
Abstract
Cutaneous toxoplasmosis has been previously reported in human beings, rarely reported in cats, and reported in 1 dog with systemic toxoplasmosis. The present report describes 2 cases of cutaneous toxoplasmosis in 2 dogs treated with immunosuppressive therapy. One of the dogs developed generalized cutaneous pustules and pruritus, and the other dog only had a single subcutaneous nodule. Microscopically, skin biopsies showed moderate to severe pyogranulomatous and necrotizing dermatitis and panniculitis, with multifocal vasculitis and vascular thrombosis. Single or aggregates of protozoal tachyzoites were mostly intracytoplasmic and occasionally extracellular. The etiology was confirmed in both cases by immunohistochemistry and by polymerase chain reaction assays, which were followed by nucleic acid sequencing. Both patients were treated with clindamycin. The dog with generalized lesions developed pulmonary and neurological signs and was euthanized. The dog with a single nodule recovered completely with no remission of cutaneous lesions.
Toxoplasmosis is a disease caused by the coccidian protozoa Toxoplasma gondii, which infects human beings and a wide range of domestic species. Transmission occurs by ingestion of oocysts from feline feces, ingestion of meat from an intermediate host containing cysts, or transplacentally. When ingested, the organisms penetrate the intestinal mucosa and can disseminate through other tissues. Tissue cysts are presumed to persist throughout the life of the host. 8 Reactivation of a latent infection caused by T. gondii is usually characterized by involvement of the central nervous system (CNS), occasionally the lungs, and infrequently other organs, and in most cases, patients that develop clinical disease frequently have concurrent immunosuppression.1,19,22 Cutaneous manifestations of the disease have been reported in human beings1,3-5,17 and rarely reported in cats,2,16,19 and only 1 report describes cutaneous infection in a dog with systemic toxoplasmosis. 22 In the reported cases of cutaneous toxoplasmosis in human patients, the lesions present as erythema multiforme–like eruptions or as a nodular,3,4,17 maculopapular, papulopustular, lichenoid, or vegetative dermatitis. 17 These patients can have systemic signs, including asthenia, fever, joint pain, and lymphadenopathies.3-5 The presence of organisms in skin biopsies is observed in approximately half of the cases, and the diagnosis in the past was usually confirmed by animal inoculation or seroconversion. 17 Currently, polymerase chain reaction (PCR) assay and nucleic acid sequencing can be used to confirm these cases. 1 The current report describes 2 adult dogs treated with immunosuppressive therapy that developed severe cutaneous lesions caused by T. gondii. Diagnosis was confirmed by immunohistochemistry and PCR.
In the first case, a 9-year-old Akita/German Shepherd Dog cross was presented with severe anemia and was clinically diagnosed with immune-mediated hemolytic disease (IMHA) and lower urinary tract infection. The dog was treated with prednisone, cyclosporine, sucralfate, and amoxicillin–clavulanic acid with successful increase and stabilization of the packed cell volume (PCV) and resolution of the urinary tract infection. After 20 days, the dog developed bloody diarrhea and was treated with metronidazole. After an additional 20 days, the dog was reevaluated clinically due to generalized and progressive cutaneous pustules and pruritus. Four skin punch biopsies were collected and submitted to the Dermatopathology Specialty Service at Texas A&M University (College Station, Texas). A few days later, the patient developed respiratory distress, muscle rigidity, and neurological signs and was treated with clindamycin. Due to the poor prognosis and severity of clinical signs, the owners elected euthanasia, but necropsy was not performed.
Histological findings in the submitted biopsies included severe pyogranulomatous inflammation extending from the superficial dermis into the superficial subcutis composed primarily of neutrophils, macrophages, and fragments of necrotic debris (Fig. 1). Multifocally, single or aggregates of 3 × 6-µm, elongated basophilic organisms with a central nuclei (tachyzoites) were mostly within the cytoplasm of endothelial cells, keratinocytes, macrophages, and fibroblasts; however, scattered extracellular organisms were also observed (Fig. 1 inset). Multifocal necrosis was primarily observed around affected blood vessels with vasculitis and vascular thrombosis (Fig. 2).
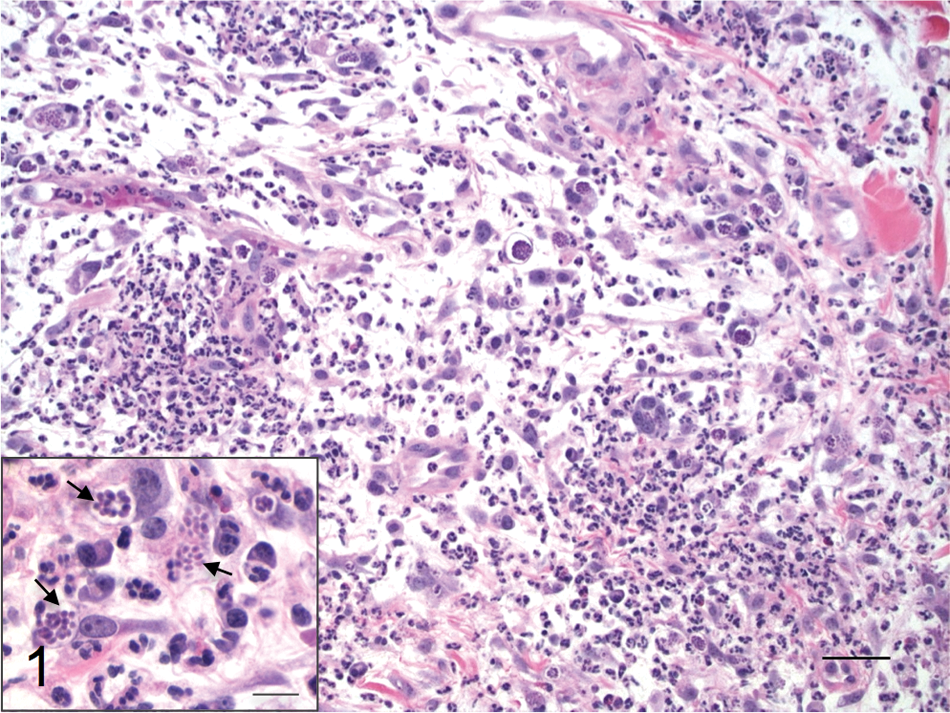
Case 1; dog. The dermis is infiltrated with neutrophils, macrophages, and occasional multinucleated giant cells. Hematoxylin and eosin (HE). Bar = 40 µm. Inset: higher magnification showing large numbers of tachyzoites (arrows) in the cytoplasm of macrophages and fibroblasts. HE. Bar = 20 µm.
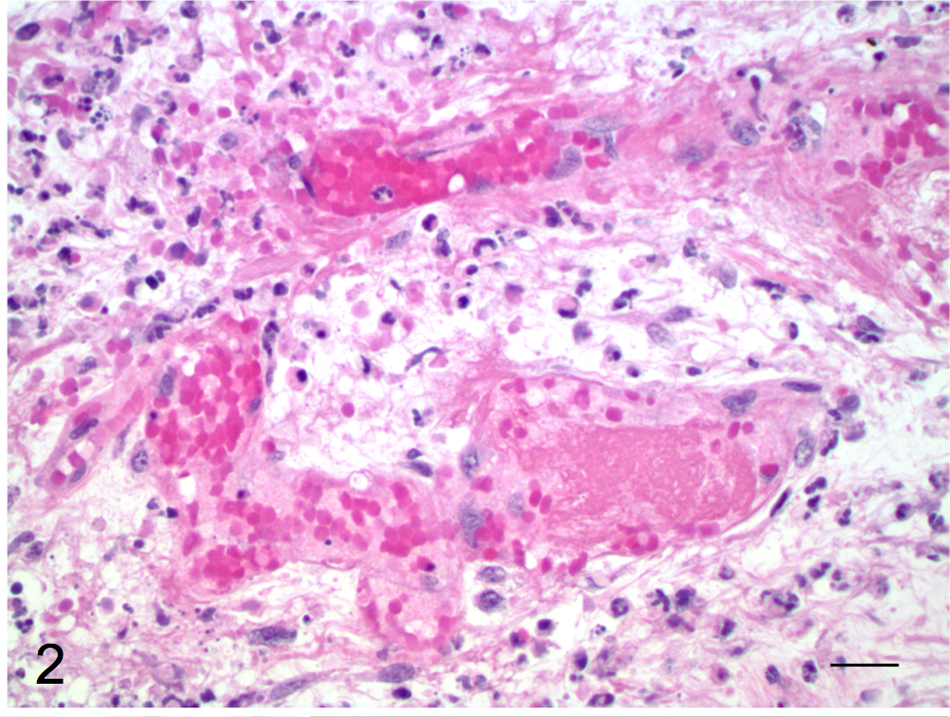
Case 1; dog. Severe necrotizing dermatitis with accumulation of fibrin and necrotic debris, vasculitis, and vascular thrombosis. Hematoxylin and eosin. Bar = 40 µm.
In the second case, a 7-year-old, female, spayed Rhodesian Ridgeback was referred to the Veterinary Medical Teaching Hospital at Texas A&M University (College Station, Texas) for a severe prolonged immune-mediated thrombocytopenia (IMTP), valvular endocarditis, and urinary tract infection. The patient was being treated with prednisone (10 mg/24 hr), aspirin (15 mg/24 hr), azathioprine (50 mg/48 hr), amoxicillin (800 mg/12 hr), and enrofloxacin (306 mg/24 hr) for approximately 3 weeks. The IMTP failed to respond to immunosuppressive therapy, and the prednisone dose was increased to 50 mg/day. After 4 weeks, a raised dermal nodule and plaque were observed on the left shoulder. Protozoal organisms were identified on cytologic examination of the mass. A skin punch biopsy taken from the mass and examined histologically was infiltrated with moderate to large numbers of macrophages, neutrophils, and plasma cells within the mid and deep dermis and subcutis. Occasional macrophages and scattered endothelial cells contained intracytoplasmic, 4–6 µm in diameter, round to oval basophilic tachyzoites, which were occasionally free within the interstitium. Additional findings included necrosis and edema, multifocal vasculitis, scattered venous thrombosis, and follicular and epidermal atrophy. The dog was treated with clindamycin (300 mg/12 hr), as well as the previously prescribed medications except for azathioprine, which was withdrawn due to development of hepatotoxicity. Immunoglobulin titers for trypanosomiasis, toxoplasmosis, and neosporosis were all negative; however, convalescent serum was not tested. Short relapse of IMTP occurred after withdrawal of azathioprine; however, no recurrence of cutaneous lesions or IMTP was observed after 5 years.
Immunohistochemistry for T. gondii and Neospora caninum were performed in paraffin-embedded samples from case 1 and for T. gondii in case 2. Briefly, deparaffinized sections were incubated with polyclonal goat antibodies against N. caninum and T. gondii. a A streptavidin immunoperoxidase labeling procedure was used to demonstrate immune reactions.11,21 Positive immunohistochemical controls included tissues that contained the different parasites to which the appropriate antisera were added. For negative controls, the primary antibodies were replaced with homologous nonimmune sera. The organisms reacted strongly positive for T. gondii in both cases (Fig. 3a) and very weakly positive for N. caninum in case 1 (Fig. 3b).
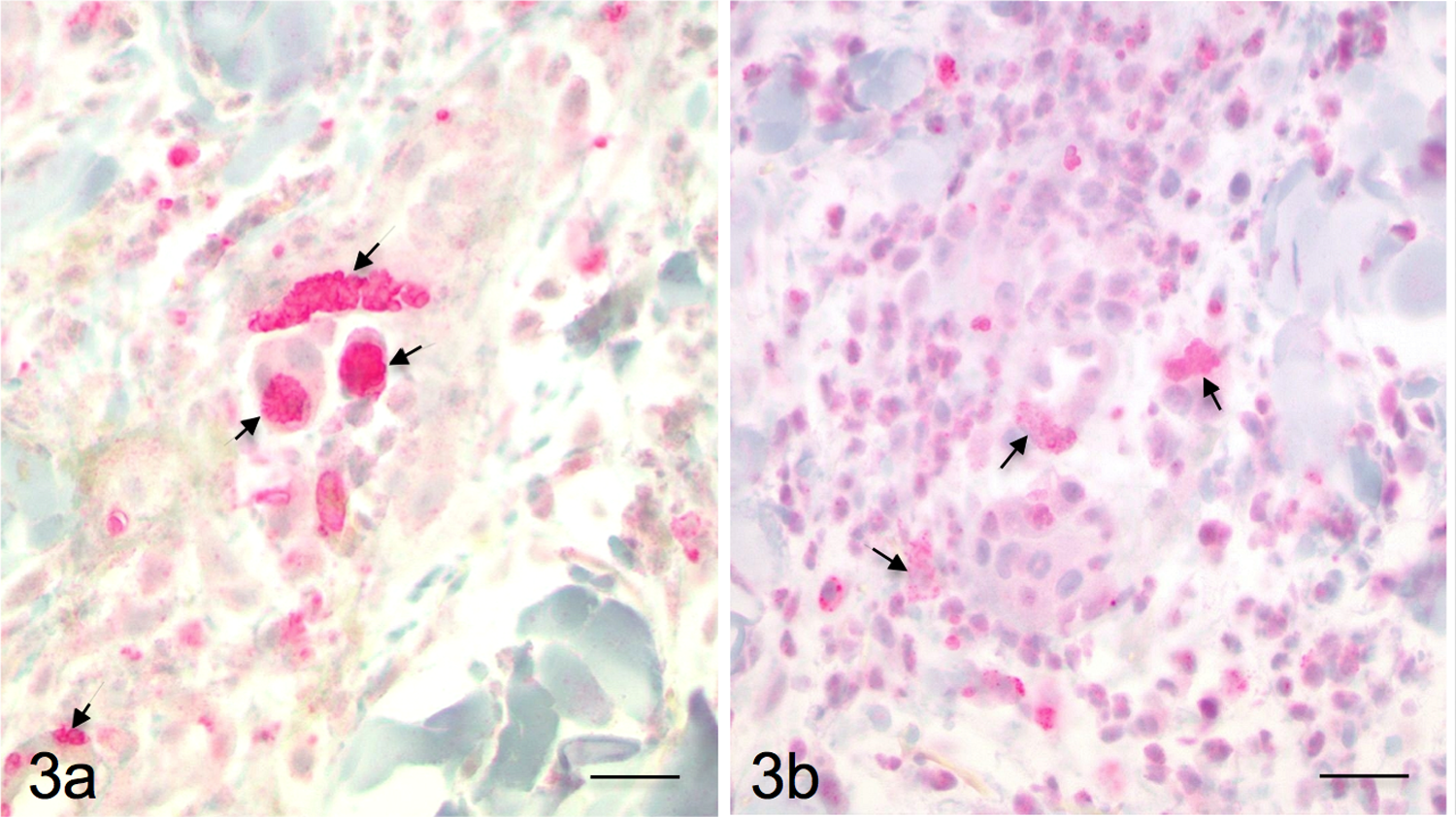
Case 1; dog. Tachyzoites (arrows) are strongly positive for Toxoplasma gondii polyclonal antibody (
The PCR assays for T. gondii and N. caninum were conducted using DNA extracted from formalin-fixed, paraffin-embedded tissue from both dogs. Initially, the T. gondii–specific PCR primers used were derived from the 35-fold repetitive B1 gene.5,6 A second set of T. gondii–specific PCR primers was derived from the 300-fold 529-bp T. gondii genomic repeat.10,18 The N. caninum–specific PCR primers were derived from the NC5 gene. 12 The PCR amplicons were further submitted to the Research Technology Support Facility at Michigan State University (East Lansing, Michigan) for nucleic acid sequencing. The PCR assay for the B1 gene of T. gondii was positive for both dogs (Fig. 4), and the PCR assay for the NC5 gene of N. caninum was negative for both dogs. In addition, the PCR assay for the 300-fold genomic repeat from T. gondii was positive for the dog from case 1. All of the PCR assays showed no cross-reactivity among organisms when tested with genomic DNA from each organism (data not shown). The PCR amplicons of the B1 gene from both dogs were 99% homologous with the nucleic acid sequences of the T. gondii 35-fold repetitive B1 gene (GenBank accession no. AF179871). The PCR amplicon of the 300-fold T. gondii genomic repeat from the dog in case 1 was 100% homologous to nucleic acid sequences for that repeat (GenBank accession nos. DQ779192 and EF195646). The PCR and nucleic acid sequences confirmed that the cutaneous lesions in both dogs were due to infection with T. gondii.
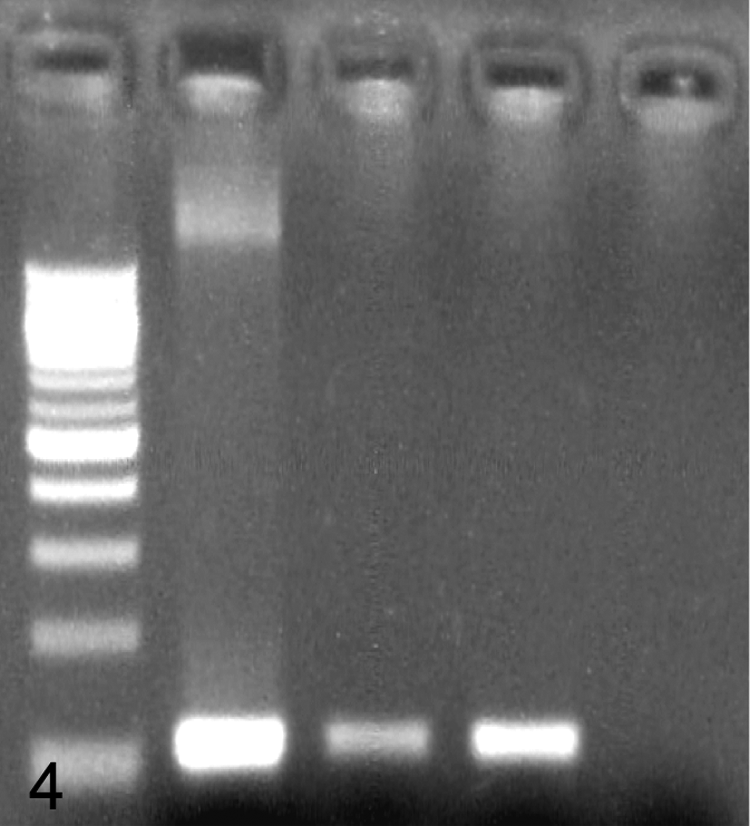
Polymerase chain reaction for detection of Toxoplasma gondii. Lane 1: 100-bp DNA ladder; lane 2: case 1; lane 3: case 2; lane 4: positive control; lane 5: negative control.
Cutaneous toxoplasmosis is a rare to uncommon manifestation of the infection by T. gondii described in human beings1,3-5,17 and in a few domestic animal species.2,13,16,19,22 Even though a high percentage of animals are serologically positive for toxoplasmosis, only a few animals develop clinical disease. It is speculated that concomitant illness or immunosuppression may cause a host to become more susceptible to proliferation of T. gondii and development of clinical disease. 8 Most of the cases of cutaneous toxoplasmosis described in human beings have occurred in immunosuppressed patients and occasionally as a severe complication of hematopoietic stem cell transplantation.1,21 In both dogs described in the present report, as well as in the previously described case of cutaneous toxoplasmosis in a dog, 22 cutaneous lesions developed after the dogs received immunosuppressive therapy for treatment of IMHA or IMTP, which likely resulted in reactivation of a latent infection of T. gondii.
In human patients, cutaneous lesions can present as erythema multiforme–like eruptions or as a nodular, maculopapular, papulopustular, lichenoid, or vegetative dermatitis. Those patients may have systemic signs that include asthenia, fever, joint pain, and lymphadenopathies. The clinical lesions of cutaneous toxoplasmosis in cats can present as a single cutaneous nodule 19 or as multiple ulcerated and nonulcerated cutaneous nodules.2,7 The cutaneous lesions in the previously reported case in a dog were characterized by multiple raised, alopecic, and ulcerated nodules with some nodules exuding purulent material. 22 One of the dogs in the present report developed a generalized pustular dermatitis with significant pruritus, whereas the other affected dog only had a single cutaneous raised nodule on the shoulder.
Histologically, the previously described cases of cutaneous toxoplasmosis in cats and a dog were characterized by a necrotizing and granulomatous or pyogranulomatous dermatitis and panniculitis with vasculitis. Epidermal hyperplasia and hyperkeratosis can occur as well. The protozoal organisms can be single or arranged in clusters, some of which are extracellular or within the cytoplasm of follicular, epidermal, and glandular epithelial cells; macrophages; fibroblasts; and endothelial cells. The organisms are approximately 2 × 6 µm in size and have a crescent shape with a pale basophilic cytoplasm and a dark nucleus (tachyzoites).2,7,19,22 Identification of organisms in histologic lesions can be a challenge in some cases. Even though organisms were abundant within the lesions of case 1, only scattered to rare organisms were observed within the lesions of case 2. In human patients serologically positive for antibody against T. gondii with cutaneous histologic lesions strongly suggestive of toxoplasmosis, organisms are only identified histologically in approximately 50% of the cutaneous lesions. Similar findings have also been observed in cats that have systemic toxoplasmosis with ulcerative skin lesions and vasculitis, presumed to be caused by T. gondii; however, organisms were not identified in histologic sections of affected skin. 7 Also, similar histologic cutaneous lesions and morphologically similar protozoal organisms are observed in animals infected with N. caninum, making histologic differentiation between these 2 organisms virtually impossible.8,20
For this reason, confirmation of clinical cases based only on histopathology of skin might be insufficient, as in numerous cases, identification of characteristic organisms can be challenging.1,2,7,8,14,15 In the past, clinical diagnosis in these patients was usually confirmed by animal inoculation or seroconversion against T. gondii.1,7,17 However, serologic techniques may be nonspecific and may lack sensitivity.2,7,22 To overcome such problems, immunohistochemistry (IHC), PCR, and transmission electron microscopy can be used to confirm the diagnosis. Even though IHC using polyclonal antibodies against T. gondii is considered sensitive, positive results might not be conclusive, due to moderately low specificity of polyclonal antibodies that can cross-react between T. gondii and N. caninum. 2 Cross-reaction was observed in case 1 of the present report; however, immunolabeling was very strong for T. gondii and very weak for N. caninum. Polymerase chain reaction is considered a more accurate technique for the diagnosis of T. gondii, being useful for early detection of T. gondii infection in people and animals, especially in asymptomatic cases.1,14 Transmission electron microscopy can be used to detect structural differences between these 2 organisms, 8 but in occasional cases, these organisms can be indistinguishable due to many ultrastructural similarities shared by T. gondii and N. caninum tachyzoites.
Clindamycin, trimethoprim, and sulfa combination are the most commonly used drugs against toxoplasmosis in animals, and azithromycin and ponazuril are also effective to treat the infection. 8 Clindamycin has been successfully used to treat fever, myositis, uveitis, and CNS disease in animals, even though gastrointestinal irritation can occur in some treated animals.8,9,13 Clinical signs not related to the CNS usually resolve within a few days after treatment, with ocular and CNS toxoplasmosis responding more slowly to therapy, although it is believed that no drug can completely clear T. gondii from the body. Unfortunately, the prognosis is usually poor in dogs and cats that develop disseminated toxoplasmosis. 8
In conclusion, even though rarely described, cutaneous toxoplasmosis occurs in dogs and other species, especially if these patients are immunosuppressed. Diagnosis confirmation can be a challenge in similar cases; however, the use of proper diagnostic techniques can improve conclusive diagnosis of toxoplasmosis in animals.
Footnotes
a.
VMRD Inc., Pullman, WA.
The author(s) declared that they had no conflicts of interest with respect to their authorship or the publication of this article.
The author(s) declared that they received no financial support for their research and/or authorship of this article.