
Abstract
Measurement of low concentrations of C-reactive protein (CRP) in dogs has previously been performed with nonautomated assays. The aim of this study was to validate an automated high-sensitivity CRP (hsCRP) assay, developed by modifying a routinely used canine-specific immunoturbidimetric CRP test (cCRP). Imprecision, linearity under dilution, limit of blank (LOB), limit of detection (LOD), and limit of quantification (LOQ) were determined for the hsCRP test, as well as the presence of prozone effect and interferences. The imprecision, measured as intra-assay variation, was ≤2.7%. The assay was acceptably linear under dilution. An analytically relevant prozone effect was present for samples with CRP concentration >150 mg/L, and there were mild interferences from hemolysis and lipemia. The LOB, LOD, and LOQ were 0.10 mg/L, 0.22 mg/L, and 0.50 mg/L, respectively. A method comparison study with a canine-specific enzyme-linked immunosorbent assay (ELISA) was performed, showing poor agreement between the hsCRP test and the ELISA. An additional aim of the study was to apply the hsCRP test to clinical research samples. Serum samples from 7 dogs undergoing ovariohysterectomy were collected pre- and postoperatively, and CRP was measured with both the cCRP and hsCRP assay. The expected postoperative increase in CRP was detected earlier with the hsCRP test, compared with the cCRP test. The hsCRP assay was further applied on samples from 6 lean and 9 overweight dogs. There was no significant difference in CRP concentration between the groups (P = 0.06). In conclusion, the hsCRP test had acceptable analytical performance, and the assay was successfully applied to clinical research samples.
Introduction
C-reactive protein (CRP) is a major positive acute phase protein (APP) in dogs, produced in the liver in response to increased concentrations of pro-inflammatory cytokines.4,9 The hallmark of a major APP is a low blood concentration in the healthy dog, and a rapid and marked increase during inflammation.4,9 This makes major APPs such as CRP valuable as clinical markers for diagnosing and monitoring inflammatory diseases in veterinary medicine.4,9,12,26 In people, the use of CRP has extended beyond the role as a mere diagnostic test, and the association between this biomarker and lifestyle-related diseases such as obesity, diabetes mellitus, and cardiovascular disease is gaining increasing interest.8,33 In this context, assays have been developed that measure CRP in the low or ultra-low concentration range, and these tests are then referred to as high-sensitivity CRP (hsCRP) assays. The hsCRP test is different from the routinely used CRP test regarding methodology applied, purpose of testing, and interpretation of the results. Examples of applications of hsCRP testing in human beings are to assess the risk of future cardiovascular disease,15,34,35,40 and as a prognostic marker in cancer. 1 Similarly, measurements of CRP concentrations in the low range have been performed in dogs in a research setting. It has been investigated if obesity in dogs is associated with increased CRP concentrations,11,37 as it is in people,5,32 and the association between cardiac disease and CRP concentrations has been studied.7,25 In order to investigate minor changes in CRP concentrations in the low range in dogs, routine CRP tests such as the previously validated immunoturbidimetric assays10,14,20 are not suitable. These tests are developed for assessing moderately to markedly increased CRP concentrations in ill dogs, and they are neither sufficiently accurate nor precise at low CRP concentrations. Instead, tests such as enzyme-linked immunosorbent assay (ELISA) 21 and time-resolved immunofluorometric assay (TR-IFMA) 31 have been used; these assays have low limits of detection (LODs) and can therefore be considered as hsCRP methods. However, no automated hsCRP test is currently available for use in dogs to our knowledge.
The aim of this study was to validate an automated canine-specific hsCRP assay. An additional aim was to apply this test for analyzing CRP in serum samples collected for clinical research purposes. We hypothesized that the hsCRP test could detect increased CRP concentrations earlier in postoperative samples from dogs undergoing surgery, compared with the routinely used canine-specific CRP test. Second, we hypothesized that overweight dogs would have higher CRP concentrations compared to lean dogs.
Material and methods
A method validation study was performed to establish the analytical performance of the hsCRP assay. After satisfactory completion of the validation study, the hsCRP test was applied to serum samples from 2 clinical research studies.
Animals and samples
Method validation study
Blood samples were collected for diagnostic purposes from canine patients admitted to the University Animal Hospital at the Swedish University of Agricultural Sciences (UDS-SLU; Uppsala, Sweden), in tubes with clot activator. a Sera were prepared by centrifugation at 2,000 × g for 5 min, and stored in cryotubes b at −20°C for a maximum of 4 weeks. Samples were thawed at room temperature and thoroughly mixed immediately prior to analysis.
Clinical research studies
The current studies were approved by the Local Ethical Committees in Uppsala, Sweden. Informed owner consent was obtained prior to sampling. Blood samples were collected by venipuncture in tubes with clot activator. a Sera were prepared as described above, and were frozen in cryotubes. b
C-reactive protein after surgery
The ability of the hsCRP test to detect a postoperative increase in CRP concentration was investigated, and then compared with the performance of the routinely used canine-specific immunoturbidimetric CRP (cCRP) assay, c on which the hsCRP test was based. Dogs undergoing ovariohysterectomy (OHE) at UDS-SLU were sampled immediately prior to surgery (baseline) and 2, 4, 6, and 8 hr after the start of surgery, defined as the time point of the initial skin incision. Inclusion criteria were that the dog had an elective open approach OHE, and that the preoperative CRP concentration measured with the cCRP assay was <6.8 mg/L, which was the reference interval for CRP at UDS. Samples were stored at −80°C for a maximum of 3 months prior to analysis.
C-reactive protein in lean and overweight dogs
To study CRP concentrations in lean and overweight dogs, serum samples were obtained from healthy intact male Labrador Retrievers 3−6 years of age. The dog owners were interviewed concerning the health status of their dogs, and routine hematology and biochemistry profiles and urinalysis were performed in all dogs.
All dogs underwent routine clinical examination, which also included visual evaluation of spontaneous lameness in walk and trot on a straight track, as well as examination of oral health status in nonsedated animals. Only dogs reported to be healthy by their owners, without significant abnormal findings on clinical examination and with laboratory test results within the reference intervals, were included in the study. The body condition score (BCS) was determined as previously described 24 by a single examiner, and dogs were allocated to either a lean group (BCS ≤ 5) or an overweight group (BCS ≥ 6). Samples were stored at −70°C for a maximum of 12 months prior to analysis.
C-reactive protein analysis
Validation study
C-reactive protein was measured with a hsCRP assay, which was based on a previously validated, canine-specific immunoturbidimetric CRP method.c,14 In this assay, polyclonal chicken anti-canine CRP antibodies react with CRP in a serum sample, causing an increased turbidity that is measured spectrophotometrically. In the original assay, 2 μL of serum sample was mixed with 70 μL of reagent containing anti-CRP antibodies. To develop the hsCRP test, the assay application was modified by increasing the sample volume 10-fold to 20 μL, whereas the reagent volume was kept unchanged. The calibrator kit of the original CRP assay was used to create the calibrator curve for the hsCRP test, after manually prediluting the calibrators 1:10 with 0.9% NaCl immediately prior to calibration. Analyses were performed on a fully automated, open-system clinical chemistry/immunoassay analyzer. d Two control pools made of pooled canine sera were analyzed once daily during the experiment.
Clinical research studies
Serum samples from dogs undergoing surgery were analyzed with the hsCRP and the cCRP assay in duplicates in a single run. The limit of quantification (LOQ) of the cCRP assay was 6.8 mg/L, and samples below this limit were reported as <6.8 mg/L. Samples from the lean and overweight dogs were first analyzed with a previously validated human immunoturbidimetric CRP assaye,20 calibrated with canine CRP. f All samples that had CRP concentrations <30 mg/L were thereafter reanalyzed with the hsCRP assay in duplicates in a single run.
Quality goals and determination ofassay characteristics
Quality goals were derived from data of biological variation in healthy dogs, 22 as recommended. 19 The maximal allowable imprecision (CVmax) was set to 12%, the maximal allowable bias (biasmax) to 9.5%, and maximal allowable total error (TEa) to 29.6%. 22 The maximal optimal imprecision (CVopt), bias (biasopt), and total error (TEopt) were 6.1%, 4.8%, and 14.8%, respectively.13,22
The within-run imprecision was determined by analyzing 3 serum samples in 15 replicates in 1 run, and the between-run imprecision by measuring 3 samples once daily on 5 consecutive days; the latter samples were frozen in aliquots to avoid repeated freeze–thaw episodes. The intra- and interassay variations, expressed as coefficients of variation (CV), were calculated and compared to CVmax and CVopt. No recalibration was performed during the imprecision study.
In a study of linearity under dilution, a sample with CRP concentration near the upper end of the assay range was used. The sample was manually diluted with 0.9% NaCl to obtain 11 samples with concentrations of 0.9, 0.8, 0.7, 0.6, 0.5, 0.4, 0.3, 0.2, 0.1, 0.05, and 0.025 times the original concentration. Samples were analyzed in duplicate in a single run.
Inaccuracy was further tested in a spike and recovery study. A serum pool with low CRP concentration (base pool) was spiked with 4.7 mg/L and 8.7 mg/L of purified canine CRP. f The base pool and the spiked samples were analyzed in triplicate, and recovery of the spiked amount was calculated. Acceptable recovery after spiking was set to 80–120%.
Presence of prozone effect was evaluated by analyzing 6 serum samples with both the hsCRP and cCRP assay. The CRP concentrations and the absorbances reported by the hsCRP method were compared to the CRP concentrations obtained with the cCRP method, which has no analytical relevant prozone effect up to at least 1,200 mg/L. 14 An analytical relevant prozone effect was considered to be present if samples with high CRP concentrations were reported to be false-low by the hsCRP assay.
The limit of blank (LOB) was determined by analyzing a blank sample, 0.9% NaCl, 20 times in a row. LOB was calculated as follows 28 :

The limit of detection (LOD) was calculated according to the following formula 28 :

where the standard deviation (SD) of a low sample was determined by analyzing a sample with an expected CRP concentration of 0.25 mg/L, 10 times in a row.
The LOQ, the lowest amount of analyte in a sample that can be quantitatively determined with stated acceptable imprecision and trueness, 28 was established. A start sample with a CRP concentration of approximately 8 mg/L, as determined by the hsCRP assay, was manually diluted with 0.9% NaCl to the expected concentrations of 1.0, 0.5, and 0.25 mg/L. The diluted samples were analyzed 10 times in a row on 2 different days, with a recalibration performed between the 2 days. The start sample was analyzed in triplicate on both days. Bias in this experiment was defined as the difference between the observed mean value and the expected value, which was based on the concentration of the start sample and dilution factors. Imprecision was calculated as the CV value of the replicate measurements. The lowest concentration that had TE smaller than TEa (29.6%) was set as the LOQ of the assay.
Interference from hemolysis and lipemia was tested as previously described. 14 A hemolytic solution was prepared according to Clinical and Laboratory Standards Institute guidelines, 6 and a commercial fat emulsion g was purchased for testing lipemia. Test pools were created by adding interferents to serum samples, to obtain 3 hemolytic test pools and 3 lipemic test pools. The final concentrations of hemoglobin in the test pools were 5 g/L and 10 g/L, and final triglyceride concentrations were 10 g/L and 25 g/L. Control pools were made with the same serum samples used for creating the test pools, but, instead of an interfering substance, the same volume of 0.9% NaCl was added to create hemolytic control pools, and the same volume of distilled water was added to create lipemic control pools. All samples were measured in triplicate. An interfering effect causing a change in CRP concentration of ≤10% was considered acceptable.
The hsCRP method was compared with a previously validated canine high-sensitivity CRP ELISA,h,21 in order to investigate if the methods could be used interchangeably. According to the manufacturer, the reportable range of the ELISA was 3.75–60 mg/L when a 1:500 predilution of samples was taken into account. To optimize the assay for samples in the low range, samples in this study were prediluted 1:100, corresponding to a reportable range of 0.75–12 mg/L. The exact LOQ of the ELISA was not investigated, and 0.75 mg/L was set as the concentration corresponding to LOQ. To evaluate performance of the ELISA after modification, linearity was assessed by serial diluting a serum sample with CRP concentration of approximately 10 mg/L. The diluted samples were analyzed in triplicate in 1 run, and the ELISA was found to be acceptably linear using the same acceptance criteria as for the hsCRP study (data not shown). The imprecision of the ELISA, calculated as CV value of the triplicate measurements, was lower than the CV value for intra-assay variation reported by the manufacturer (6.5–6.9%). With the exception of the modified predilution step, the ELISA testing was performed according to the manufacturer’s instructions.
In the method comparison study, serum samples were analyzed in duplicate with both methods within 2 hr using a single 96-well ELISA plate. The CVs of the duplicate measurements were calculated, and if it was higher than CVmax (12%) with either of the methods, the sample was excluded. Two canine serum control samples were analyzed with both methods.
Statistical analysis
Method validation study
Statistical analyses were performed using a statistical software program. i Arithmetic means, SDs, and CVs were calculated using routine descriptive statistics.
Linearity under dilution was evaluated by visual inspection, and by first-order and polynomial regression analysis, 27 with a significance level of α = 0.05. Statistical nonlinearity was present if the second- or third-order model had better fit than the first-order model. Analytical relevant nonlinearity was present if the difference in CRP concentration predicted by the linear model and the best-fitting model exceeded TEa.
In the study of interference, samples were measured in triplicate (n = 3). This number of replicates was required for detecting interference with 95% confidence and power, and was calculated by the following formula 6 :

where α = 0.05, β = 0.05, s = within-run precision of the method, and dmax = maximum allowable difference caused by interference (±10%). The difference in concentration between the test pool and control pool (dobs) was calculated. The 95% confidence intervals (CIs) for dobs were calculated according to the following equation 6 :

The acceptance limits, expressed in mg/L, were ±0.1 ×CRPcontrol pool. If the 95% CI of dobs was within the acceptance limits, it was concluded with 95% confidence that no interfering effect was present.
In the method comparison study, a Bland–Altman plot including the 95% limits of agreement was used to evaluate the difference between methods. 2 The mean difference (dmean) between the methods and the SD of the differences (SDdiff) were calculated. The 95% limits of agreement were calculated by the formula dmean ± 1.96 × SDdiff, and the area between the upper and lower limit in the plot represented the range in which 95% of the differences between the methods were expected to be.
Clinical research studies
Statistical analyses were performed using a commercially available software program. j Data was examined graphically, and normality was assessed using the Anderson–Darling test. Log transformation was performed on nonnormal distributed data. To investigate at which time point after surgery an increase in CRP could be detected compared to the baseline, data was log-transformed and evaluated with a paired t-test with Bonferroni correction. A 2-sample t-test was used to compare CRP concentrations in lean and overweight dogs, after log-transformation of data. CRP concentrations <LOQ were assigned a value of 0.5 × LOQ for the statistical analyses. The significance level was set at P < 0.05.
Results
Method validation study
The modified calibrator curve ranged from 0 to 30 mg/L. In the imprecision study, the CV values were lower than CVopt (6.1%) for all tested samples (Table 1). In the study of linearity under dilution, data was evaluated visually by comparing the observed concentration for each diluted sample with the expected concentration (Fig. 1). The third-order polynomial regression model showed best fit, indicating the presence of statistical nonlinearity. The difference in predicted CRP concentration by the first- and third-order model was <TEa for all samples, except for the sample with lowest CRP concentration. For this sample, linear regression predicted a value of 0.42 mg/L, compared to the value of 0.67 mg/L predicted by the third-order model. When the analysis was repeated with the lowest sample excluded, the difference between the first- and third-order model was <TEa for all samples.
Imprecision for an automated canine-specific high-sensitivity C-reactive protein assay.*
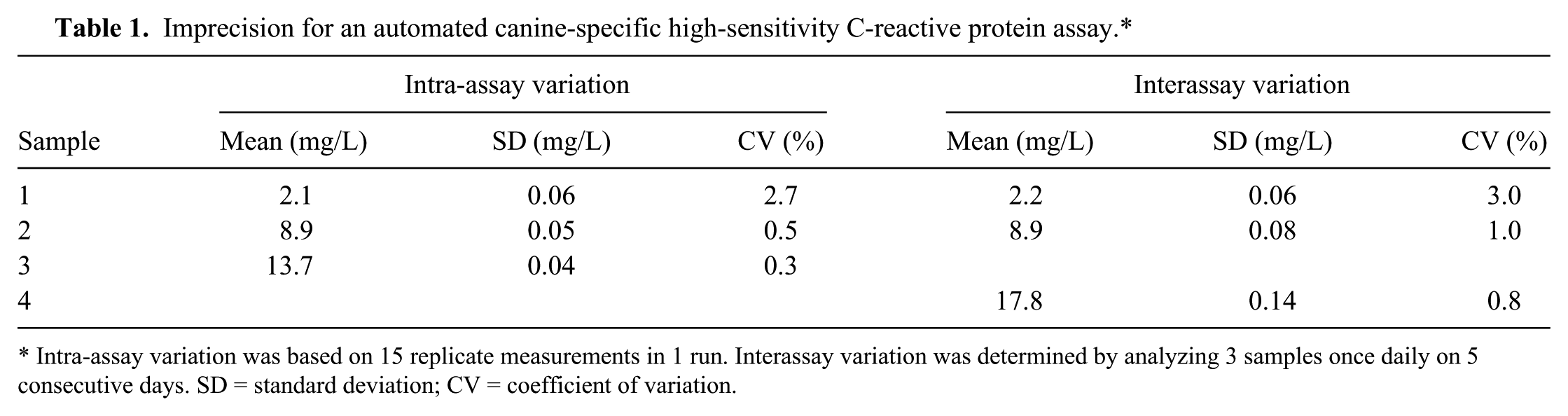
Intra-assay variation was based on 15 replicate measurements in 1 run. Interassay variation was determined by analyzing 3 samples once daily on 5 consecutive days. SD = standard deviation; CV = coefficient of variation.
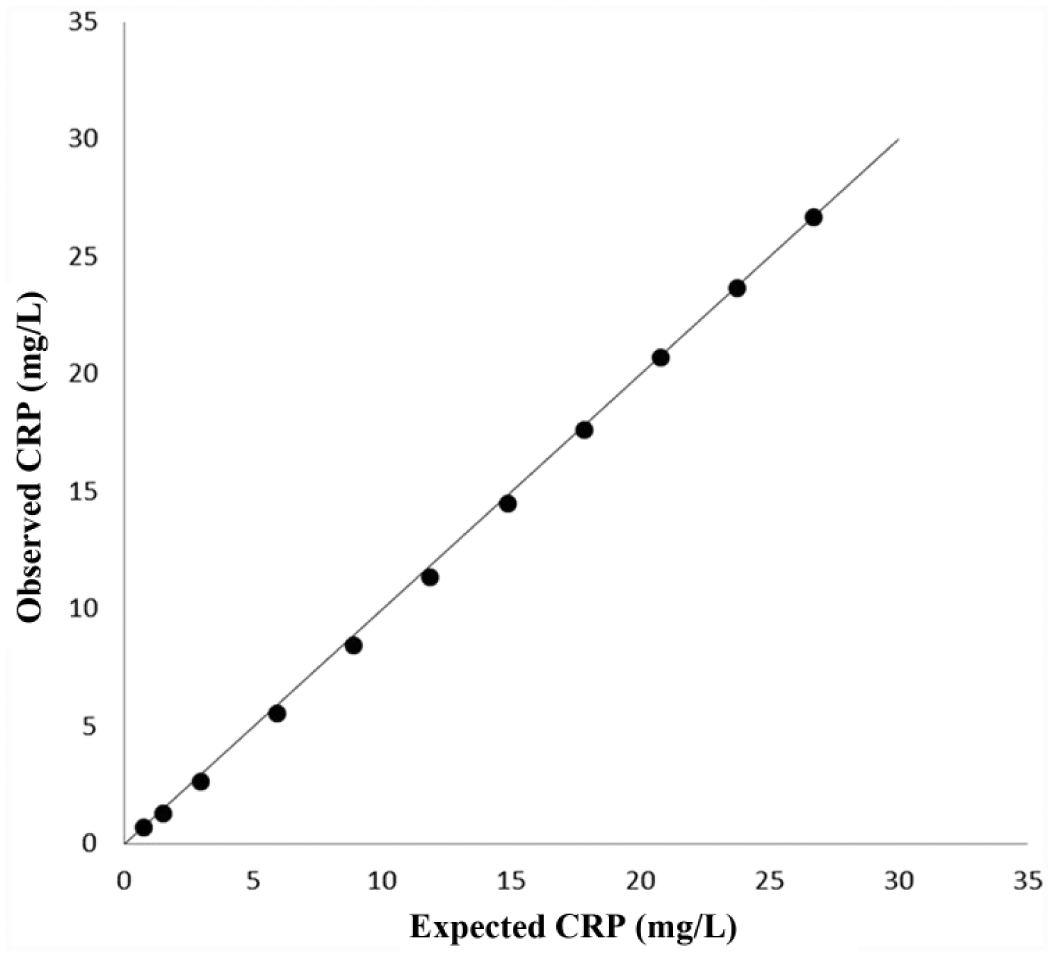
Linearity under dilution for an automated canine-specific high-sensitivity C-reactive protein (hsCRP) assay.
In the spike and recovery study, the base pool had a CRP concentration of 3.30 mg/L, and the recoveries after spiking were 114% and 117%, respectively. An analytical relevant prozone effect was present for samples with CRP concentrations greater than ~150 mg/L (Fig. 2). Two samples with CRP concentrations of 228 mg/L and 311 mg/L had absorbances that were lower than the absorbance of the upper calibrator of the hsCRP assay. The CRP concentrations of these samples were reported to be 20 mg/L and 14 mg/L, respectively, instead of being correctly reported as >30 mg/L by the assay. LOB and LOD was 0.10 mg/L and 0.22 mg/L, respectively. The LOQ was set to 0.5 mg/L; TE at this concentration was 26.5%, which was lower than TEa of 29.6%. At the expected concentration of 0.25 mg/L, TE was 70.3%. The CV values for the samples with expected CRP concentrations of 1.0 mg/L, 0.5 mg/L, and 0.25 mg/L were 4.7%, 9.0%, and 29.3%, respectively. Interference from hemolysis was present at 10 g/L hemoglobin in a sample with CRP concentration of approximately 3 mg/L, but not in the other tested hemolytic samples (Table 2). In the experiment in which a commercial fat emulsion was added to serum, no interfering effect was detected at a triglyceride concentration of 10 g/L, and only minor interference was present at a triglyceride concentration of 25 g/L (Table 2).
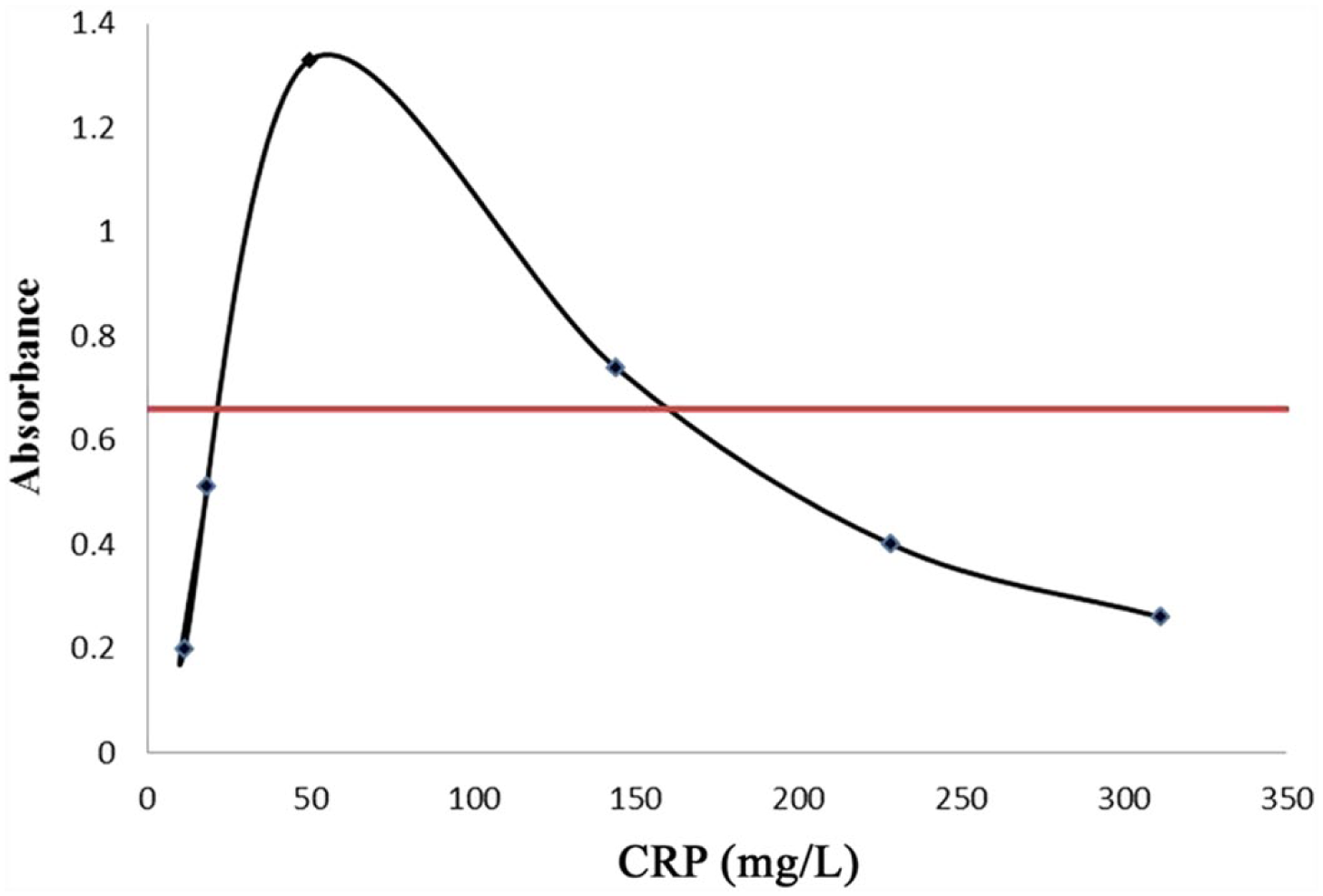
Prozone effect with the automated canine-specific high-sensitivity C-reactive protein (hsCRP) assay. The absorbance with the hsCRP assay was plotted against the CRP concentration as determined by the canine-specific (c)CRP assay. The horizontal line illustrates the absorbance of the top calibrator of the hsCRP assay with a concentration of 30 mg/L. An analytical relevant prozone effect was present, because in the 2 highest samples the absorbances were lower than the absorbance of the upper calibrator of the hsCRP assay.
Interference from hemolysis and lipemia for an automated canine-specific high-sensitivity C-reactive protein (CRP) assay.*
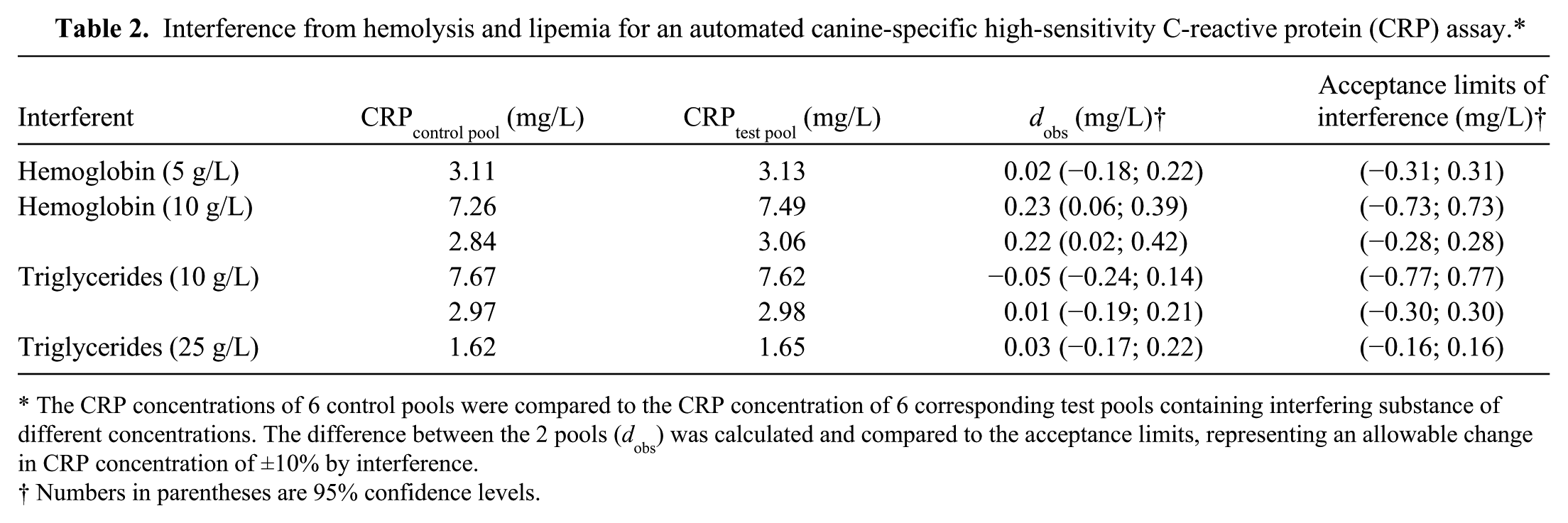
The CRP concentrations of 6 control pools were compared to the CRP concentration of 6 corresponding test pools containing interfering substance of different concentrations. The difference between the 2 pools (dobs) was calculated and compared to the acceptance limits, representing an allowable change in CRP concentration of ±10% by interference.
Numbers in parentheses are 95% confidence levels.
In the method comparison study, 40 patient samples were included. No samples were excluded because of unacceptable CV of duplicate measurements (>12%); the median CV values of the duplicate measurements were 3.0% for the ELISA and 0.9% for the hsCRP assay. Three samples had CRP concentrations <LOQ with both methods, and 4 samples had concentrations above the upper limit of the ELISA (12 mg/L). For the remaining 33 samples, visual inspection of the difference plot revealed a marked difference between the methods (Fig. 3). Because the differences between the 2 methods increased with increasing CRP concentrations, data was log-transformed before calculating the 95% limits of agreement (Fig. 4). The log-transformed bias was −0.56 and the 95% limits of agreements (95% CI) were −1.14 (−1.32; −0.96) and 0.02 (−0.16; 0.20). The anti-logs of the lower and upper limits of agreement were 0.32 and 1.02, respectively. The interpretation was that in 95% of the cases, the hsCRP assay will measure CRP concentrations between 0.32 and 1.02 times the ELISA concentration. This difference was larger than could be accepted based on the predetermined TEa (29.6%). In method comparison studies, the imprecision of both methods should be considered; when measuring samples in duplicate with both methods, as performed in the current study, this will cause the SD of the difference to be lower than if single measurements are performed. This can be corrected when calculating the limits of agreement 2 ; however, because it had already been concluded that the methods did not agree, further calculations were not performed in this study.

Bland–Altman difference plot for C-reactive protein (CRP) concentrations in canine sera measured with an automated immunoturbidimetric canine-specific high-sensitivity CRP assay (hsCRP) and a canine-specific enzyme-linked immunosorbent assay (ELISA; n = 35).
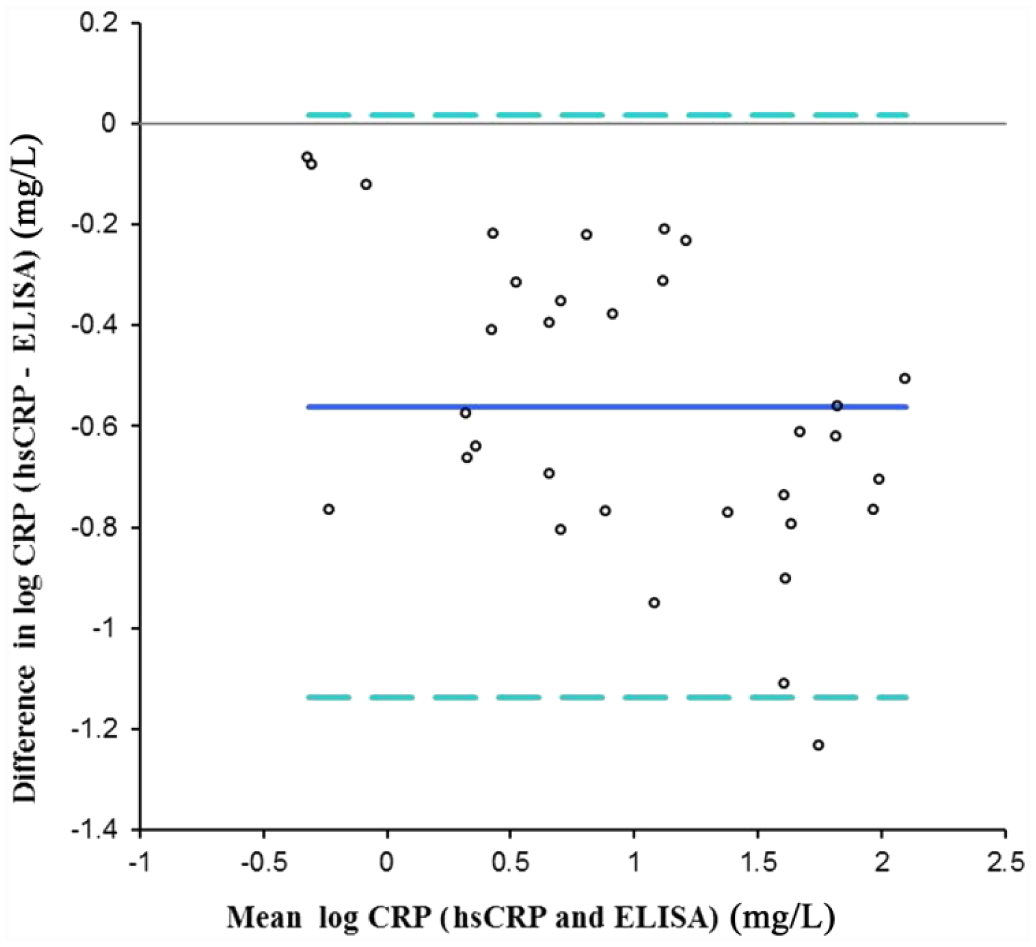
Bland–Altman difference plot with bias (solid line) and 95% limits of agreement (dashed lines) for log transformed C-reactive protein (CRP) concentrations measured with an automated immunoturbidimetric canine-specific high-sensitivity CRP assay (hsCRP) and a canine-specific enzyme-linked immunosorbent assay (ELISA; n = 35).
Clinical research studies
High-sensitivity CRP after surgery
Seven dogs of 4 different breeds were included in the study: 3 German Shepherd dogs, 2 Labrador Retrievers, 1 Airedale Terrier, and 1 Danish-Swedish Farmdog. The median age was 4 years (range: 1–7 years). The median CRP concentrations measured with the hsCRP assay was 0.83 mg/L prior to surgery (baseline). At 2, 4, 6, and 8 hr after surgery, the median CRP concentrations were 0.69 mg/L, 1.44 mg/L, 6.14 mg/L, and 13.9 mg/L, respectively. The difference in CRP concentration compared with baseline was statistically significant at 6 hr (P = 0.01) and 8 hr (P < 0.01), but not at 2 hr (P = 1.00) and 4 hr (P = 0.16). With the cCRP assay, a significant increase in CRP was detected at 8 hr (P < 0.01) but not at 2 hr (P = 1.00), 4 hr (P = 1.00), or 6 hr (P = 0.74).
High-sensitivity CRP in lean and overweight dogs
Fifteen dogs were included in the study; 6 dogs had a BCS of 5 and were allocated to the lean group, and 9 dogs had a BCS of 6–7 (median 6) and were allocated to the overweight group. Mean weight in the lean group was 34 kg, and in the overweight group 38 kg. The median (range) age was 5 (3–6) years and 5 (5–6) years in the lean and overweight group, respectively. The median (range) CRP concentration in the lean group was 0.7 (<0.5–1.4) mg/L, compared with 1.1 (0.5–6.4) mg/L in the overweight group (P = 0.06).
Discussion
In this study, an automated, canine-specific hsCRP assay was validated and applied on samples from clinical research studies. The validation indicated that the hsCRP test can be used to accurately measure low CRP concentrations in canine serum samples. The imprecision of the hsCRP assay met the requirement for optimal performance, expressed as a CV value of <6.1%,13,22 and was lower than previously reported for canine-specific hsCRP methods.21,31 The focus in the current study was on within-run imprecision, because the recommendation for using such a test in research is to analyze all samples from 1 study in a single run, to avoid interassay variation. The hsCRP assay was acceptably linear under dilution for the intended working range ≤30 mg/L, with the exception of the most diluted sample with the lowest hsCRP concentration. This sample did not meet the quality requirement in the linearity study, but yet the sample had an expected CRP concentration above the LOQ of 0.5 mg/L determined in a separate experiment. The different study designs in the linearity and LOQ experiments can explain the discrepancy. In the linearity study, the whole intended measurement range was evaluated by diluting a sample with CRP concentration of approximately 30 mg/L, whereas in the LOQ experiment, a start sample with CRP concentration of approximately 8 mg/L was diluted to expected CRP concentrations of 1 mg/L, 0.5 mg/L, and 0.25 mg/L. The concentration of the start sample represented the “true” value in this experiment, and a different LOQ may have been obtained if a start sample with another CRP concentration was chosen. This needs to be acknowledged by researchers performing studies where an exact LOQ is of importance.
The original cCRP test, on which the hsCRP test was based, was not affected by relevant prozone effect. 14 By increasing the sample volume 10 times in the hsCRP test, without changing the reagent volume, a prozone effect was expected to occur. The reason for this is that in a sample with high CRP concentration, the amount of CRP protein will be relatively much higher than the amount of CRP-binding antibodies, preventing successful formation of antigen–antibody complexes and leading to erroneous results. In our experiment, a prozone effect was illustrated by the fact that samples with CRP concentrations greater than ~150 mg/L were falsely reported to have low CRP concentrations (<30 mg/L) with the hsCRP assay. Therefore, it is crucial that only samples with low CRP concentrations are analyzed with the hsCRP assay.
The results from the interference study showed that, in the hsCRP assay, there was no statistically significant interference from hemolysis at a hemoglobin concentration of 5 g/L, which corresponds to moderate hemolysis that is easily detected by visual inspection. At higher hemoglobin concentrations (10 g/L), slight interference was present, and therefore such samples should not be analyzed with the hsCRP assay. Interference from hemolysis has previously been shown with the canine CRP ELISA used as comparative method in this study, 21 whereas no interfering effect was present with a TR-IFMA. 30 In samples that were made lipemic by adding a commercial fat emulsion to sera, no interfering effect was present at a triglyceride concentration of 10 g/L, and only a mild interfering effect was present at a triglyceride concentration of 25 g/L, which represents severe hypertriglyceridemia. The presence of lipemia in a sample will cause increased absorbance of the blank reading in the instrument compared with the absorbance of a nonlipemic sample. After the blank reading, when sample and reagent containing antibodies are mixed, the absorbance increases even further. In naturally lipemic samples analyzed with the hsCRP assay, the absorbance occasionally was so high that it exceeded the optical limit of the instrument and therefore no result was reported (data not shown). This interference did not occur in the samples to which a commercial fat emulsion was added, despite a higher triglyceride concentration in the experimental samples than in the naturally lipemic samples (data not shown). The commercial fat emulsion does not contain triglycerides of the same sizes that are most commonly present in vivo. 29 Therefore, the results from the experiment with added fat solution cannot be directly transferred to naturally lipemic samples. Another approach for testing the effect of lipemia could be to measure CRP in samples before and after ultracentrifugation, 3 and experiments using this method could be performed to further characterize the effect of natural lipemia on hsCRP measurements.
There is no gold standard method available for measuring canine CRP, and therefore it was not possible to assess true bias in the method comparison study. Instead, a comparison between the new assay and a previously validated ELISA was performed to investigate relative bias. Because the agreement between the methods was poor, the assays should not be used interchangeably. Most often, the hsCRP test measured lower CRP concentrations than the comparative test, but there was a marked variation between individual samples, and the cause of this was not determined. Compared with the ELISA, the hsCRP test had the important advantage that it was automated, which diminished the risk of manual errors and made it much less labor intensive to operate. Also, a large number of samples could be analyzed in 1 run with the hsCRP assay, thereby avoiding the interassay variation caused by the use of multiple ELISA plates.
No method comparison study between the cCRP test and the hsCRP test was performed, because of the different measurement ranges of the assays. Instead, the methods were compared when applied on clinical research samples from dogs undergoing surgery. The hypothesis, that the hsCRP test would be superior for detecting an expected increase in CRP concentrations at an early stage after OHE, was confirmed. The hsCRP assay is therefore the preferred test for monitoring CRP changes during the first postoperative hours in dogs undergoing surgery.
In people, obesity has been associated with increased concentrations of CRP,5,32 whereas studies of obese dogs have reported both increased 11 and decreased37,39 CRP concentrations. Different study designs and inclusion and exclusion criteria could explain these divergent results. One possible pitfall when investigating differences in CRP concentrations in apparently healthy dogs is that it can be difficult to exclude with certainty the presence of low-grade inflammatory diseases such as inflammatory bowel disease, rhinitis, periodontitis, and osteoarthritis, which may affect CRP concentrations.16,18,36,41 In addition, factors such as age, sex, or breed could potentially influence CRP concentrations in dogs. In people, CRP concentrations are positively correlated with increasing age,17,32 and differences between men and women have been reported. 32 No significant age or sex differences in CRP concentrations were found in a previous study of 144 healthy Beagles aged 3 months to 6 years, 23 but breed differences have been reported.25,38 In the present study, dogs of a single breed and sex were included to avoid these 2 factors as possible confounders. The hypothesis that overweight dogs had increased CRP concentrations compared with lean dogs was not statistically confirmed. The dogs in the present study were only mildly overweight and a different result may have been obtained if grossly obese dogs had also been included. Larger studies on well-characterized dogs are required to establish the association between BCS and CRP concentrations in dogs.
To facilitate additional research about conditions involving CRP within low and ultralow serum concentrations, a hsCRP assay should ideally be commercially available and easily accessible. These goals are only partially obtained with this validated hsCRP assay as neither the calibrators nor controls, as purchased from the manufacturer, are adapted for a hsCRP assay. Therefore, if these commercially available reagents are to be used for hsCRP testing on a new instrument, or if a new batch is purchased, a validation study should be performed prior to evaluation of subject samples. To date, 4 different batches have been successfully validated for hsCRP testing at the authors’ laboratory (data not shown), illustrating the assay’s suitability to the research laboratory setting.
Footnotes
Acknowledgements
The authors acknowledge Kathrin Sunde (Gentian AS) and Anne Frösegård (University Animal Hospital, SLU) for advice and laboratory assistance.
a.
Vacutainer, Becton-Dickinson, Stockholm, Sweden.
b.
SC Micro tube, Sarstedt AG & Co, Nümbrecht, Germany.
c.
Gentian cCRP, Gentian AS, Moss, Norway.
d.
Abbott Architect c4000, Abbott Park, IL.
e.
Randox Laboratories Ltd, Crumlin, United Kingdom.
f.
LifeDiagnostics, West Chester, PA.
g.
Intralipid 200 g/L, Fresenius Kabi AB, Uppsala, Sweden.
h.
Phase EIA canine CRP Assay, Tridelta Development Ltd, Maynooth, Ireland.
i.
Analyse-it Software Ltd, Leeds, United Kingdom.
j.
Minitab Inc., State College, PA.
Declaration of conflicting interests
Anna Hillström’s PhD project at the Swedish University of Agricultural Sciences (SLU) was partly financed by Gentian AS, the company manufacturing the assay investigated in this article. The research was performed independently, with collaborative parties outside the university having no influence over study design, data acquisition, analyses, results, manuscript preparation, or scientific publication.
Funding
The study was financed by Eurostars project Mammalian CRP through Vinnova project 2010-01777.