
Abstract
We characterized features of complete diaphyseal fractures of third metacarpal bones in Thoroughbred racehorses. Given that stress fractures are known to occur in the third metacarpal bone, an additional aim was to determine if complete fractures are associated with signs of a preexisting incomplete stress fracture. Bilateral metacarpi from 12 Thoroughbred racehorses euthanized because of complete unilateral metacarpal diaphyseal fracture were examined visually and radiographically. Open, comminuted, transverse or short oblique fractures occurred in the middle of the diaphysis or supracondylar region. Periosteal surface discoloration and bone callus formation contiguous with the fracture line were present in fractured bones. All contralateral intact metacarpi had gross anatomic lesions, and 10 had radiographic abnormalities similar to those observed on fractured metacarpi. Catastrophic metacarpal fractures occurred in racehorses with bilateral evidence of preexisting bone injury.
Introduction
Third metacarpal bone (MC III) injuries are a common cause of lameness, poor performance, and time out of training for young racehorses.5,18 Complete diaphyseal MC III fractures are uncommon. 6 Fracture of MC III has been documented as a cause of severe or fatal musculoskeletal injury.1,7,8,10,13,17 Catastrophic MC III fractures accounted for 5% of Quarter Horse 17 and 3% of Thoroughbred and Quarter Horse 10 racing- and training-related musculoskeletal fatalities in California, and 20% of Thoroughbred and 10% of Quarter Horse catastrophic injuries in the midwestern United States. 1
Transverse fractures of the distal portion of the diaphysis have been described in 6 racehorses, 14 and incomplete oblique sagittal fractures of the dorsal cortex were reported in 6 racehorses. 20 Although the pathogenesis of metacarpal bone fractures remains hypothetical, there is evidence that catastrophic fractures in racehorses are not spontaneous events, but are the end stage of a series of events associated with bone damage and repair, recognized as stress fractures. 16 An association of complete fractures with dorsal cortical stress fractures has been suggested.6,14 Callus formation was associated with incomplete distal diaphyseal transverse fractures. 14 The MC III is one of the bones most commonly affected by stress fractures. 19 Further, racehorses entering training are commonly affected with inflammation of the dorsal cortex of MC III (dorsal metacarpal disease or “bucked shins”) when high-speed work is initiated (Norwood GL. Bucked-shin complex in Thoroughbreds. Proc Ann Conv Am Assoc Equine Pract 1978;24:319–336). 15 A proportion of these horses subsequently develop dorsal cortical stress fractures.4,9
We characterized the features of MC IIIs that sustained a catastrophic diaphyseal fracture. Because incomplete stress fractures occur in the middle and distal diaphyseal regions of the MC III of racehorses without overt external trauma, we hypothesized that complete diaphyseal MC III fractures in racehorses would occur in association with evidence consistent with preexisting stress fracture.
Materials and methods
A convenience sample of bilateral MC IIIs from 12 Thoroughbred racehorses (2–5 y of age; 7 female, 5 male) that were euthanized because of a unilateral complete diaphyseal MC III fracture (7 left, 5 right) at California racetracks from 1994 to 2011 were studied. Bilateral metacarpal bones were manually debrided of soft tissues and examined for cortical discoloration and periosteal bone proliferation. Cortical bone surface discoloration (none, petechiae-like, diffuse, widespread), texture (smooth, rough), and periosteal bone proliferation (none, <3 mm diameter and <3 mm depth, >3 mm in diameter or depth) were tabulated for fractured and contralateral (intact) bones. Location of the periosteal proliferation was measured from the distal extent of the distal articular surface.
Bones were radiographed (56 kVp, 5.4 mAs, 30 cm film distance) using a portable generator (TR90 Tough Ray, MinXray, Northbrook, IL) and flat panel digital radiography detector (Mark III, Sound-Eklin, Carlsbad, CA). Intact bones were mounted through the proximal articular surface to a custom jig to standardize dorsopalmar (DP), lateromedial (LM), dorso45°medial palmarolateral oblique (D45M-PLO), dorso45°lateral palmaromedial oblique (D45L-PMO), dorso60°medial palmarolateral oblique (D60M-PLO), and dorso60°lateral palmaromedial oblique (D60L-PMO) views.
Radiographs were analyzed using DICOM viewing software (Efilm Workstation, Merge Healthcare, Chicago, IL). The contralateral intact limb was assessed for the presence or absence of periosteal proliferation, cortical radiolucencies, and endosteal bone proliferation. When present, periosteal proliferation was categorized as smooth or irregular surfaced, focal or diffuse, homogeneous or heterogeneous, and less, more, or similar in density to that of the underlying cortical bone. Cortical lucency was categorized as discrete or diffuse. Radiolucent lines were categorized as incomplete or complete relative to the cortical thickness, and by proximal or distal intracortical propagation from the outer cortical surface. The distance from the most distal extent of the metacarpus to the center of the periosteal proliferation was measured where applicable. On the fractured limbs, location of the distal component of the fracture on the medial, lateral, dorsal, and palmar cortices was measured from the most distal extent of the metacarpus.
Locations of abnormalities were compared between fractured and intact contralateral bones using a paired t-test and a correlation statistic when abnormalities were present on both bones (SAS software, SAS Institute, Cary, NC). P values ≤ 0.05 were considered to be statistically significant.
Results
Fractures occurred in the distal diaphyseal (supracondylar) region only (3 bones), middle of the diaphysis (mid-diaphysis) only (3 bones), or in both supracondylar and mid-diaphyseal regions (6 bones; Figs. 1, 2). Horses had a transverse (5), short oblique (4), long oblique (1), or combination of transverse and short oblique fractures (2). The 3 supracondylar fractures had a transverse configuration with an oblique component through the dorsal cortex (Fig. 1), whereas the 3 mid-diaphyseal–only fractures were highly comminuted with an oblique component (Fig. 2).
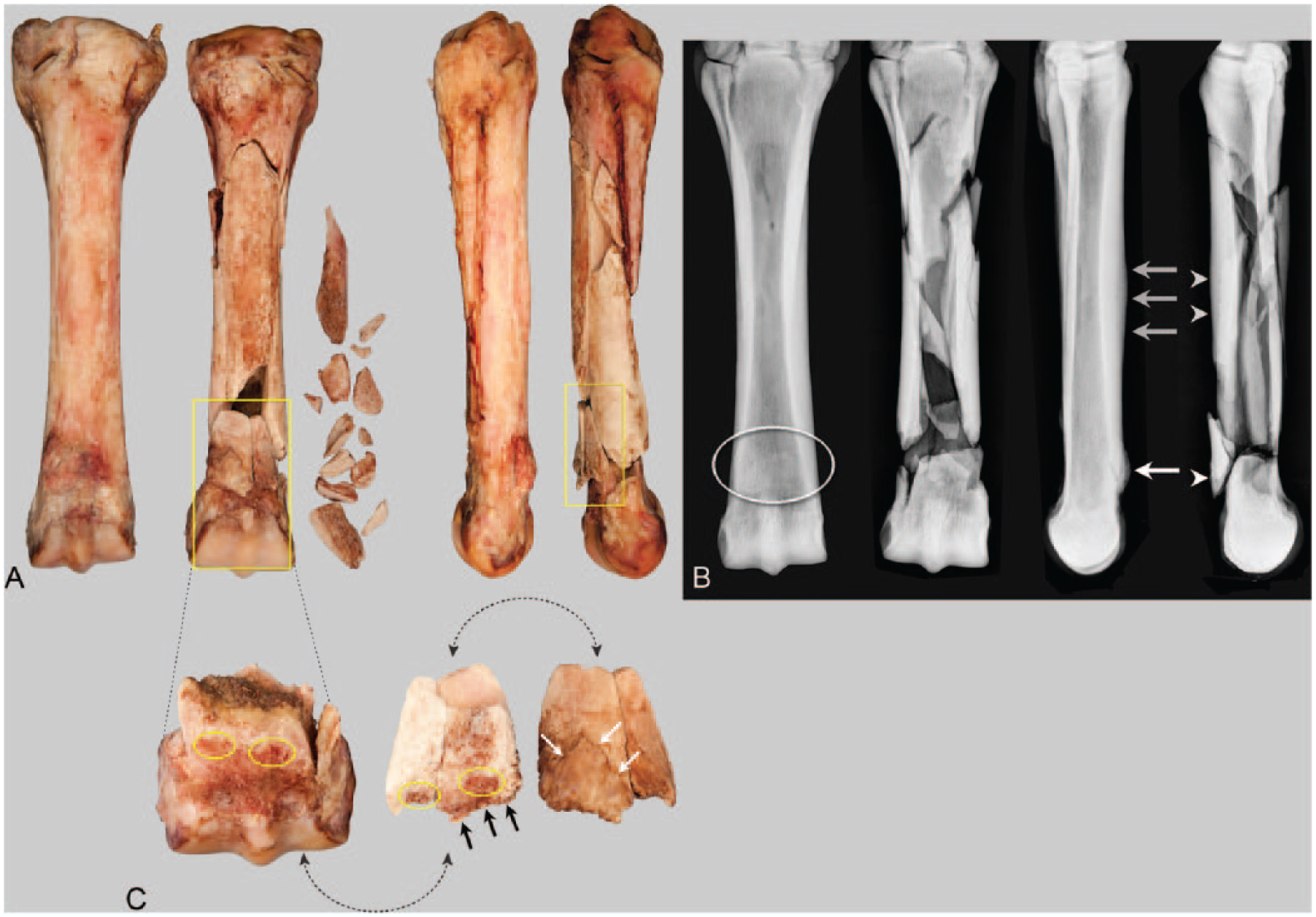
Bilateral third metacarpal bones (MC IIIs) from a 3-y-old Thoroughbred racehorse with a left forelimb metacarpal bone fracture. (
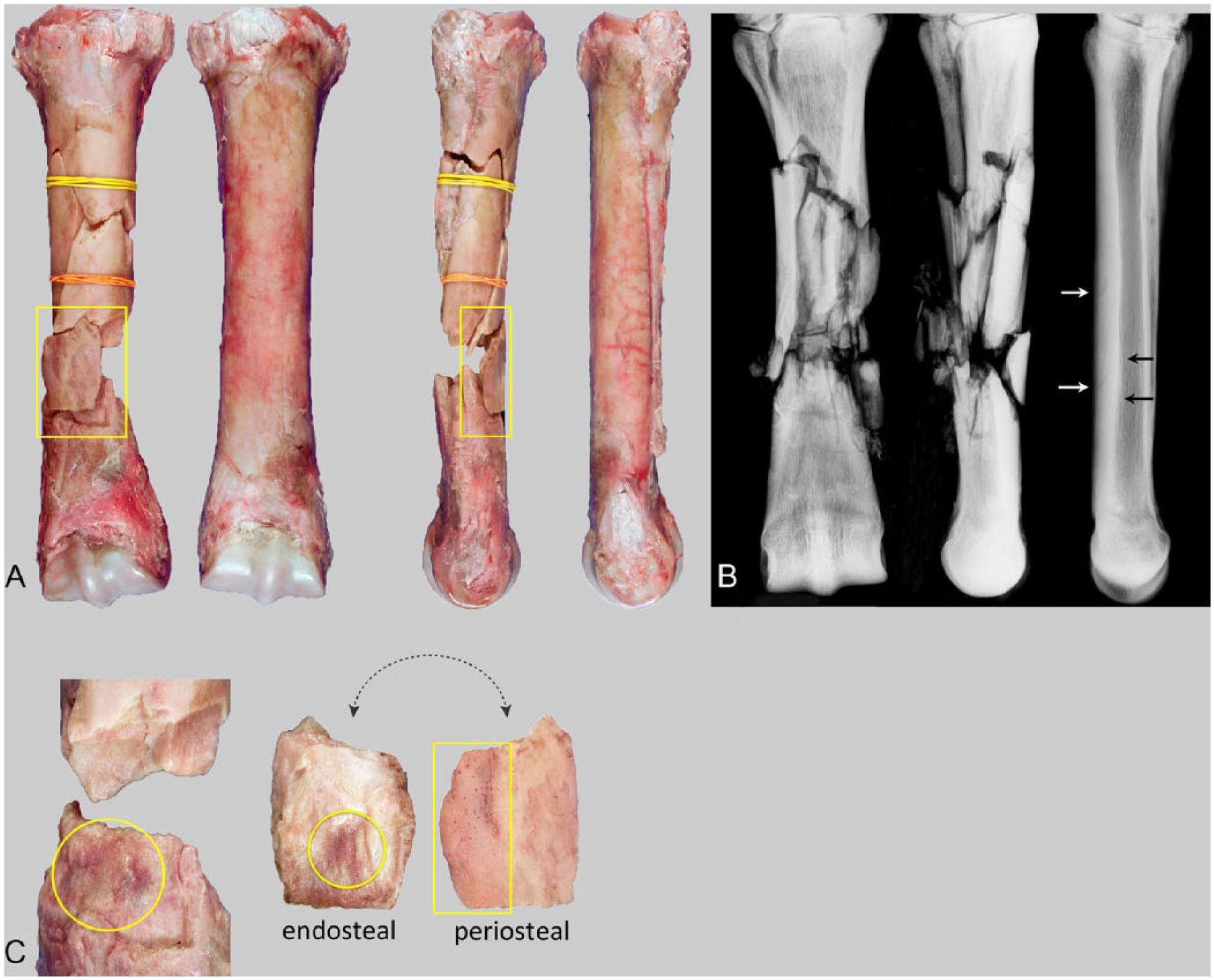
Bilateral third metacarpal bones (MC IIIs) from a 4-y-old Thoroughbred racehorse with a right forelimb metacarpal bone fracture. (A) Dorsal (left) and medial (right) views illustrate a unilateral comminuted fracture of the middle of the diaphysis of the right forelimb MC III. (B) Dorsopalmar radiographic projection of the fractured bone, and lateromedial radiographic projections of the fractured and intact metacarpal bone. The intact bone has radiolucent lines (white arrows) and endosteal sclerosis (black arrows) indicative of incomplete dorsal cortical fractures. (C) The dorsal cortical bone fragment denoted within the yellow rectangle in panel A has been removed from the distal bone fragment, and the periosteal and endosteal surfaces of the fragment are illustrated to the right. Yellow circles highlight areas of red discoloration on opposing fracture surfaces of the distal fragment and the dorsal cortical fragment. The rectangle illustrates woven bone on the periosteal surface of the fragment.
On radiography and gross examination, all fractured bones had at least 1 comminuted fragment from the dorsal cortex that had an abnormal periosteal surface, characterized by discoloration and rough-surfaced new periosteal bone (Figs. 1, 2). The cortical fracture surface on the adjacent parent bone fragment also had a focus of dark discoloration (red or brown) in 9 bones. Periosteal bone formation that altered (expanded) the shape of the periosteal surface contour (i.e., modeling) was noted on the LM radiographic projection. In 6 metacarpi, there was smooth periosteal bone formation in the proximodorsal region of the diaphysis; however, this bone formation was only associated with the fracture in 1 metacarpus. Rough-surfaced new periosteal woven bone proliferation was contiguous with the fracture gap on fracture fragments in 3 metacarpi. Periosteal modeling was identified on fracture fragments in all fractured metacarpi. All bones had rough-surfaced periosteal new bone <3 mm in depth and diameter, and 7 bones had a focal callus >3 mm in depth and diameter. Reconstruction of available fracture fragments demonstrated that periosteal modeling changes bridged the location of the fracture before fracture occurred in all cases (n = 7).
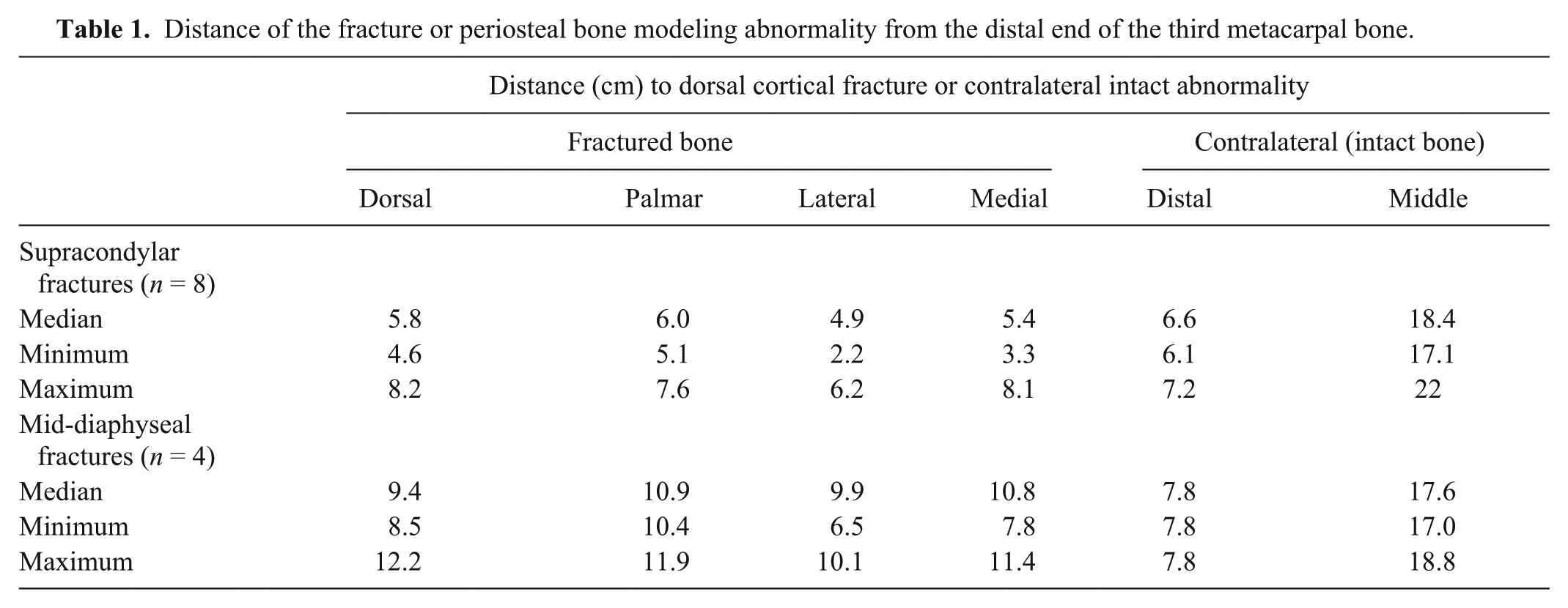
Periosteal bone production was identified in 8 intact, contralateral bones, 4 in the dorsolateral aspect of the supracondylar region, 8 in the dorsal aspect of the diaphysis (Fig. 2), and 3 in both locations. The location of supracondylar abnormalities in the intact limb was highly positively correlated (r2 = 0.92) with the location of fracture in the fractured bones (Table 1). Diaphyseal abnormalities were largely proximal or distal to those in the fractured bones (Table 1).
Distance of the fracture or periosteal bone modeling abnormality from the distal end of the third metacarpal bone.
Proximal or middle diaphyseal abnormalities in intact, contralateral bones were smooth- (8 bones) or irregular- (1) surfaced, focal (3) or diffuse (6), homogeneous (8) or heterogeneous (1), less dense (5) or of similar density (4) to the underlying cortical bone. Cortical lucencies were present in 4 bones. One of these bones had 2 discrete dorsoproximal-oriented incomplete cortical linear lucencies associated with 2 focal, smooth-surfaced, homogeneous sites of periosteal modeling in the dorsal aspect of the cortex. This bone also had evidence of endosteal proliferative bone production.
Focal calluses, present on the dorsal cortex of the supracondylar region of 4 intact, contralateral bones, were >3 mm in width and depth and characterized by red, irregular-surfaced, new periosteal woven bone. The periphery of all 4 calluses had a thin layer of rough-surfaced, discolored new bone production. One additional bone had an irregular bone surface in the same location, without a discrete callus. Diaphyseal bone modeling was evident as smooth-surfaced dorsal cortical expansion in 6 bones (2.5–4.4 cm long regions). The periosteal surface was red or dark brown in all bones, with rough-surfaced new bone evident in 3 bones.
Discussion
All fractures in this case series were open and comminuted, with missing fragments. Two fracture configurations were apparent: comminuted transverse or short oblique supracondylar fractures, and more highly comminuted short or long oblique mid-diaphyseal fractures. Both fracture configurations were associated with dorsal cortical periosteal new bone formation, suggestive of preexisting bone injury. Eleven horses had abnormalities in the contralateral, intact bones that mirrored preexisting changes in the fractured bones. Bilateral findings are consistent with repetitive overuse injuries (i.e., injuries caused by repetitive cycles of high-load events) and catastrophic fracture of the most severely affected limb.
All supracondylar (distal diaphyseal) fractures in our study had findings consistent with a preexisting stress fracture. Periosteal callus had bridged the dorsal surface of proximal and distal fracture fragments. The supracondylar fractures were similar in location and configuration to the complete, non-displaced, transverse fractures in 6 young Thoroughbred racehorses that were attributed to a stress fracture etiology. 14 Half of the horses with supracondylar fractures had evidence of periosteal modeling in a similar location on the contralateral intact limb. The bilateral distribution of the findings is consistent with injuries caused by repetitive cycles of high-load events.
Mid-diaphyseal fractures in our study also had findings consistent with preexisting injury. Evidence for diaphyseal initiation of fracture was the presence of woven bone callus on the periosteal surface of fracture fragments. Periosteal abnormalities included diffuse discoloration and roughening consistent with highly vascular new woven bone. In some cases, new bone was superimposed on a larger region of smooth dorsal cortical expansion consistent with a recent exacerbation, or re-exacerbation, of dorsal metacarpal disease (bucked shins). Diffuse periosteal change associated with incomplete dorsal cortical oblique sagittal fractures was also recognized in 6 Thoroughbred racehorses. 20 The distodorsal-to-proximopalmar oblique nature of the cortical fracture surface in our study is similar to the dorsal cortical fractures reported in 53 Thoroughbred racehorses. 3
Detection and management of horses that could be at risk for catastrophic metacarpal fracture is difficult. Mid-diaphyseal and supracondylar fractures occur at sites that undergo adaptation in response to increasing intensity of racehorse training. Dorsomedial metacarpal expansion is well documented in Thoroughbred racehorses that transition from trotting and galloping to race speed exercise in response to increased bone strains and change in principal strain direction.11,12 If the intensity or duration of exercise exceeds the ability of these sites to successfully adapt by cortical expansion, injury from repetitive activities may occur. These events create challenges for veterinarians to discriminate between normal adaptation and injury, with attendant increased risk for stress and catastrophic fractures. Whereas dorsal metacarpal expansion is necessary for adaptation to the rigors of racing, and a large proportion of horses manifest clinical signs of dorsal metacarpal disease (bucked shins) during this process, 2 catastrophic metacarpal fractures are infrequent occurrences. However, metacarpi with intracortical lucency and/or thick, focal new periosteal bone formation in addition to clinical signs of dorsal metacarpal disease (i.e., focal pain, heat, edema, and reluctance to perform or lameness) should be considered at risk for fracture.
Study limitations include the convenience sample from 12 horses. Factors that may have biased the metacarpi available for examination are unknown. Missing bone fragments compromised the ability to fully reconstruct fractured metacarpi, but also likely resulted in conservative estimates of the number and/or proportion of fractured metacarpi that had preexisting lesions because abnormal findings may have been present only on the missing fragments. Radiographic findings observed on radiographs of bone specimens may be harder to detect on clinical radiographs of metacarpi because of surrounding soft tissues.
We conclude that complete supracondylar and diaphyseal MC III fractures in Thoroughbred racehorses are likely to be associated with preexisting lesions. Racehorses with radiographic evidence of intracortical stress remodeling or incomplete stress fractures of the dorsal cortex of MC III should be considered at risk for complete fracture.
Footnotes
Acknowledgements
We thank Shannon Mitchell for illustration collation, and the veterinary pathologists at the California Animal Health and Food Safety Laboratory System for providing samples.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for publication of this work was provided by the Center for Equine Health with funds provided by the State of California pari-mutuel fund and contributions by private donors.