
Abstract
Mycoplasma haemocanis is a hemotropic bacterium that can be associated with acute hemolytic disease in immunocompromised or splenectomized dogs. The present case report describes for the first time the use of real-time quantitative polymerase chain reaction (qPCR) to monitor M. haemocanis infection in a splenectomized dog. The report also describes the application of real-time qPCR for the analysis of deoxyribonucleic acid extracted from stained blood films. The analysis of blood films from the time of initial presentation allowed a retrospective confirmation of M. haemocanis infection. The M. haemocanis copy numbers remained high throughout antibiotic treatment of this dog. A decline in copy numbers was only recorded after 11 months of therapy, when improvements in clinical and hematological indices were also noted. Clearance of infection was not achieved, and the dog remained positive for M. haemocanis at 3.5 months postcessation of antibiotic therapy. Cytological examination of blood films for the presence of organisms was insensitive for the detection of parasitemia.
Mycoplasma haemocanis is a hemotropic bacterial species that parasitizes the erythrocytes of dogs, causing hemolysis and anemia in splenectomized and immunocompromised animals. 5,19 Previously known as Haemobartonella canis, this bacterium has recently been reclassified from the order Rickettsiales to the order Mollicutes within the Mycoplasmataceae family. 15 The introduction of highly sensitive polymerase chain reaction (PCR) assays for the detection of M. haemocanis has indicated that infection may be more common than previously appreciated. This is particularly noted in countries with warmer climates and those with endemic Rhipicephalus sanguineus (brown dog tick) populations. 1,9,10,11,12,17,25 Clinical disease, however, remains uncommon and is rarely reported in animals that are immunocompetent and that are not splenectomized. 13,16 As a result of the low incidence of clinical disease, there is little available information on monitoring of infection in clinical cases, and few reports exist that examine the efficacy of antibiotic therapies against canine hemoplasmas. In the present report, real-time quantitative PCR (qPCR) was used to monitor the course of infection and therapy in a splenectomized dog with naturally acquired M. haemocanis infection. To the authors' knowledge, this is the first report describing the use of qPCR to monitor infection in a dog that also includes the retrospective analysis of DNA extracted from stained blood films.
A 9-year-old, intact, male Labrador retriever was presented to a first-opinion clinic after visiting an after-hours emergency service for acute collapse and abdominal bloating. The dog had been splenectomized 4 months prior to presentation because ultrasound examination had indicated partial intermittent splenic torsion causing recurrent bouts of abdominal distension. Recovery from surgery had been uneventful until the present episode. No other history of illness was noted, and the dog had never traveled outside of the United Kingdom or received any blood transfusions.
On presentation, the dog appeared weak, with pale mucous membranes and a slightly distended abdomen. No obvious cause for the abdominal distension could be identified on ultrasound examination, and a blood sample was obtained for routine hematology. The dog was found to have a regenerative anemia, with increased numbers of nucleated red blood cells (nRBCs) and a moderate thrombocytopenia (Table. 1). On examination of a blood smear stained with May-Grünwald and Giemsa, numerous small spherical bodies were seen on approximately 90% of the erythrocytes. These bodies appeared epierythrocytic and were present both individually and in chains (Fig. 1A) across the surface of the cells. Based on the morphologic appearance of the bodies, a diagnosis of anemia secondary to M. haemocanis infection was made and the dog was immediately started on oxytetracycline (24 mg/kg orally every 8 hr on an empty stomach). The presence of epierythrocytic organisms was subsequently confirmed using transmission electron microscopy on the initial blood sample by fixing the specimen with modified Karnovsky solution, postfixing in 1% osmium tetroxide, and routinely embedding into resin (Fig. 1B).
Following initiation of therapy, the dog made a rapid clinical recovery. Table 1 shows that the dog's hemoglobin value had increased by 7 days postdiagnosis (p.d.) and had returned to within the reference range by 17 days p.d. Cytologically, occasional small spherical structures were thought to be present on erythrocytes at day 7 p.d. but not at day 17 p.d. (Table. 1). At day 29 p.d. (not shown in Table 1), withdrawal of antibiotics was attempted, but after 4 days the dog rapidly relapsed clinically, and oxytetracycline was immediately restarted. At the time of this relapse, further laboratory assistance was sought for the molecular evaluation of the original diagnosis of M. haemocanis, as well as monitoring of M. haemocanis with qPCR.
The first blood sample tested for M. haemocanis by qPCR was collected on day 58 p.d. Further blood samples were tested on days 87, 122, 142, 186, 203, 204, 205, and 316 p.d. For these samples, DNA was extracted from 100 μl of ethylenediaminetetraacetic acid (EDTA) blood using a commercial kit, b per the manufacturer's protocol. The DNA was eluted with 100 μl of elution buffer. Appropriate negative and positive controls were included within each extraction run. Quantitative PCR was then performed on the extracted DNA using a previously described assay, 1 which incorporates amplification of an internal control by duplexing with a qPCR assay specific for canine glyceraldehyde-3-phosphate dehydrogenase (GAPDH). The inclusion of an internal control ensures amplifiable DNA is present and monitors for the presence of PCR inhibitors. Quantification of M. haemocanis copy number was determined by comparison to a standard curve generated by the dilution and analysis of plasmid samples containing known numbers of M. haemocanis, as previously described. 1 Each sample was analyzed in triplicate with appropriate negative and positive controls included within each PCR run. To verify the identity of the infecting organism, sequencing of the 16S ribosomal RNA gene and a portion of the ribonuclease P β-subunit gene were performed using the same EDTA blood sample, as described previously. 18,23 The results indicated complete identity with M. haemocanis sequences available from GenBank (http://www.ncbi.nlm.nih.gov/).
Unfortunately, whole blood samples obtained before the start of qPCR monitoring (i.e., before day 58 p.d.) were unavailable for analysis. In order to confirm the initial diagnosis, retrospective qPCR analysis was performed on DNA extracted from each of 3 blood films prepared from blood collected on days 0, 7, and 37 p.d., respectively. These blood films had been routinely stained with May-Grünwald and Giemsa. DNA was extracted from the blood films as described previously (Tasker S, Peters IR, Mumford AD, et al.: 2010, Investigation of human hemotropic Mycoplasma infections using a novel generic hemoplasma qPCR optimized for blood samples and blood smears. Under review). Analysis of the blood film prepared at the time of diagnosis on day 0 p.d. confirmed the presence of M. haemocanis (Table. 1). However, blood films from day 7 p.d. were negative for hemoplasma DNA by qPCR, while the blood films from day 37 p.d. were only qPCR positive in 3 of 8 replicates.
The results of the qPCR analyses performed on whole blood are presented graphically in Fig. 2. Between days 58 and 87 p.d., no marked change in the level of M. haemocanis copy numbers was noted. As a result of this lack of decrease in M. haemocanis copy numbers, the dog was changed to enrofloxacin treatment (5.6 mg/kg orally every 24 hr) on day 100 p.d. Severe neutropenia was noted at day 122 p.d. after 3 weeks of enrofloxacin therapy (Table. 1). Unfortunately, as the result of a gap in monitoring, the exact time of onset of the neutropenia could not be established. Copy numbers of M. haemocanis remained relatively stable during the first 14 weeks (98 days) of enrofloxacin therapy. During this period, gradual onset of lethargy and weight loss were noted in the dog, along with persistent neutropenia and a gradual decline in hematocrit (Table. 1). After one further attempt at withdrawal of therapy (4 days in total), with subsequent clinical relapse at day 200 p.d., a mutual decision was reached with the owners to maintain the dog on enrofloxacin, with the understanding that euthanasia would be considered if the dog's condition deteriorated further. However, between days 270 and 300 p.d., an improvement was noted in the dog's demeanor and activity levels, including a weight gain of 3 kg. Hematology performed on day 316 p.d. indicated a reduction in the severity of the neutropenia and resolution of the ongoing anemia. A corresponding decrease in M. haemocanis copy numbers was also noted by qPCR. Four weeks later, the owner stopped all antibiotics. The dog was unavailable for sampling at this time, but a blood sample obtained 3.5 months after withdrawal from therapy (day 448 p.d.) showed a very mild decrease in red blood count, a mild thrombocytosis, mildly increased nRBCs, and a mild increase in the reticulocyte count. The mild thrombocytosis and increased nRBCs were expected, given the asplenism. However, the mildly decreased red blood count and mild reticulocytosis indicated that increased red cell turnover was occurring. The qPCR indicated that M. haemocanis was still present, despite the fact that the dog appeared normal on physical examination.
Results from routine hematology and selected real-time quantitative polymerase chain reaction analyses.*
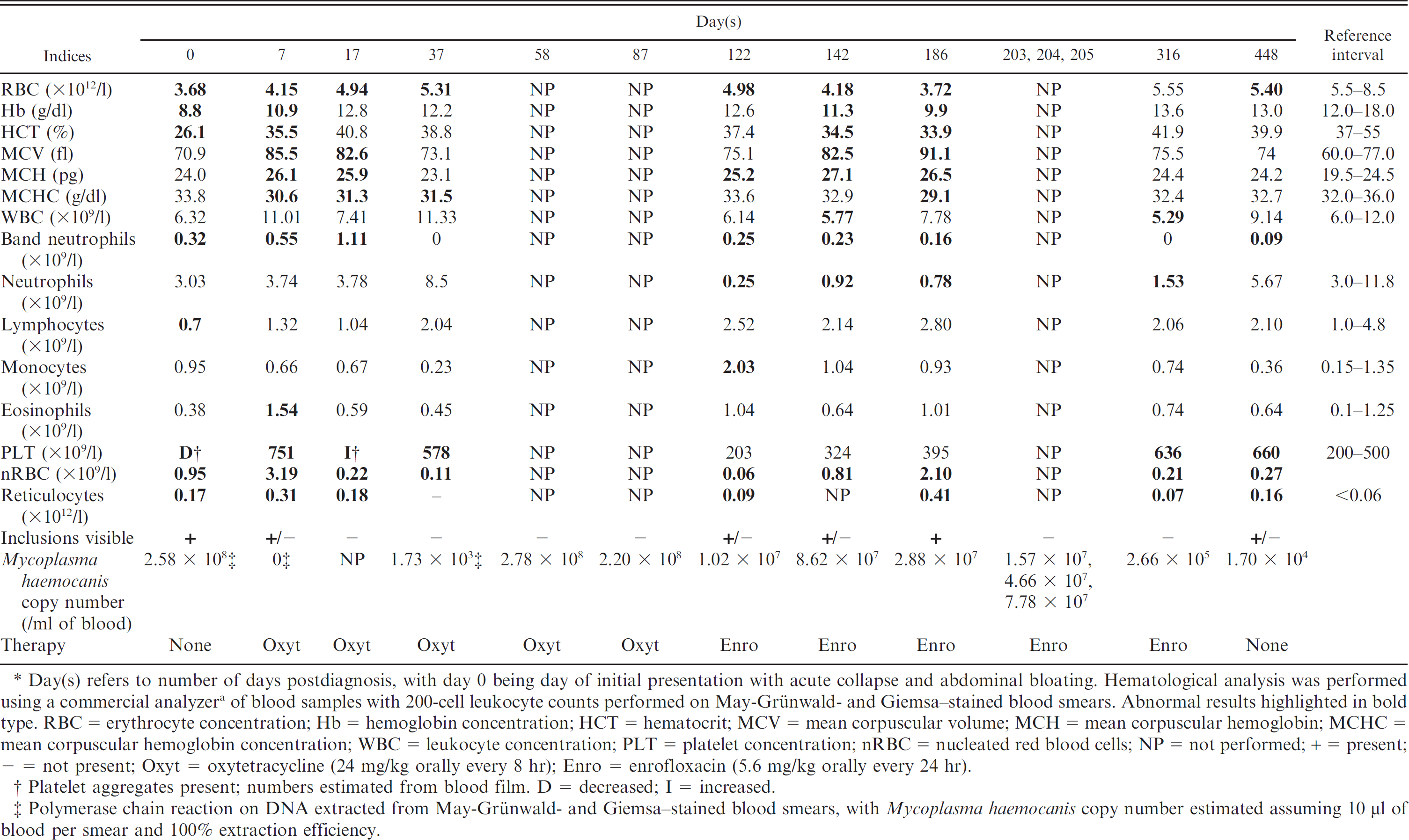
Day(s) refers to number of days postdiagnosis, with day 0 being day of initial presentation with acute collapse and abdominal bloating. Hematological analysis was performed using a commercial analyzer a of blood samples with 200-cell leukocyte counts performed on May-Grünwald- and Giemsa—stained blood smears. Abnormal results highlighted in bold type. RBC = erythrocyte concentration; Hb = hemoglobin concentration; HCT = hematocrit; MCV = mean corpuscular volume; MCH = mean corpuscular hemoglobin; MCHC = mean corpuscular hemoglobin concentration; WBC = leukocyte concentration; PLT = platelet concentration; nRBC = nucleated red blood cells; NP = not performed; + = present; - = not present; Oxyt = oxytetracycline (24 mg/kg orally every 8 hr); Enro = enrofloxacin (5.6 mg/kg orally every 24 hr).
Platelet aggregates present; numbers estimated from blood film. D = decreased; I = increased.
Polymerase chain reaction on DNA extracted from May-Grünwald- and Giemsa—stained blood smears, with Mycoplasma haemocanis copy number estimated assuming 10 μl of blood per smear and 100% extraction efficiency.
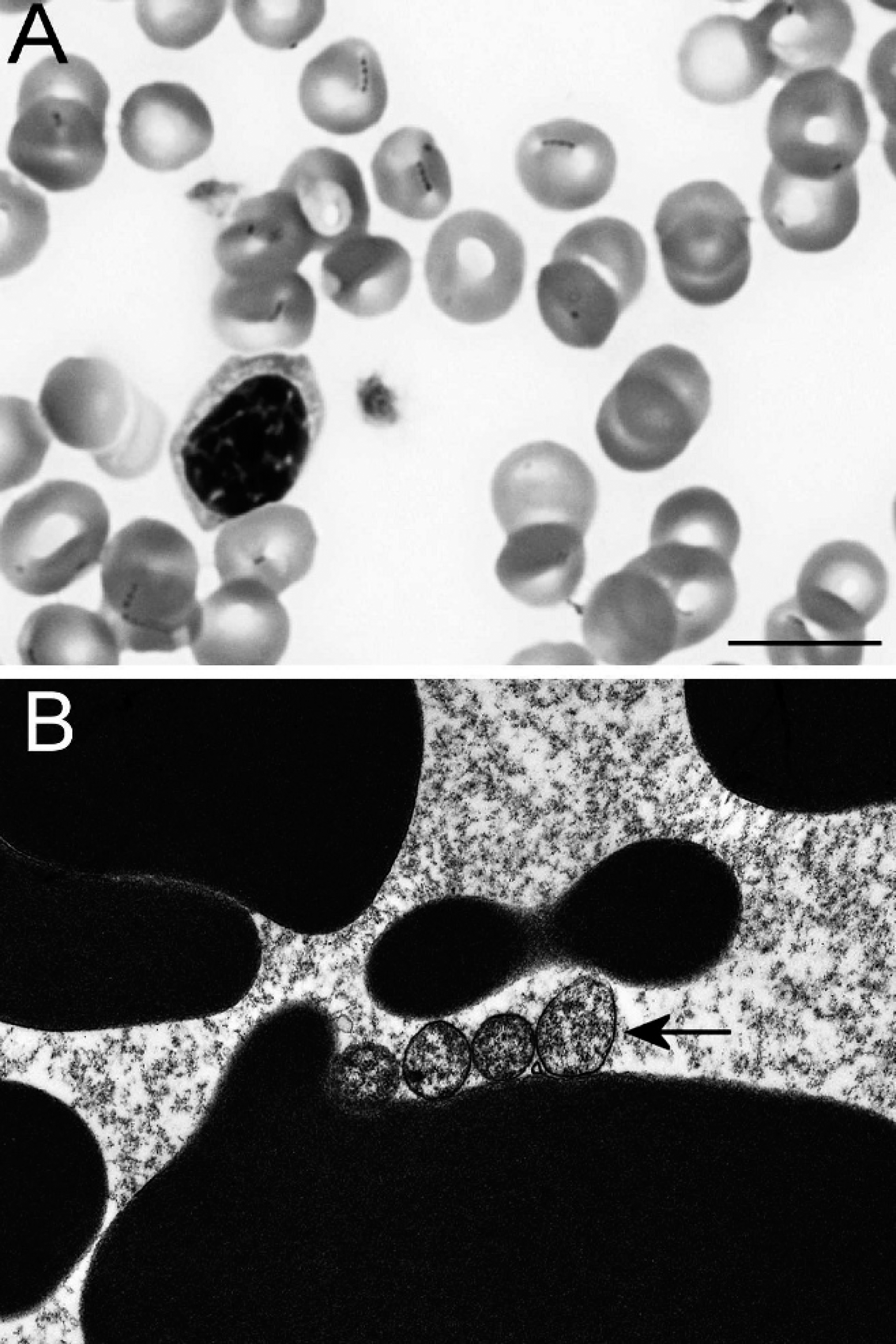
Photomicrographs of erythrocytes from a splenectomized dog infected with Mycoplasma haemocanis.
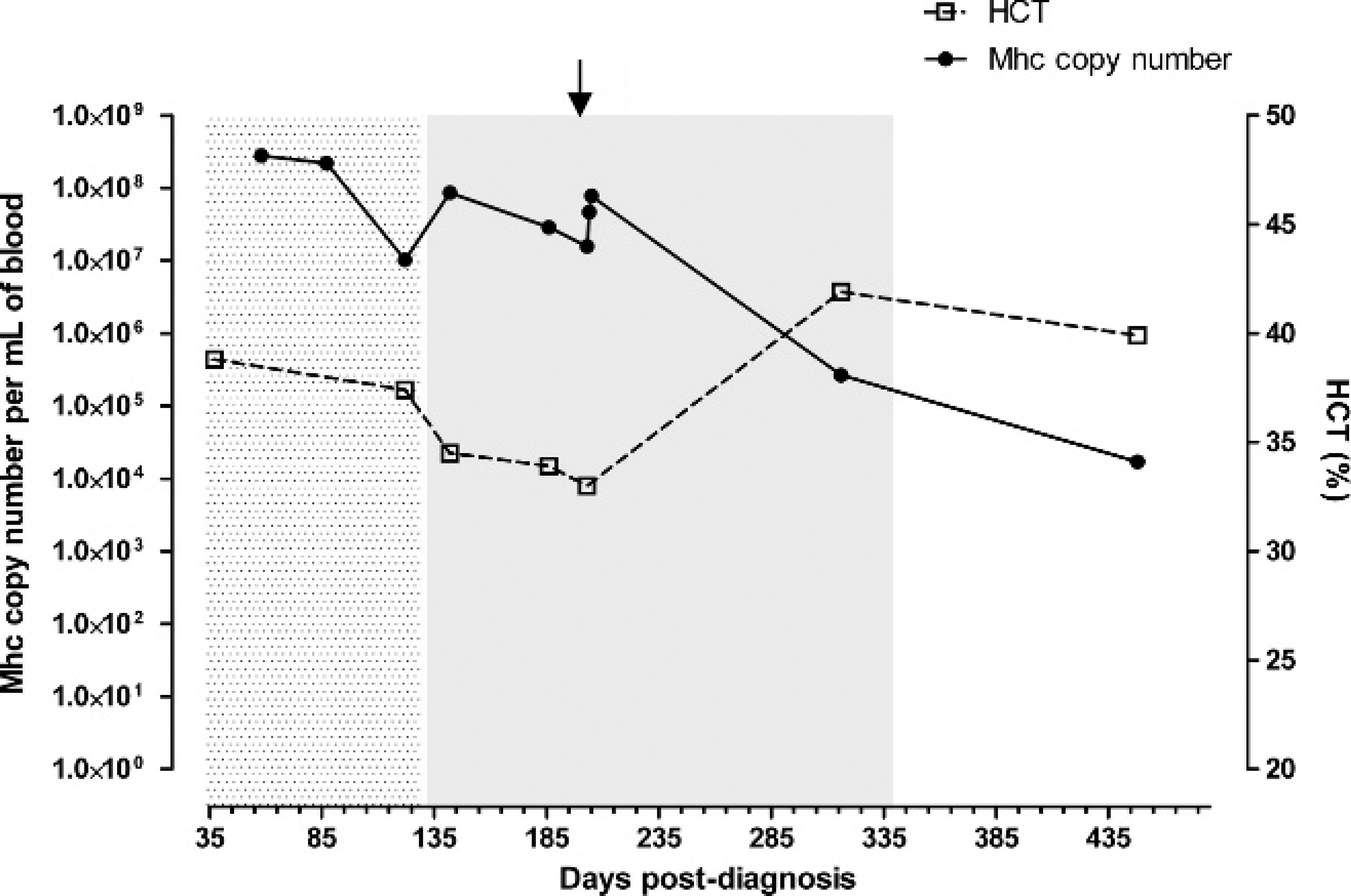
Serial monitoring of Mycoplasma haemocanis (Mhc) copy numbers in whole blood samples during antibiotic therapy, with corresponding hematocrit (HCT) levels. The first stippled region of the graph between days 37 and 100 post-diagnosis indicates when the dog was treated with oxytetracycline (24 mg/kg orally every 8 hr). Between days 100 and 340 postdiagnosis (gray shaded region), the dog received enrofloxacin (5.6 mg/kg orally every 24 hr). After day 340, therapy was withdrawn permanently (unshaded region). The arrow indicates when withdrawal of therapy was attempted but failed. This figure does not show the real-time quantitative polymerase chain reaction results for the first 37 days postdiagnosis (shown in Table 1), as these were obtained using DNA extracted from blood smears and so are not directly comparable with results obtained using DNA extracted from whole blood. Relatively little change in copy numbers was seen during treatment with oxytetracycline and during the first 100 days of treatment with enrofloxacin. However, during the latter stages of enrofloxacin therapy, an inverse relationship between copy numbers and hematocrit becomes apparent, with falling copy numbers associated with an improvement in hematocrit.
To the authors' knowledge, this is the first report of qPCR being used to monitor M. haemocanis infection in a dog. As a result of the first-opinion nature of the case, gaps are present in the collection of samples, and ideal sampling intervals were not always maintained, but this case illustrates the potential usefulness of qPCR for monitoring hemoplasma infection in dogs. Long-term clearance of infection was not achieved in this dog, despite remission of clinical signs. Persistence of chronic asymptomatic infection following acute disease has been noted previously in feline hemoplasmas, 20,21,26 and in these cases, the decision to withdraw therapy may require consideration of qPCR results in combination with other clinicopathological indices. As noted by previous authors, 2,24 blood smear microscopy was an insensitive tool for the detection of Parasitemia, with organisms being absent from most blood smears during the monitoring period.
The ability to analyze DNA from stained blood films was very useful in allowing the retrospective confirmation of diagnosis in the dog in the present study. Blood films, unlike whole blood samples, are frequently stored for prolonged periods at referral testing facilities. These serve to form an archive of material that could potentially be used for retrospective analysis in clinical cases and in larger research studies. In the present case, it was interesting to note that the blood films from day 7 were negative by qPCR. Given the later relapse in clinical disease, it is unlikely that true clearance of infection had occurred. Instead, bacterial concentrations may have decreased below the detection limit of the qPCR when blood smears were used for DNA extraction. The smaller volume of material available for extraction from blood smears (total of approximately 5–10 μl of blood used to make a blood smear, compared to 100 μl used for qPCR analysis of whole blood samples) would have contributed to a decrease in sensitivity. The presence of excessive cross-linking of DNA from the smear preparation and staining process could also not be excluded, although GAPDH was adequately amplified from smears, and previous work has failed to show an adverse effect of fixing and staining on DNA extraction and subsequent qPCR from blood smears (Tasker S, et al.: 2010, Investigation of human hemotropic Mycoplasma infections using a novel generic hemoplasma qPCR assay).
The results of qPCR analysis indicate that neither oxytetracycline nor enrofloxacin were effective in significantly reducing M. haemocanis numbers, although variable control of clinical signs was achieved. These findings are similar to those of a recent study in alpacas, in which treatment with oxytetracycline was not associated with faster clearance of “Candidatus Mycoplasma haemolamae” infection. 24 However, in cats, studies 6,7,20,21,22 using qPCR have demonstrated the effectiveness of both doxycycline and fluoroquinolones in reducing copy numbers of feline hemoplasmas and improving clinical signs, but again, clearance of infection is not always achieved. Given the long duration of treatment with no marked change in M. haemocanis copy numbers, it is likely that the resolution of clinical disease in the present case was due to the development of an effective immune response by the dog. It is known that despite an intense immune response and antibiotic treatment, hemoplasma-infected animals often remain chronic carriers after clinical signs have resolved. 14 Clinicians should be aware that achieving complete clearance may not be possible in all cases of M. haemocanis infection, and the decision to withdraw therapy needs to be based on the complete clinical picture.
The reason for the delayed recovery from acute disease in the present case (after initial return of a qPCR-negative result) is not known. One factor that possibly contributed to the delayed recovery may have been the severe neutropenia that developed during the course of treatment. The cause for the neutropenia was not discovered, but temporally this appeared to coincide with the introduction of enrofloxacin. Gaps in hematological testing made it impossible to confirm this association. Alternatively, the neutropenia could have been due to the hemoplasma infection, either from a direct effect of the organism or indirectly through immune-mediated or myelosuppressive mechanisms. Transient neutropenia has been noted in 2 previous cases of M. haemocanis—associated disease, 3,4 but persistent neutropenia is not otherwise noted in the veterinary literature.
The lack of a spleen may have been an additional contributory factor to the dog's inability to clear the M. haemocanis infection. Most cases of canine hemoplasmosis in the veterinary literature have been reported in splenectomized dogs, but, unfortunately, follow-up data are often limited, and monitoring of M. haemocanis copy numbers has not been previously available. It is therefore difficult to know if the persistent infection in the dog in the present study was a unique finding or whether prolonged parasitemia is seen in many splenectomized dogs. Further information about the incidence of persistent infection in postantibiotic therapy for dogs would be useful for formulating recommendations on qPCR monitoring and for determining when to withdraw therapy. The possibility that a concurrent but undetected illness contributed to the prolonged clinical course in this dog can also not be discounted.
A final feature of interest in the current case was the incongruence between the blood qPCR results and the microscopic findings. As noted previously, organisms were rarely visible on the blood films, despite the detection of high copy numbers by qPCR. The possibility of detachment of organisms from the erythrocytes was considered, but blood films were always prepared immediately after collection, and organisms were not detected in the background of smears. In an interesting parallel, investigators 8 of a highly pathogenic strain of Mycoplasma suis recently showed that these bacteria were able to penetrate porcine erythrocytes and were detected intracellularly within vacuoles and freely within the cytoplasm. The above investigation was initiated after a similar incongruence between copy numbers and smear examination was noted during monitoring of an outbreak in feeder pigs. The authors suggested the marked pathogenicity of the isolate and its resistance to standard antibiotic treatment may have been due to its ability to exist intracellularly. It is not known if other hemoplasma species are able to invade erythrocytes, but the possibility should be considered, particularly given the discordant results noted in the present case.
Acknowledgements
The authors would like to thank the staff of the University of Glasgow Veterinary Clinical Pathology Laboratory for their assistance with sample handling. Dr. Sarinder Day of the University of Bristol is also thanked for her help with the processing of some of the samples. ENB was supported by a University of Bristol Postgraduate Research Scholarship and Pfizer Health Limited. Quantitative PCR analysis of the samples was supported by a grant from The Wellcome Trust (grant WT077718).
Footnotes
a.
Advia 120 analyzer, Siemens Healthcare Diagnostics, Deerfield, IL.
b.
Macherey-Nagel NucleoSpin® Blood kit, ABgene, Epsom, United Kingdom.