
Abstract
Clonality testing based on polymerase chain reaction is an important tool for diagnosis of lymphoproliferative diseases. Many primers have been designed and used for canine clonality testing. Canine intestinal lymphoma is usually diagnosed pathologically by examination of excised intestinal or endoscopic biopsy tissues, and clonality testing is sometimes used to support the pathological diagnosis if this examination is inconclusive. In the present study, the sensitivity of each previously published primer set for clonality testing was examined by using formalin-fixed, paraffin-embedded sections from 39 cases pathologically diagnosed as canine intestinal lymphoma (large-cell type). All 39 cases were immunohistochemically positive for cluster of differentiation (CD)3. Thirty-two out of the 39 cases showed clonality in the T-cell receptor gamma (TRG) with at least 1 of the tested primers. The primer set with the highest sensitivity detected all 32 cases with TRG clonality, with a sensitivity of 82.1%. These results provide useful evidence for the selection of primer sets for clonality testing of canine intestinal lymphoma.
Clonality testing is an important technique for diagnosis of lymphoproliferative diseases such as leukemia and lymphoma.1,2 Although many primer sets for canine clonality assays have been published,3,5,12,19,22,23 the sensitivity of each primer set is different. The selection of appropriate primers for specific clonality tests is important, and it is possible that the overall sensitivity of clonality assays depends on the primer sets used. However, to date, there has been no single study comparing the published primer sets using the same samples.
Intestinal lymphoma accounts for 5–7% of canine lymphoma cases. 6 Microscopic examination of excised or endoscopic biopsy tissues is essential for diagnosis of this disease. However, clonality tests show that cases diagnosed as lymphoplasmacytic enteritis may exhibit clonal rearrangement. These cases generally exhibit a short survival time compared with those that feature polyclonal rearrangement.10,18 The data suggests that even when the pathological diagnosis is enteritis, comorbid lymphoma may be present as well. Therefore, employing clonality tests together with pathological examinations to support morphological diagnosis and to avoid missing instances of lymphoma may be prudent.4,13 Intestinal lymphoma cases in particular are more likely to require a clonality test for diagnosis than cases of multicentric or cutaneous lymphoma.
For clonality tests in humans, many loci are selected to ensure detection of rearrangements.9,15,21 For canine cases, however, target loci are restricted to the T-cell receptor gamma (TRG) and immunoglobulin heavy chain (IGH) genes,3,5,12,22,23 and sensitivity may be lower than in human tests. It is therefore necessary to use the primer sets that yield the highest sensitivity under test conditions for canine clonality tests. The aim of our study was to identify the best primer sets among all previously published primers for TRG, based on a comparison of detection rates for canine intestinal T-cell lymphoma.
Forty intestinal lymphoma (large-cell type) cases with a mass lesion submitted to a commercial pathological laboratory (North Lab, Hokkaido, Japan) were randomly chosen for this study. The paraffin sections (4-µm thick) were then stained with hematoxylin and eosin. All cases were diagnosed morphologically as intestinal lymphoma (large-cell type) by a board-certified pathologist (Y Kagawa). All cases showed intestinal mass and tumor cells distributed in the mucosal and submucosal area. An automated immunohistochemistry (IHC) system a was used to process the deparaffinized and antigen retrieval tissues. The IHC antibodies used were cluster of differentiation (CD)3 b (mouse anti-human monoclonal) and CD79a c (mouse anti-human monoclonal).
Only the tumor region was scraped from the 20-µm-thick section with a sterilized needle after deparaffinization, and genomic DNA was extracted using a commercial genomic DNA extraction kit d according to the instruction manual. Concentration of DNA was determined by a spectrophotometer. e Integrity of genomic DNA was verified by amplification of the constant region of IGH (130 bp)3 and c-KIT exon 8 (228 bp). 17
All primers used in our study are listed in Table 1. Primers previously identified for TRG are designated T-Burnett, 3 T-Chaubert, 5 T-Keller, 12 T-Vernau, 22 and T-Yagihara 23 (all named according to the publication author’s name). In the original report describing T-Yagihara, 2 forward and 2 reverse primers were permuted, so, in total, 4 sets of primers were used to detect rearrangement of TRG. 23 In our study, 1 forward primer and 2 reverse primers were permuted and thus 2 sets of primers were used in polymerase chain reaction (PCR) experiments, as performed in other studies (Table 1).3,5 The 2 sets of primers were designated as T-Yagihara (Va) and (Vb), respectively. The primer sets for IGH were designated B-major, 3 B-minor, 3 B-Tamura, 19 and B-Vernau. 22
Primers used in the current study and the polymerase chain reaction conditions for each primer.
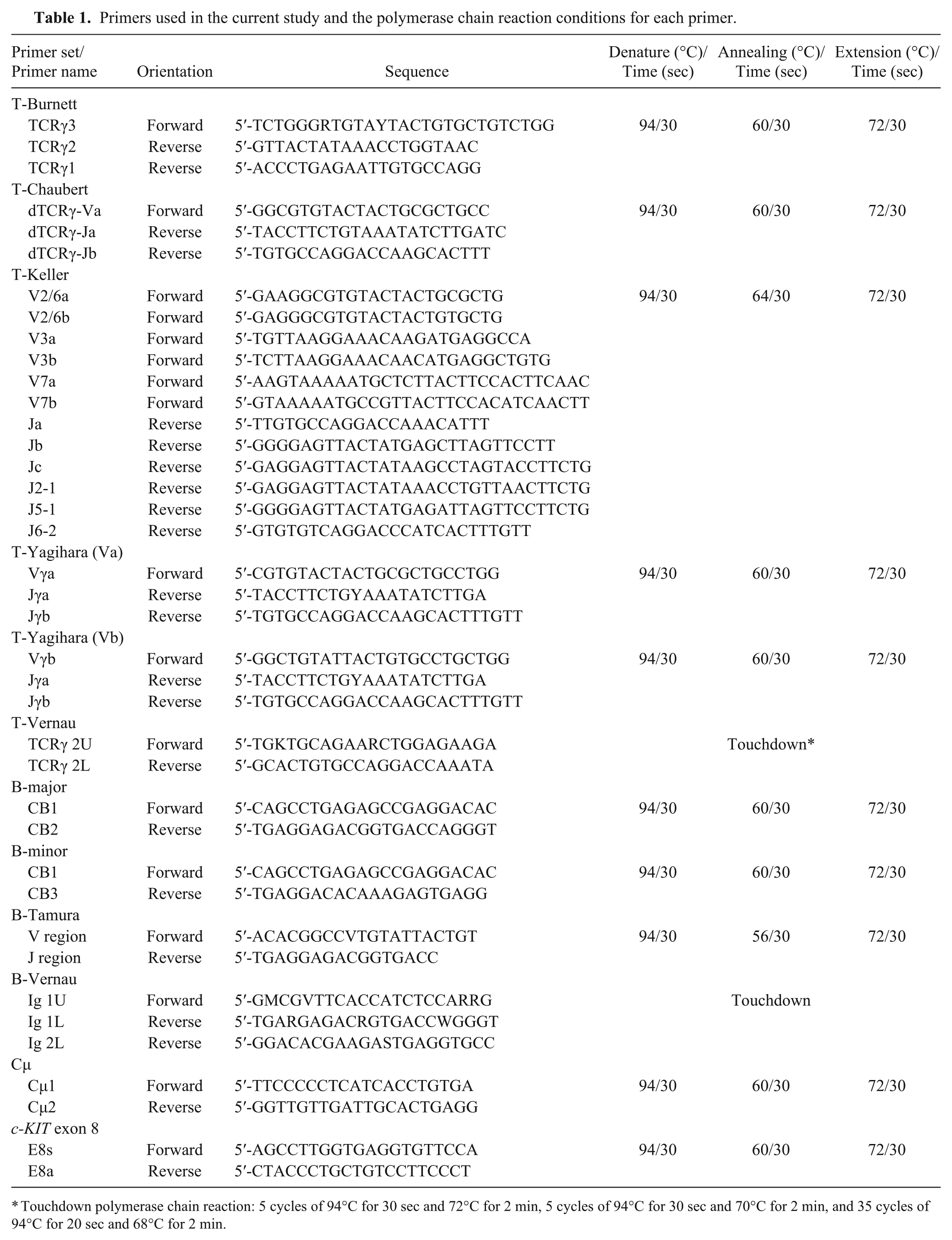
Touchdown polymerase chain reaction: 5 cycles of 94°C for 30 sec and 72°C for 2 min, 5 cycles of 94°C for 30 sec and 70°C for 2 min, and 35 cycles of 94°C for 20 sec and 68°C for 2 min.
Polymerase chain reaction was performed with 40 ng of genomic DNA as a template, in a total volume of 20 µL, containing 1× PCR buffer, 1.5 mM Mg2+, 2.5 mM deoxynucleotide triphosphates, 0.2 µM of each primer, and 0.5 units of DNA polymerase. f After initial denaturation at 95°C for 120 sec, 35 cycles of amplification were carried out at 94°C for 30 sec, followed by annealing for 30 sec and extension at 72°C for 30 sec. Annealing temperatures reported in original articles were used (Table 1), with the exception of T-Vernau and B-Vernau, which were used on touchdown PCR according to a previous study. 22 For heteroduplex analysis, the PCR product was denatured at 95°C for 5 min and re-annealed at 4°C for 1 hr. A negative control with water instead of template DNA was included in each PCR preparation. All sample PCRs were prepared in duplicate and electrophoresed side-by-side on a non-denatured 12% polyacrylamide gel g to confirm reproducibility of the amplification. The gel was stained with fluorescent dye h and visualized on a blue LED transilluminator.
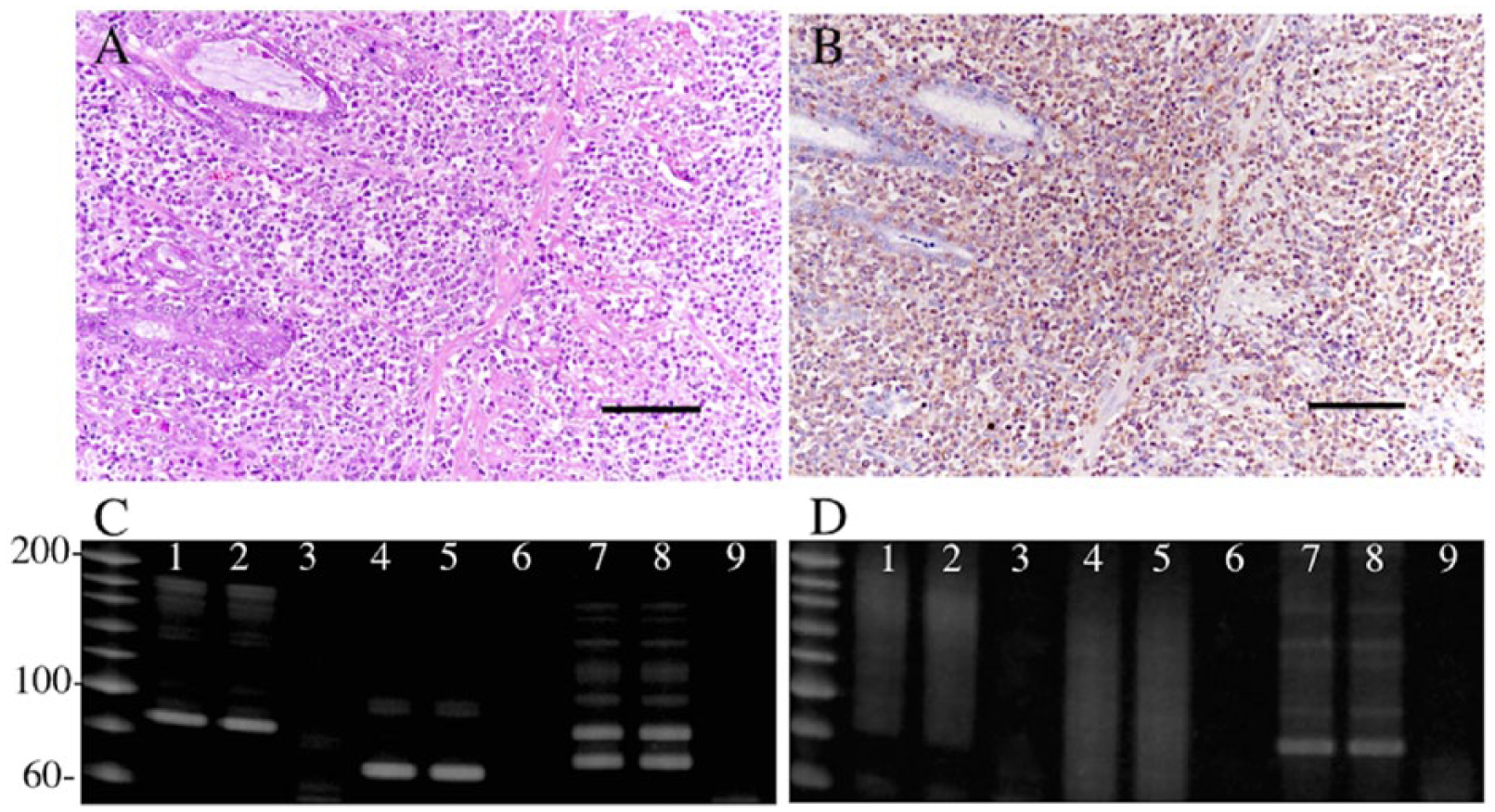
Clonality was determined based on previous interpretations.12,16 It was assumed that 1–2 reproducible and discrete bands indicated monoclonal or biclonal rearrangement, and a minimum of 3 reproducible and discrete bands indicated oligoclonality. These 3 patterns were interpreted as clonal. Single or several nonreproducible discrete bands were interpreted as pseudoclonal. Smear product was identified as polyclonal. Pseudoclonal, polyclonal, and no-amplification patterns were interpreted as not clonal. Representative electrophoretic patterns in the clonal and polyclonal categories are shown in Figure 1C and 1D.
Forty intestinal lymphomas were classified as T-cell or B-cell neoplasm by IHC profiles of CD3 and CD79a. Of 40 cases, 39 were T-cell lineage, and only 1 case was B-cell lineage. Following World Health Organization criteria, 20 39 cases were consequently classified as intestinal T-cell lymphoma and used for clonality testing, with the remaining single case being identified as large B-cell lymphoma and was not used for clonality testing.
Before the clonality test was performed, the integrity of the genomic DNA extracted from formalin-fixed, paraffin-embedded sections was verified. A PCR product with 130 bp on the IgH constant region was detected from all 39 samples. A PCR product with 228 bp on c-KIT exon 8 was amplifiable in 26 out of 39 samples (data not shown). This suggests that the genomic DNA had been damaged or chemically modified. However, all 39 samples were considered to be suitable for clonality testing because the amplicon size of the target was ≤130 bp.
Figure 1A and 1B shows representative hematoxylin–eosin staining and IHC by anti-CD3 antibody. All 39 cases had a mass lesion on the small intestine. Large lymphocytes that were positive for CD3 were widely infiltrated and effaced mucosa to muscular structure. All were diagnosed as lymphoma. Clonality was detected in 32 out of 39 cases of intestinal T-cell lymphoma (Table 2). The primer set T-Keller yielded clonal bands in 32 out of 39 cases and showed the best detection rate on the TRG locus (82.1%). The other primer sets detected fewer cases, and all of the cases detected by T-Burnett, T-Chaubert, T-Yagihara, and T-Vernau were included in the 32 detected by T-Keller. Two of the 32 were detected only by T-Keller primer sets (Table 3). All of the intestinal T-cell lymphoma cases tested negative from the IGH primer sets.
Molecular conclusions from the clonality test.*

Numbers in the first 2 rows are the number of cases determined as “clonal” (first row) or “not clonal” (second row) when that primer was used.
Electrophoretic and immunohistochemical profile.*
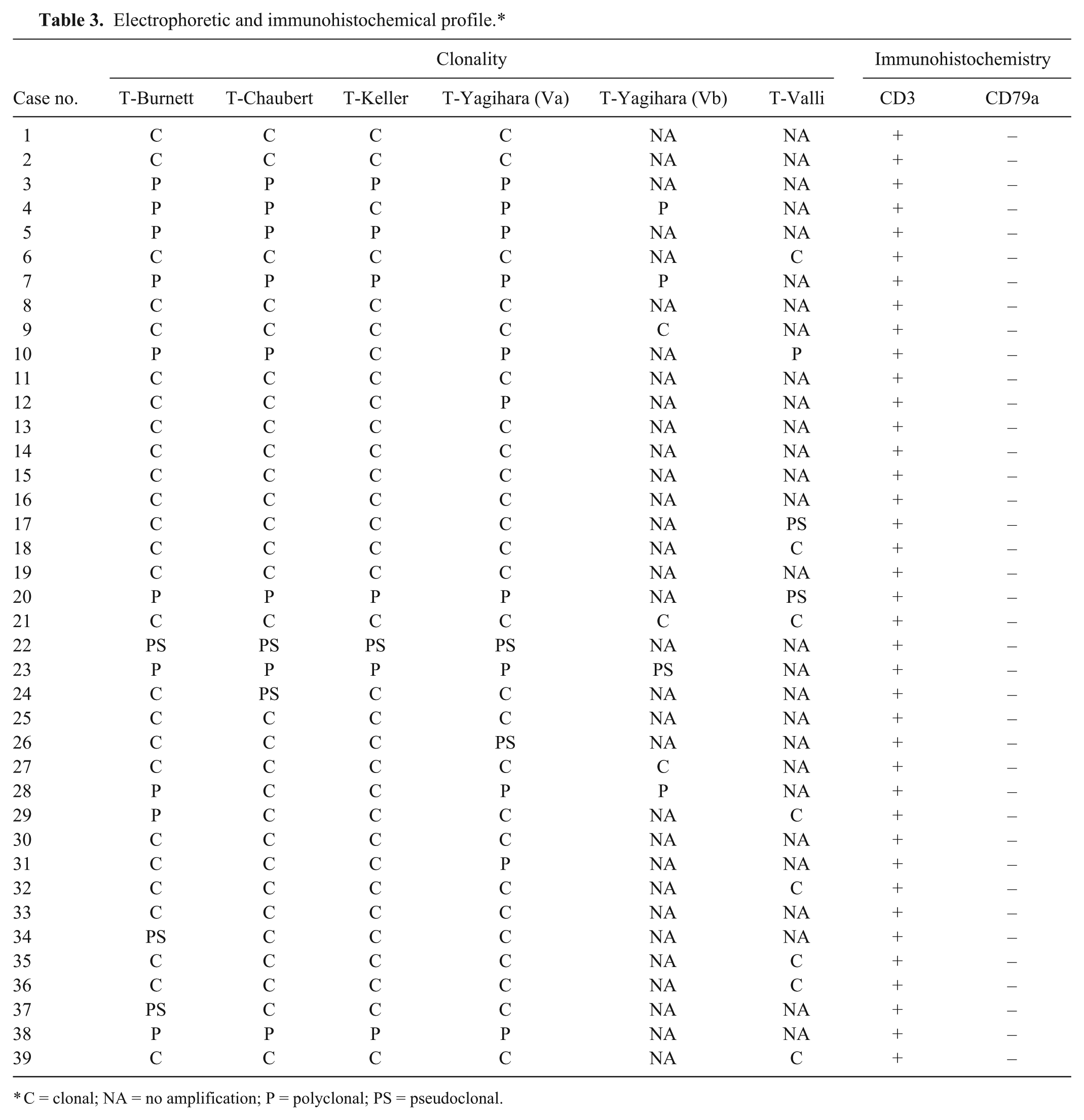
C = clonal; NA = no amplification; P = polyclonal; PS = pseudoclonal.
Our study revealed that the T-Keller primer set, used to test for TRG rearrangement, exhibits the highest detection rate in clonality assays of canine intestinal T-cell lymphoma (large-cell type). The detection rates of T-Burnett, T-Chaubert, T-Yagihara, and T-Vernau were lower than that of T-Keller, and cases that were positive for those primers were also detectable by T-Keller. It has previously been shown, by comparison of the genomic sequences of each segment in the variable region of the gene, that the primers published prior to T-Keller exhibit various degrees of mismatches with TRG. 12 Mismatches may cause misannealing to the target sequence, so these primers may not cover all segments of the gene, which decreases the sensitivity of the clonality test. T-Keller consists of gene-specific primers that match the V and J regions, which were designed based on a genomic sequence of the TRG locus11,12 In contrast, T-Burnett, 3 T-Chaubert, 5 T-Vernau, 22 and T-Yagihara 23 were designed based on complementary (c)DNA sequences that were obtained from tissues such as the spleen by reverse transcription PCR, or from GenBank. Because of the way it was designed, T-Keller has no potential mismatches and therefore should show greater sensitivity than the other primer sets in clonality tests. This was confirmed in the present study. Primer sets for human TRG clonality testing were also designed as sequence-specific and showed 87% sensitivity to T-cell malignancy. 8 Although it is difficult to compare sensitivity for TRG clonality because the gene structure of the TRG locus differs between human and dog,12,15 the quality of the T-Keller primer set for canine clonality might be comparable to TRG primer sets for human clonality.
In a previous study that used the primer sets T-Vernau and T-Burnett, the sensitivity of clonality tests in 12 canine intestinal lymphoma cases was 66.7%. 8 The sensitivity of T-Burnett in our study was the same as this previous finding. Taken together, the primers T-Burnett and T-Vernau are insufficient for clonality testing of canine intestinal lymphoma.
The survival time of dogs with chronic enteritis that tested positive for clonality was significantly shorter than that of dogs with clonality-negative enteritis. 10 In another study, clonality-positive cases in inflammatory intestinal disease were identified as having a reduced diversity of lymphocytes. 18 Cases with reduced diversity showed a higher risk of death, and it was suggested that the clonality-positive cases may have been suffering from intestinal lymphoma. The sensitivity of the clonality test is relatively high, and 80% of stage 3 lymphomas tested positive for clonality on peripheral blood, indicating that positive results could be obtained even if there were no microscopically visible tumor cells. 14 There may, however, be a minimum number of tumor cells in a sample for a positive clonality result to be obtained in cases of inflammatory gastrointestinal disease, below which the test result would still be negative. Diagnosis of inflammatory bowel disease and intestinal lymphoma has been improved by the spread of endoscopes. The quality of diagnosis of intestinal lymphoma may, however, be further improved by the combination of pathological examination and clonality testing. 13 To this end, clonality testing should be performed using the primer set that yields the highest sensitivity.
Some cases showed a polyclonal pattern on clonality testing, as indicated by a smear product on polyacrylamide gel electrophoresis. As a smear product may be yielded from a polyclonal lymphocytic population carrying many types of rearranged TRG or IGH, a clonal product may sometimes be obscured by a smear product showing a polyclonal background. 12 Although this possibility could not be fully ruled out in our study, 7 cases for clonality negative with the T-Keller primer set might be due to a polyclonal background. Alternately, the number of normal lymphocytes in all samples may have been lower in our study because only the tumor region that formed the intestinal mass lesion for which large and CD3-positive lymphocytes had infiltrated were excised from each paraffin section; although this region presumably contained the majority of tumor lymphocytes. As mentioned above, 7 cases yielded no clonal amplification. The T-Keller primer set does not contain TRGV5-2 due to the predicted infrequency of rearrangement 12 ; however TRGV5-2 cDNA was isolated from peripheral lymphocytes although the rate of usage was low. 23 Absence of TRGV5-2 primer might be another reason for the failure of clonal amplification.
All 39 intestinal T-cell lymphoma cases tested as “not clonal” with each IGH primer set. B-cell lymphoma also occurs in the gastrointestinal tract.6,7 It may be important to note that IHC classification by cell lineage is beneficial for selection of primer sets for B or T cells prior to clonality testing. Although the T-Keller primer set showed the highest sensitivity for canine gastrointestinal lymphoma; if predominantly B-cell lymphomas were chosen, then an IGH primer set would likely have been more sensitive.
The present study comprehensively examined the sensitivity of primers for clonality tests of canine intestinal lymphoma, and revealed that the primer set T-Keller was the most sensitive. These results provide evidence for selection of the best primer set for clonality testing of canine intestinal lymphoma.
Footnotes
a.
Histostainer, Nichirei, Tokyo, Japan.
b.
Dako Denmark A/S, Glostrup, Denmark.
c.
Dako Denmark A/S, Glostrup, Denmark.
d.
High pure PCR template preparation kit, Roche Diagnostic Japan, Tokyo, Japan.
e.
ND-1000, Thermo Fisher Scientific Inc., Waltham, MA.
f.
Blend Taq plus, TOYOBO Corp., Tokyo, Japan.
g.
ATTO Corp., Tokyo Japan.
h.
GelStar nucleic acid gel stain, Lonza Rockland Inc., Rockland, ME.
Authors’ contributions
M Takanosu substantially contributed to conception and design of the study and drafted the manuscript. Both authors contributed to acquisition, analysis, and interpretation of data; and gave final approval. Y Kagawa critically revised the manuscript. M Takanosu agrees to be accountable for all aspects of the work in ensuring that questions relating to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, or publication of this article.