
Abstract
Equine catastrophic skeletal breakdown injury is a serious issue within the racing industry, given the impact on equine and human health. The metacarpo- and metatarso-phalangeal (fetlock) joints are common sites of catastrophic injury. However, lesions involving articular cartilage, subchondral bone, and synovium are commonly identified within the fetlock of the contralateral limb; hence, it is imperative that lesions in both limbs are evaluated and characterized during postmortem examination. Bone and articular cartilage changes typically occur in specific locations, related to cyclic fetlock load and overextension during high-speed exercise. Associations between preexisting degenerative fetlock lesions and catastrophic injury are a focus of continued research. These lesions often occur because of adaptive failure related to cumulative damage. Further investigation of these lesions is imperative to determine their impact on equine performance or injury. Ultimately, consistent documentation of catastrophic versus non-catastrophic osteochondral lesions provided by pathologists, in the context of training history, diagnostic imaging, and the presence or absence of catastrophic injury, will contribute to further understanding of skeletal responses associated with catastrophic failure.
Research on catastrophic musculoskeletal injuries of racehorses is important for the equine racing industry, given the impact of these injuries on equine and human (jockey, exercise rider, driver) health as well as public perception of the racing industry. Metacarpo- and metarso-phalangeal (commonly referred to as the fetlock) joint injuries, often associated with degenerative changes of the distal end of metacarpal and metatarsal three (MCIII and MTIII), are among the most common catastrophic injuries in Thoroughbred racehorses. The most recently published breakdown injury rate from the Equine Injury Database for the 2015 racing season, which collects data from 118 participating racetracks in the United States, is 1.62 per 1,000 starts (https://goo.gl/DsLkBw). Continued investigation of the nature and pathogenesis of musculoskeletal lesions that can predispose to catastrophic injury is needed.
Previous work evaluating the forelimbs of racehorses euthanized following catastrophic injury often identified degenerative articular cartilage and bone lesions in the affected and/or contralateral limbs, indicating preexisting lesions at the distal end of MCIII and MTIII, thus predisposing to fetlock catastrophic injury.1,20,21,31,37–39 Detection of a preexisting, predisposing lesion at the site of catastrophic fracture can be difficult because of hemorrhage, loss of integrity of the articular cartilage and bone, and/or embedding of track material in open fractures. In such cases, evaluation of the contralateral limb can provide valuable insight into the skeletal adaptation processes occurring in a horse. Given the footfall pattern of the gallop, lesions are often bilaterally symmetric between the affected and contralateral limbs. In addition, the forelimbs, especially the leading forelimb, sustain a higher mechanical load than the hindlimbs.3,19
The current theory regarding the mechanism of preexisting skeletal lesions and catastrophic injury involves cumulative damage of the articular cartilage and subchondral bone (traumatic overload arthrosis/arthritis) as a result of repetitive strain during high-speed exercise and fetlock hyperextension, resulting in tissue fatigue and ultimately skeletal failure.14,40 Consistent with Wolff’s law, 41 some degree of bone change (i.e., subchondral bone sclerosis) is expected in equine athletes to withstand the biomechanical rigors of training and racing. Bone adapts to biomechanical stress via continual modeling and remodeling processes, which results in alteration of bone structure (e.g., size and shape) in response to biomechanical stress and loading, and the replacement of damaged bone with new bone.6,14 The remodeling process readily occurs during rest periods but is reduced during periods of high cyclic loading.8,10,11,14 Therefore, repetitive high-loading of the fetlock joint during high-speed exercise can impair normal repair processes necessary to maintain a structurally and functionally robust bone, resulting in bone fatigue and cumulative damage characterized by lesions such as bone microcracks and articular cartilage degeneration.6,18,40 The presence of preexisting skeletal injury is compatible with cumulative damage and impaired or inadequate remodeling.6,29 Antemortem identification of the critical time point where cumulative lesions associated with skeletal fatigue produce increased susceptibility to catastrophic injury remains an ongoing area of research.
Knowledge of anatomic structures at the distal end of MCIII and MTIII is crucial because preexisting lesions typically occur in specific locations related to fetlock hyperextension. The medial and lateral condyles of the distal ends of the third metacarpal/metatarsal bones are separated centrally by the sagittal ridge, which runs in a dorsal-palmar direction, and the immediately adjacent parasagittal grooves (Fig. 1). The medial condyle is slightly larger than the lateral one. The palmar aspects of the condyles have a flatter curvature compared to the dorsal aspects of the condyles.9,17 During fetlock hyperextension, the weight-bearing forces are directly imposed on the palmar–plantar aspect of the condyles and the proximal sesamoid bones, whereas dorsal aspects of the condyles articulate with the proximal phalanx. The transverse ridge is the point where the dorsal aspect of the condyle transitions to the palmar aspect and is accentuated with racing and race training (Figs. 1, 2).
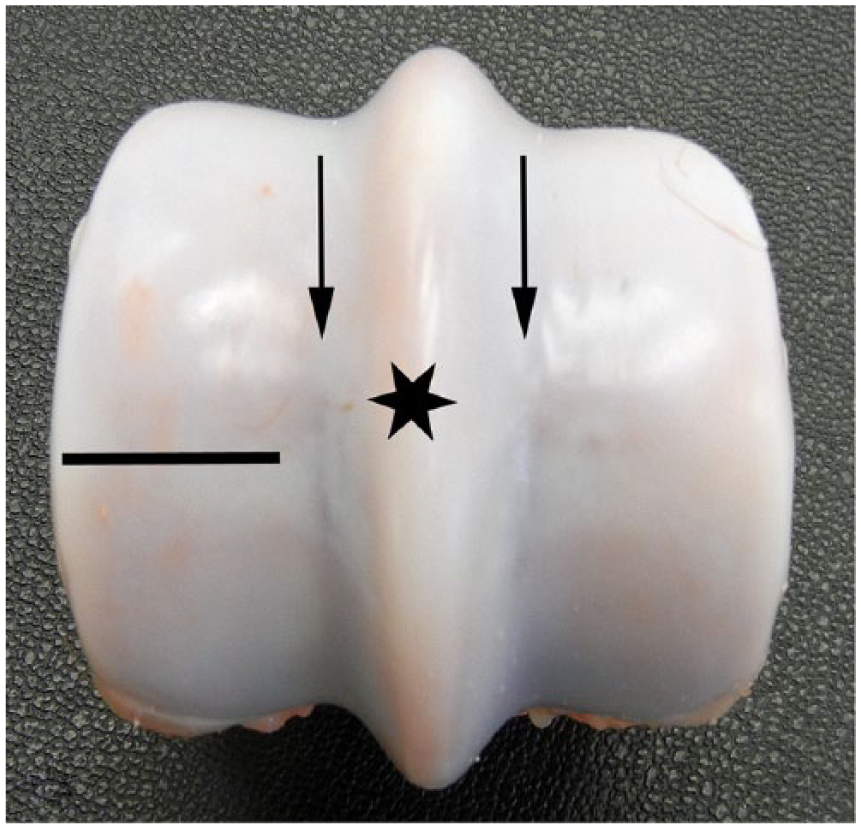
Normal gross anatomy of the distal end of the equine third metacarpal bone. The medial condyle is on the left and the lateral condyle on the right. The sagittal ridge is in the center (star). The parasagittal grooves (arrows) are immediately adjacent to the medial and lateral aspects of the sagittal ridge. The transverse ridge is located at the dorsal-to-palmar condyle transition (black line). The dorsal aspect of the condyle is at the top of the image; palmar aspect of the condyle is at the bottom of the image.
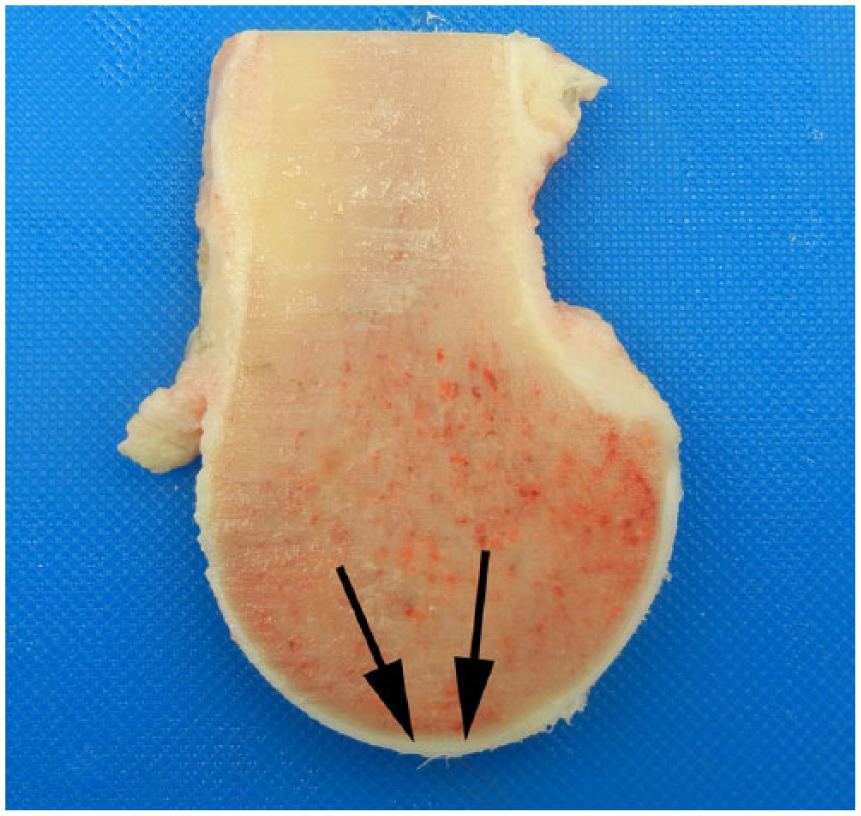
Location of the transverse ridge on parasagittal section of the medial condyle of the third metacarpal bone. The general location of the transverse ridge at the point where the dorsal aspect of the condyle transitions to the palmar aspect of the condyle (arrows). Dorsal is on the left and palmar is on the right.
Systematic postmortem examination and documentation of bone and articular cartilage changes related to high-speed exercise can provide important insight into racehorse lesions and may in the future help identity horses at risk for catastrophic injury. We use a previously published grading system1,24 when evaluating skeletal lesions of the distal end of MCIII and MTIII from horses euthanized for skeletal and non-musculoskeletal reasons while in active training or racing. Methodical evaluation of the distal end of MCIII and MTIII by diagnostic pathologists provides vital information to understand skeletal responses resulting in catastrophic injury. Herein, we provide a concise reference to familiarize diagnostic pathologists with the anatomy, descriptive terminology, and common lesions affecting the bone and cartilage of the distal end of MCIII and MTIII in racehorses that sustain catastrophic injuries. These lesions fall under the broad categorization of traumatic overload arthrosis/arthritis of the fetlock joint.
General articular cartilage lesions (thinning, fibrillation, parasagittal groove fissures, wear lines)
Articular cartilage provides a low-friction surface for unimpeded joint movement and transmits biomechanical forces associated with weight bearing. 36 Because articular cartilage is avascular, devoid of nerves, and comprises only one cell type (the chondrocyte), repair capabilities are limited. Thinning and fibrillation of articular cartilage is a well-documented degenerative response to athletic endeavors.6,29 Grossly discernible linear fissures of the articular cartilage in the parasagittal groove have been associated with lateral condylar fractures (Fig. 3). 31 Wear (score) lines within the articular cartilage occur across the condyles of MCIII and MTIII (Fig. 4). Wear lines are defined as vertical clefts in the articular cartilage. These lesions have been associated with impaired mechanical function of the articular cartilage. 15
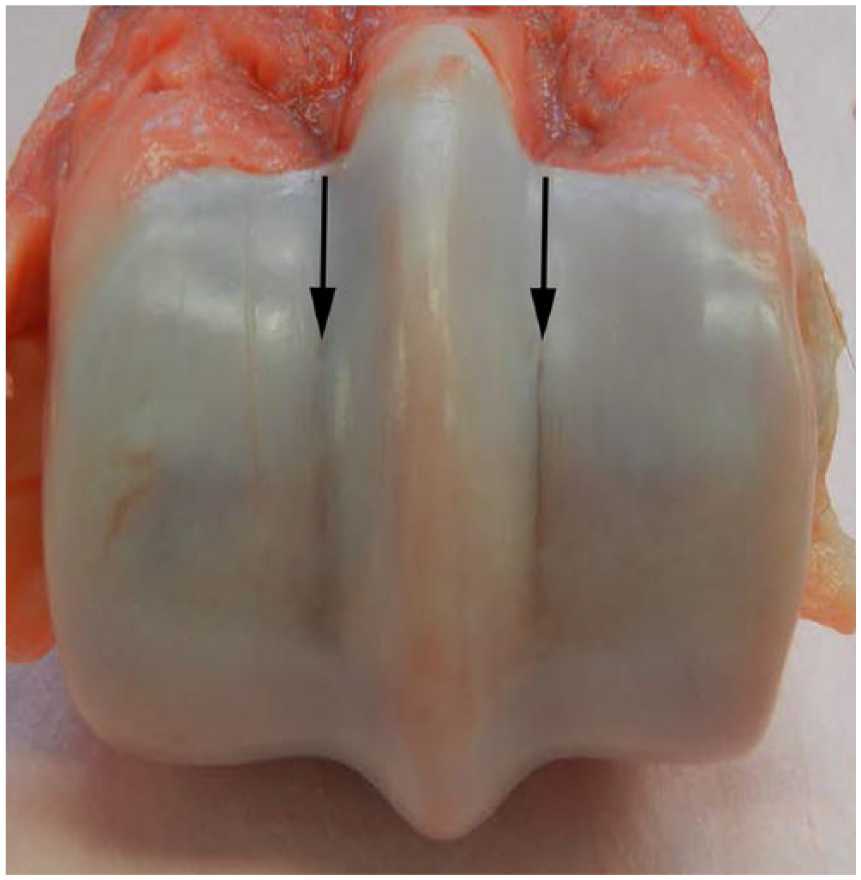
Parasagittal groove fissure (arrows) of the right third metacarpal bone in a horse that sustained a left front lateral condylar fracture. Medial is on the left and lateral is on the right.
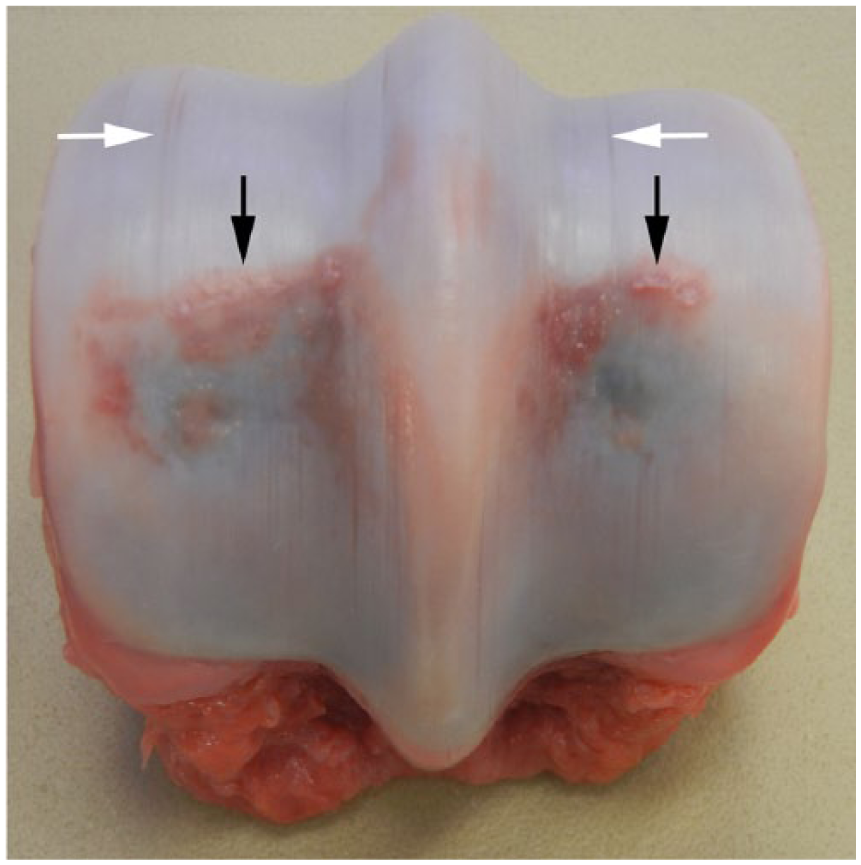
Articular cartilage and subchondral bone lesions in the distal end of the left third metacarpal bone of a horse that sustained a right front biaxial sesamoid fracture. Articular cartilage fibrillation along the transverse ridge (i.e., transverse ridge arthrosis [black arrows]). Articular cartilage wear (score) lines of the medial and lateral condyles (white arrows) are present. Focal central blue discoloration on the palmar aspect of both medial and lateral condyles, corresponding to subchondral bone lysis, is also evident. Medial is on the left and lateral is on the right.
Transverse ridge arthrosis
Changes in biomechanical properties of the articular cartilage, collagen fibers, and subchondral bone at the transverse ridge, as well as contact with the proximal sesamoid bones during fetlock hyperextension, make the transverse ridge particularly susceptible to development of degenerative changes, including articular cartilage fibrillation or ulceration, referred to as transverse ridge arthrosis (Fig. 4).25,26 This lesion has also been commonly termed “gull wing arthrosis” and is clinically associated with swelling in the caudal aspect of the fetlock. 34
Subchondral bone lesions
Subchondral bone, located immediately adjacent to and integrated with articular cartilage, functions to maintain joint shape and absorb biomechanical stresses placed on the joint. 12 Common gross lesions related to cumulative stress from high-speed exercise identified in the MCIII and MTIII condyles of racehorses include flattening of the palmar aspects of the condyles in response to continual loading of the region during exercise, subchondral bone sclerosis corresponding to regions of increased bone density in response to cyclic biomechanical forces (either physiologic or pathologic), and subchondral bone bruising corresponding to subchondral bone lysis in response to impaired remodeling (Figs. 4, 5).12,26,29–33 The relationship of subchondral bone sclerosis to catastrophic injury is still ambiguous. Although subchondral bone sclerosis of the condyles is expected as a physiologic response to strengthen the bone to withstand increased biomechanical forces, this lesion has also been associated with condylar fractures30,31 and compromise of hyaline cartilage,12,29,40 and as a predisposing factor of catastrophic injury. 39 Subchondral bone sclerosis is best observed on parasagittal or dorsal sections and is characterized as white, hyperdense bone that expands the subchondral bone plate with loss of red medullary spaces (Fig. 5). Increased bone volume fraction as a result of the production of new bone in the MCIII condyles has been identified in horses in work versus untrained horses. 2 Also identified on parasagittal or dorsal sections of the condyles is subchondral lysis, which is characterized by dark red–purple foci (commonly referred to as bone bruising) typically adjacent to regions of thinned or collapsed articular cartilage (Fig. 5). Subchondral bruising can be identified on the distal articular surface of intact MCIII and MTIII as variably sized, discrete blue foci visible through the articular cartilage overlying this region (Fig. 4).
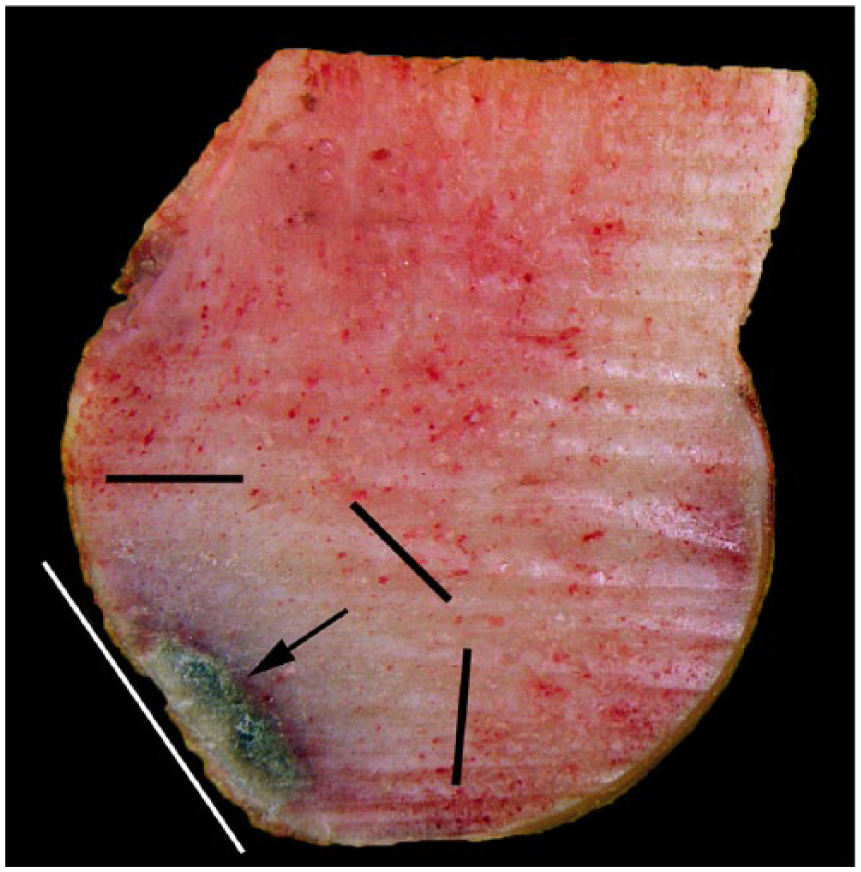
Palmar osteochondral disease characterized by trabecular bone sclerosis and palmar condyle flattening on a parasagittal section of the distal end of the right third metacarpal bone in a horse that sustained a left fore lateral condylar fracture and fetlock disarticulation. Focal subchondral bone lysis on the palmar side of the medial condyle (arrow). Dense, white bone (trabecular sclerosis) surrounds the focal area of subchondral bone lysis and trabecular sclerosis (black lines). The palmar condyle is flattened (white line).
Palmar osteochondral disease
Palmar osteochondral disease (POD) in racehorses is a well-recognized response to the biomechanics of high-speed exercise (Figs. 4, 5).1,23–25 POD was initially called traumatic osteochondrosis but the name has since changed to traumatic osteoarthritis to reflect a biomechanical versus developmental etiology. 25 Location of lesions on the palmar aspect of the MCIII and MTIII condyles is associated with the articulation with the proximal sesamoid bones and regular cyclic load and over-extension of the fetlock joint during training and racing.1,25,26,29,31,32 A grading system has been established to classify POD lesions.1,24 Inclusion of this grading system in racehorse postmortem examinations is highly recommended as it allows for a standardized approach. Early lesions involve subchondral bone lysis with no or minimal disruption of the overlying articular cartilage; these lesions progress to articular cartilage ulceration, and collapse of the subchondral bone in severe cases. 1 POD lesions are ~2–4 mm diameter, oval articular defects on the palmar or plantar aspect of the condylar surface, proximal to the transverse ridge, and located within 3–15 mm of the sagittal ridge on the respective condyle of MCIII or MTIII.25,26 The subchondral bruising that is a part of the POD process can extend past the articular defect, resulting in a larger lesion. In Thoroughbreds, POD is reported to be more severe in the forelimbs than hindlimbs, with the medial condyle of the forelimbs and the lateral condyle of the hindlimbs affected more frequently. 24 Although the specific grade of POD and its correlation to performance has yet to be established, a horse with a higher grade of POD is more likely to have problems localized to the fetlock joint while in training. 24 In a study of 102 active or retired-from-racing Thoroughbred horses, the reported prevalence of POD was 80.4%. 24
The association of POD with catastrophic fracture is controversial. Lateral condylar fractures, a common catastrophic injury, often originate from the palmar or plantar aspect of the lateral condyle and progress proximally up the shaft of MCIII and MTIII. These fractures are thought to occur because of the accumulation of stress-induced microfractures from failure of the bone to adequately adapt to biomechanical strain.18,31 Alternatively, because POD of variable severity is a common postmortem finding in racehorses that do not sustain a catastrophic injury,1,24,29,39 POD may represent a protective remodeling response. 38 Although the frequency of POD lesions identified at postmortem in limbs that do not sustain a catastrophic injury suggests that racehorses are able to train and work despite this skeletal lesion, 37 changes within the condyle may indeed lead to structural compromise that not only limits the horse’s ability to train at high speeds, but may also produce cumulative lesions that result in pathologic fracture. 38 Given the conflicting hypotheses pertaining to POD and catastrophic fractures in racehorses, further evaluation and documentation of third metacarpal lesions in equine athletes is imperative to further elucidate the significance of palmar osteochondral lesions in catastrophic injuries.
Proliferative synovitis (traumatic synovitis)
Although not as common as the previously described osteochondral lesions (authors’ unpublished observation), various severities of proliferative synovitis can be identified on postmortem examination. A bi-lobulated synovial pad is located on the dorsal (recessus dorsalis) aspect of distal MCIII and MTIII and extends to the sagittal ridge. 13 The synovial pad is suspected to act as a cushion.5,7 Because of fetlock hyperextension during high-speed exercise, the dorsal aspect of the proximal phalanx compresses the synovial pad, leading to thickening with embedded osteochondral fragments, and in severe cases, inflammation and fibrosis (Fig. 6). 4 These changes are thought to be a response to recurrent trauma to the synovial pad as opposed to a primary inflammatory synovitis. 5 In addition to the dorsal pouch, similar changes can occur to the synovium in the palmar pouch. Oftentimes, given increased pressure associated with thickening of the synovial fat pad, there is concurrent osteoclastic osteolysis in the adjacent cortical bone that produces a scalloped appearance of the dorsal or palmar–plantar supracondylar distal end of MCIII and MTIII. Grossly, in an unopened fetlock joint, this lesion manifests as swelling along the dorsal profile of the distal end of MCIII and MTIII. 28 Proliferative synovitis has also been referred to as villonodular synovitis, a term extrapolated from the human literature. This is a misnomer given that the histologic changes and proposed etiopathogenesis for the human and equine entities are different.

Synovial pad thickening (chronic proliferative synovitis) of the distal end of the right third metacarpal bone (stars).
Other lesions associated with traumatic overload arthrosis/arthritis of the fetlock
Acute fetlock capsulitis and synovitis that is associated with progression to severe osteoarthritis can occur. 16 Initially, this lesion appears clinically as a palpable warm effusion of the fetlock joint, but later it may result in thickening of periarticular tissues, lameness, and decreased range of motion. 28 Conformational abnormalities, increased biomechanical loading, and prior injury are predisposing factors. 29 Gross changes include thickened synovium and joint capsule. In addition, periarticular osteophytes along the distal end of MCIII and MTIII, proximal sesamoids, and proximal phalanx can be appreciated in the fetlock joint. Mild erosion to cartilage loss and chip fractures can occur along the dorsoproximal aspect of the proximal phalanx.
Role of diagnostic imaging
In addition to gross evaluation, advanced imaging of the limbs using either magnetic resonance imaging or computed tomography can provide important details pertaining to the type and extent of lesions within the cartilage and subchondral bone that cannot be obtained through gross examination of the external surface or cut sections. These imaging modalities are commonly used in clinical settings for identification of skeletal lesions that may predispose to catastrophic failure (Fig. 7).22,27,35,38,39 Therefore, evaluation of antemortem imaging in conjunction with postmortem evaluations could help to determine the distinction between physiologic skeletal adaption to high-speed exercise and impaired repair processes that predispose to catastrophic injury.

Magnetic resonance image (MRI) of the gross changes in Figure 5. There is focal, crescent-shaped, increased signal intensity in the subchondral bone (arrow) corresponding to subchondral bone lysis on the palmar side of the medial condyle. Decreased signal intensity, corresponding to bone sclerosis, surrounds the focal area of lysis. The palmar condyle is flattened. Proton density weighted parasagittal MRI.
Footnotes
Acknowledgements
We thank Adriel Sitzes for technical assistance and Emily Zurkuhlen for MRI study acquisition.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.