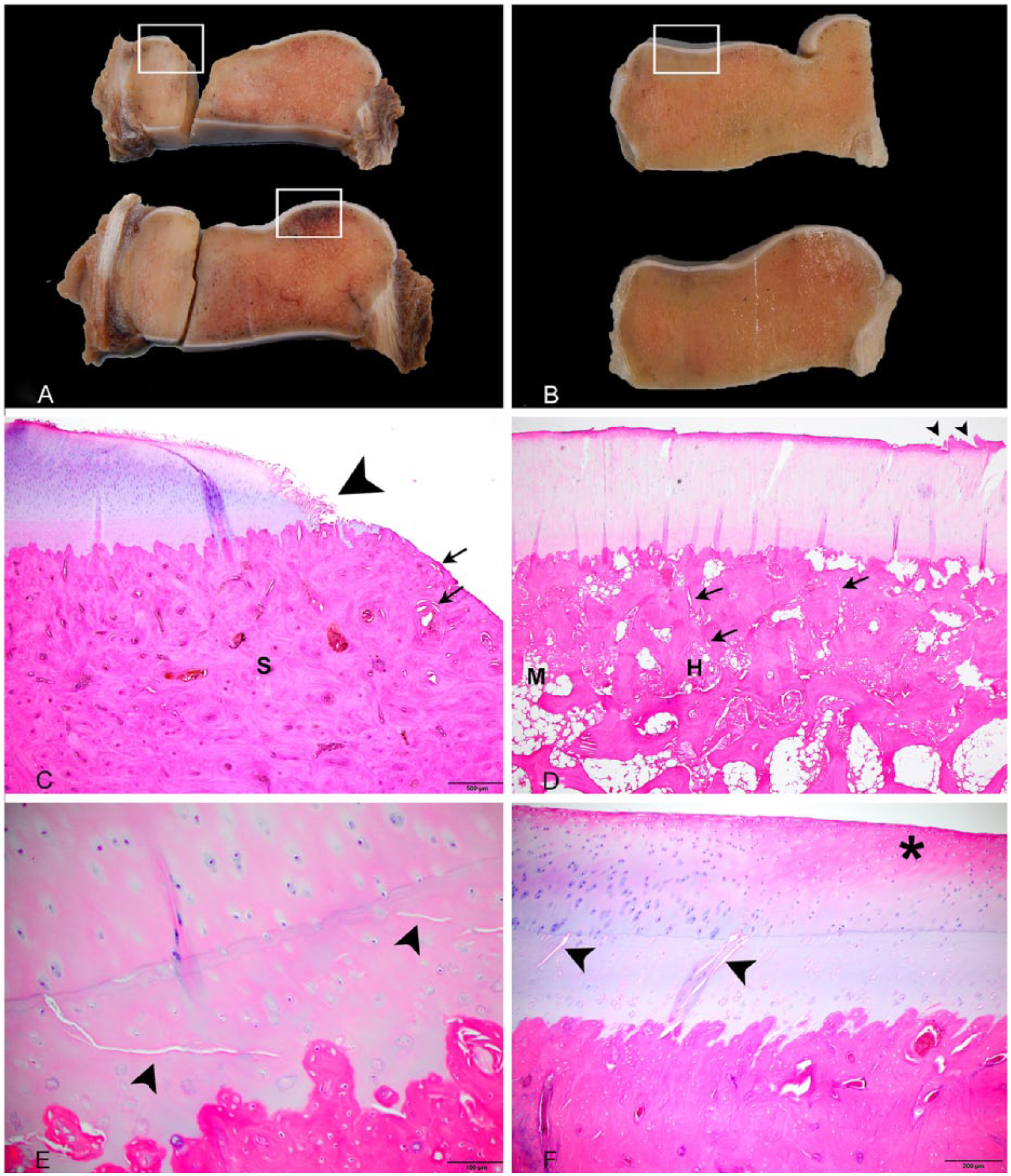
In conjunction with degenerative osteoarthritis, osteochondral fragmentation (i.e., fracture) of the equine carpus results from naturally occurring, repetitive impact trauma associated with racing and training. This lesion occurs most frequently in the middle carpal joint along the dorsodistal margin of Cr and dorsoproximal margin C3, followed by the antebrachiocarpal joint along the dorsolateral margin of the distal radius and dorsoproximal margin of Ci.42,55,68,76 In both Thoroughbred and Standardbred racehorses, early degenerative changes (e.g., subchondral sclerosis and lucency) associated with carpal lameness are thought to precede cartilage damage and fractures.29,32,65,80 However, experimental osteochondral fragmentation will induce subchondral bone remodeling and changes in the mineralized cartilage layer. 52 Osteochondral fragments involve a single articular surface of a bone (so-called “chip” fractures) or span 2 articular surfaces of a bone (bi-articular or “slab” fractures; Figs. 8, 10, 11). Depending on their location and size (“large” or “small”), chip fractures can be surgically removed, reduced with surgical implants, or treated conservatively with prolonged stall rest. 76 Although breed and activity (i.e., type of racing) does influence differences in fracture type and predilection site, sex does not influence lesion site or lameness.19,61,68
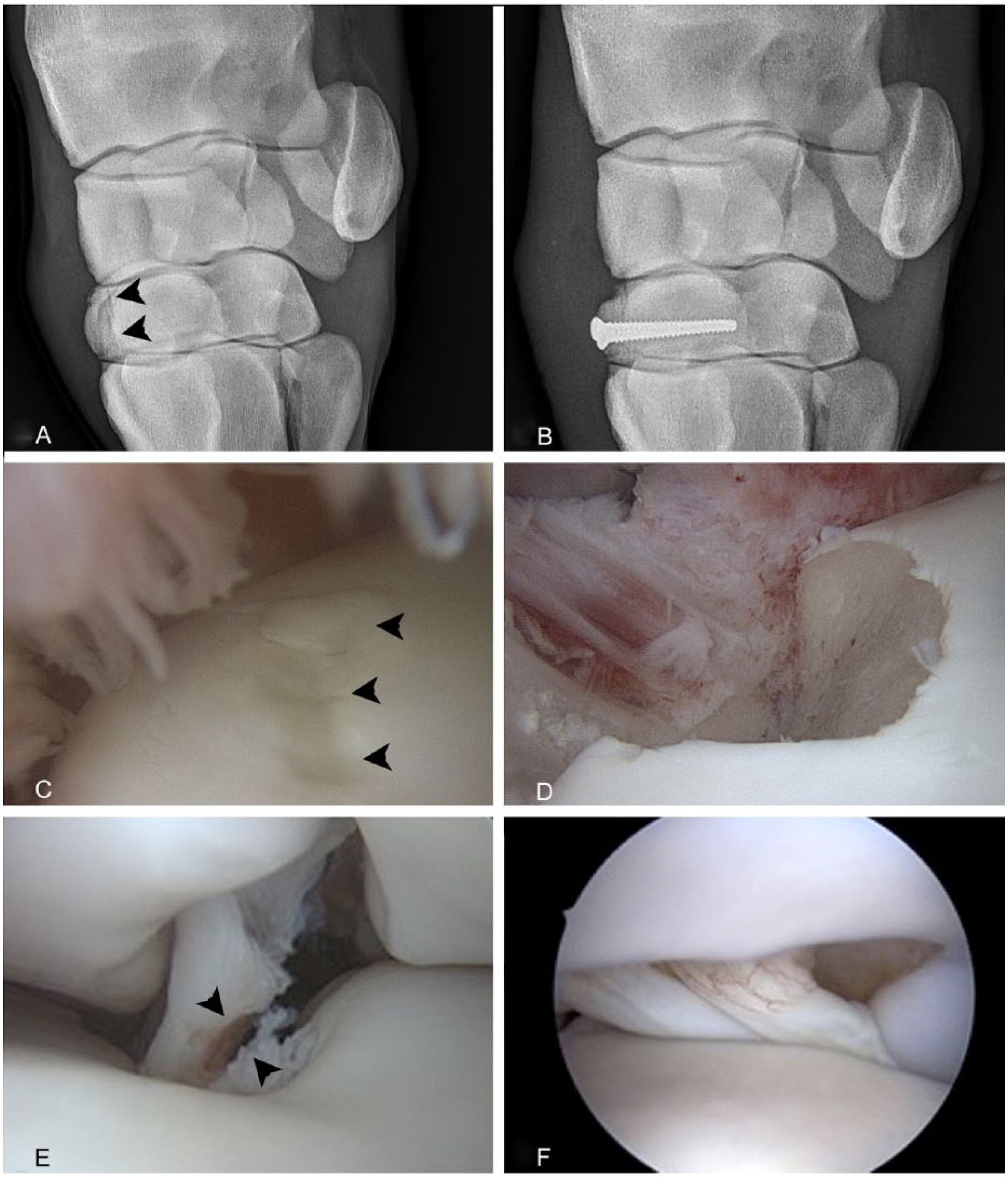
Recently, carpal fracture was reported to be the most common fatal musculoskeletal injury in racing Quarter Horses. 8 In racehorses, most fractures occur in young (<4 y old), skeletally immature animals, and although fractures in Thoroughbreds involve the right forelimb more often than the left, fractures in Standardbreds tend to be equally distributed between right and left forelimbs, and are also more frequently bilateral.68,76,89 The different site predispositions between these 2 breeds may be related to differences in gait (gallop vs. pace or trot) as well as other differences in training or racing. C3 fractures (Fig. 10) comprise incomplete or complete chip fractures and bi-articular slab fractures with the vast majority occurring in the frontal plane, a few occurring in the sagittal plane, and most involving the radial over the intermediate facet. 76 C3 fractures (Fig. 8) often occur in conjunction with fractures of opposing articular surfaces (e.g., the dorsodistal margins of the radiocarpal or intermediate carpal bones). 68
Fractures in other carpal bones (Cu, C2, C4, and Ca) are unusual, either associated with catastrophic fractures (e.g., “breakdown injuries”) that result in severe destabilization of the joint necessitating euthanasia34,57,77 (Figs. 12, 13) or occurring sporadically as the result of trauma from falls or kicks. 64 Catastrophic carpal fractures are reported in racing Thoroughbreds and Quarter Horses, but are extremely rare and not well reported in Standardbred racehorses (Drs. PM Hogan and MW Ross, pers. comm., 2016), again possibly reflecting differences in maximum racing speed and gait differences. 11 Although there are a few reports describing palmar osteochondral fragments, they rarely occur as primary lesions, and fragments within the palmar aspect of the antebrachiocarpal or middle carpal joint are often associated with primary lesions involving dorsal aspects of other carpal bones (e.g., Cr, C3, Ci, Ca, Cu) or the distolateral margin of the radius. 27 Accessory carpal bone fractures are rare (2% of all fractures) but well-recognized lesions that often result from extreme hyperextension associated with jumping or a fall, or other severe trauma to the palmar aspect of the carpus.12,45 Fractures often occur as a proximodistal slab in the frontal plane, and can involve the carpal sheath or traumatize the deep digital flexor tendon.12,45 Articular Ca fractures are often comminuted and, if not surgically removed, can result in significant instability of the antebrachiocarpal joint, and horses are at risk of secondary osteoarthritis and intractable lameness 12 (Fig. 14).
In addition to osteochondral fragmentation, stress-related injuries to associated ligaments and tendons can occur alone, or in conjunction with osteochondral fragmentation, leading to further joint instability and degenerative osteoarthritis. 39 Damage to the medial palmar intercarpal ligament (Fig. 10E, 10F) is common in horses >1 y of age, with tears tending to be more severe in Standardbreds than Thoroughbreds. 86 Avulsion fractures of the lateral palmar intercarpal ligament originating from the medial palmar aspect of the ulnar carpal bone are described as radiographically and histologically distinct from subchondral cystic lesions of the ulnar carpal bone mentioned above. 6
Footnotes
Acknowledgements
We thank Drs. Patty M. Hogan, Dean W. Richardson, and Michael W. Ross for contributing clinical materials, images, and or constructive comments to this manuscript. We also thank Ms. Karie Durynski for her excellent technical skills and efforts in producing materials used for imaging in this manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.