
Abstract
Several Actinobacillus spp. are common commensal bacteria of the oral cavity, gastrointestinal tract, and reproductive tract of horses and can cause disease in both foals and adults. The current retrospective study was designed to review Actinobacillus spp. isolated from clinical samples or necropsies of 99 horses during 1999–2011. The cases consisted of 43 foals (<6 months of age), 4 young adults (6 months–2 years), 39 adults (>2 years of age), 2 aborted fetuses, and 11 with unspecified ages. Clinical history, signs, bacterial species isolated, and associated lesions were documented. Actinobacillus spp. were isolated 111 times. The most common isolates were Actinobacillus equuli subsp. equuli (38.7%) and hemolytic Actinobacillus spp. (24.3%). Other isolates were Actinobacillus lignieresii (5.4%), Actinobacillus pleuropneumoniae (1.8%), and unclassified Actinobacillus spp. (28.8%). Actinobacillus equuli subsp. equuli was most commonly isolated from clinical and necropsy cases of septicemia and respiratory disease in both foals and adults. Embolic nephritis, the classical septicemic lesion of equine neonatal actinobacillosis, was also present in several adult septicemic actinobacillosis cases. Predisposing factors such as failure of passive transfer of colostral antibodies as well as concurrent pathogenic bacterial or viral infections were present in numerous actinobacillosis cases. There were many cases, however, for which a predisposing factor or concurrent infection was not documented or apparent, suggesting that Actinobacillus spp. can be primary pathogens under the right circumstances and in the right location.
Introduction
Equine actinobacillosis is caused by several Actinobacillus spp., which are Gram-negative, pleomorphic, commensal bacteria belonging to the family Pasteurellaceae.8,25 Actinobacillus equuli subsp. equuli and Actinobacillus equuli subsp. haemolyticus are most commonly isolated from equine cases with A. arthritidis, A. lignieresii, A. suis, and A. pleuropneumoniae being isolated sporadically and often from localized lesions.2,4,20,26 Actinobacillus equuli subsp. haemolyticus and A. equuli subsp. equuli differ by the presence or absence of a repeats-in-toxin (RTX) toxin referred to as the A. equuli toxin (Aqx), which is encoded by the aqx gene.7,8,14
Several authors have defined differences in the normal locations and disease patterns of the A. equuli subspecies.14,24,25 Actinobacillus equuli subsp. equuli is carried innocuously in the oral cavity and alimentary tract of adult horses and is primarily associated with septicemia of neonatal foals (sleepy foal disease).14,19,23 Neonatal septicemic actinobacillosis cases have characteristic lesions including embolic nephritis, embolic pneumonia, lymphoid necrosis, multifocal hepatic necrosis, and septic arthritis. 27 Actinobacillus equuli subsp. haemolyticus, however, prefers the respiratory tract and is isolated from the normal oral cavity and from tracheal wash fluids.14,15 Both subspecies can cause respiratory infections, septicemia, metritis, mastitis, arthritis, endocarditis, meningitis, mare reproductive loss syndrome, cellulitis, and peritonitis.1,6,10,18,30,32 Contributing factors for systemic actinobacillosis in foals include failure or partial failure of passive transfer (FPT) and unsanitary conditions in the birthing environment. 30 In adult horses, systemic actinobacillosis has traditionally been rare and is often associated with underlying disease or another predisposing factor.16,29
Because of the various clinical syndromes and pathological processes associated with infections of horses with Actinobacillus spp., a retrospective study of equine cases from which Actinobacillus spp. were isolated at the Oklahoma Animal Disease Diagnostic Laboratory (OADDL; Stillwater, Oklahoma) during 1999–2011 was undertaken to categorize those syndromes. In addition, because RTX toxins are major virulence factors in other bacteria, 12 the study sought to determine if there were differences in clinical disease and pathologic changes in horses infected with hemolytic or nonhemolytic Actinobacillus spp. Prior to the reclassification of A. equuli in 2002 into hemolytic and nonhemolytic subspecies and for an extended period afterward, hemolytic Actinobacillus spp. isolated from horses were usually identified by diagnostic bacteriologists as equine A. suis.8,14 In fact, differentiation between A. suis and A. equuli subsp. haemolyticus requires identification of the aqx gene in A. equuli or the apxI and apxII genes in A. suis.3,15 In addition, the RTX toxins expressed by the aqx, apxI, and apxII genes are responsible for host specificity of hemolytic A. equuli and A. suis, respectively.11,15 For the purposes of this retrospective study and because hemolytic Actinobacillus isolates from the past were not available for sequencing, isolates reported as A. suis and, more recently as A. equuli subsp. haemolyticus, are designated as hemolytic Actinobacillus spp.
Materials and methods
Case selection, sample submission, and data collection
Between 1999 and 2011, Actinobacillus spp. were isolated and identified by standard bacteriologic methods26,27 from 124 equine cases in the Bacteriology Laboratory of the OADDL. Specimens for bacteriologic isolation were obtained from clinical and necropsy cases, including those necropsied in the OADDL or in the field. Clinical and necropsy case information included clinical history, age of the animal, bacterial species isolated, and lesions noted at necropsy (when applicable). Clinical samples included transtracheal wash fluid, blood, abdominocentesis fluid, and swabs from the uterus, joints, nasal cavity, guttural pouch, bone, tendon sheath, and abscesses. Necropsy case information included pathological, microbiological, and toxicological information. Archived histology slides from each necropsy case were reviewed.
Of the 124 cases from which an Actinobacillus spp. was isolated, 99 were enrolled in the study. Enrollment into the study used the following criteria. First, the origins of the samples submitted from clinical and necropsy cases were clearly identified. Second, the case record was complete with respect to clinical history. Third, the site from which Actinobacillus spp. was isolated was clearly associated with the pathological findings or clinical disease description. Fourth, the Actinobacillus spp. isolated was not from rectal swabs or feces.
Identification of isolates and statistical analysis
For bacterial identification, samples were routinely streaked onto citrated sheep blood agar, MacConkey II agar, and phenylethanol agar. Cultures were incubated overnight at 37°C, and examined the next morning for beta hemolysis on blood agar and lactose fermentation on MacConkey agar. A Gram stain as well as oxidase and catalase tests were performed. A pure culture was loaded for identification and antimicrobial sensitivity testing on a commercial system, a and results were observed the following day. If needed, a Christie, Atkins, Munch-Peterson (CAMP) test using a Staphylococcus aureus streak on a blood agar plate was used. Final criteria for separation of Actinobacillus spp. were as published. 27 Isolates that could not be speciated by these methods were reported as Actinobacillus spp. Chi square analyses were performed 25 to determine if distributions of isolates differed from one another.
Results
Overview of cases and isolates
Of the 99 cases, 29 were necropsy cases, and 70 were clinical cases. Forty-three cases were foals (<6 months of age), 4 were clinical cases from young adults (6 months–2 years), 39 were adults (>2 years of age), 2 were aborted fetuses, and 11 had unspecified ages. Among foals, 23 were male, 16 were female, and 4 were unspecified gender. The foals included 24 American Quarter Horse, 6 Thoroughbred, 2 each Arabian and Appaloosa, 1 each American Saddlebred, American Paint Horse, and Palomino, 2 were mixed, and 4 were unspecified breeds. For the adults (>2 years of age), 14 were male, 19 were female, and 6 were unspecified gender. The adults included 21 American Quarter Horse, 6 Thoroughbred, 1 each Arabian and American Paint Horse, as well as 2 mixed and 8 unspecified breeds. Young adult horses were 2 each male and female with 2 American Quarter Horse, 1 Arabian, and 1 American Paint Horse breeds. Both fetuses were American Quarter Horse, and gender was not specified. Of the 11 horses of unspecified age, there were 5 American Quarter Horse, 1 American Saddlebred, and 5 unspecified breeds.
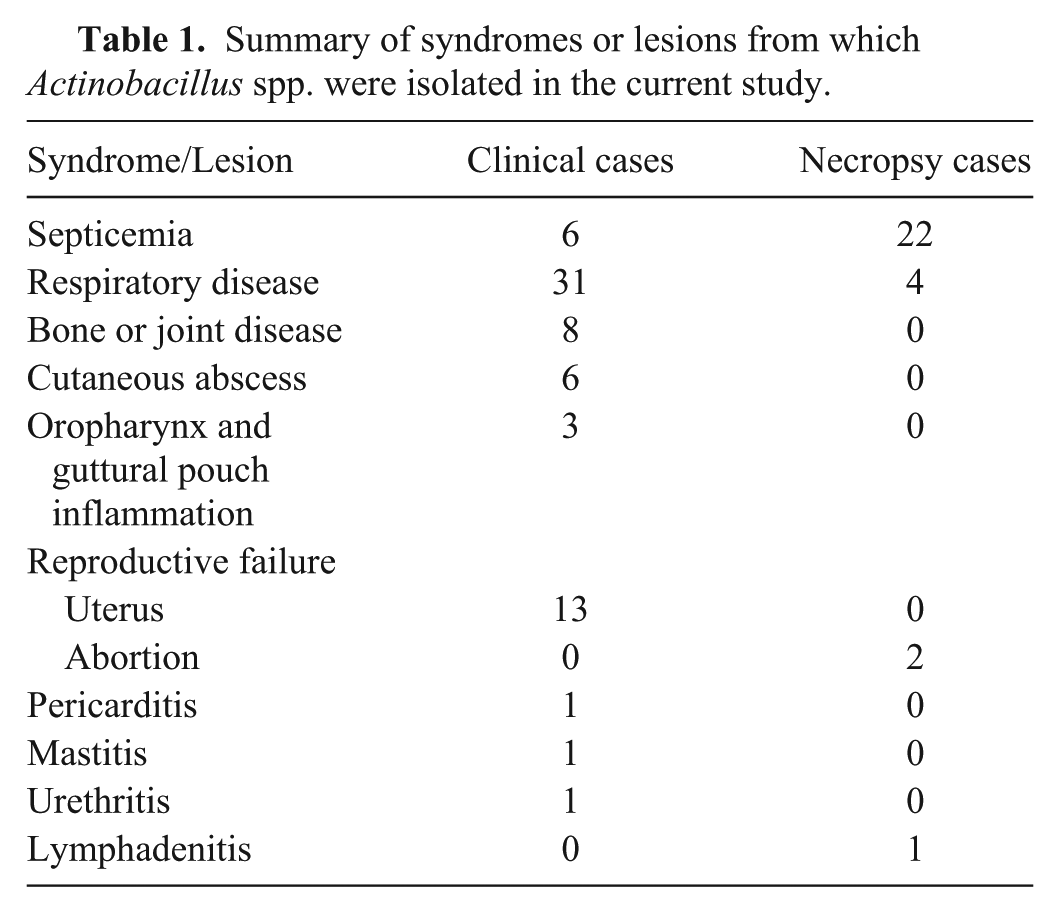
From the 99 enrolled cases, in 12 cases, more than 1 Actinobacillus spp. was recovered, primarily A. equuli subsp. equuli and hemolytic Actinobacillus spp. Of those 111 isolates from the 99 cases, 43 isolates (38.7%) were A. equuli subsp. equuli, 27 isolates (24.3%) were hemolytic Actinobacillus, 6 (5.4%) were A. lignieresii, 2 (1.8%) were A. pleuropneumoniae, and 32 (28.8%) were classified only as Actinobacillus spp. In addition, 21 of the 99 enrolled cases (21.2%) were mixed infections of 2 different Actinobacillus spp. or an Actinobacillus spp. and another potential pathogen such as Escherichia coli, Salmonella spp., Klebsiella pneumoniae, Pasteurella multocida, Streptococcus equi subsp. zooepidemicus, Clostridium spp., Equid herpesvirus 1 (EHV-1), or Influenza A virus. Syndromes and lesions from which Actinobacillus spp. were isolated are summarized in Table 1.
Summary of syndromes or lesions from which Actinobacillus spp. were isolated in the current study.
Clinical cases
Of the 70 clinical cases, 24 (34.3%) were foals (<6 months old). Thirteen presented for respiratory signs, 6 for septicemia, 2 each for synovitis and osteomyelitis, and 1 for cutaneous abscess (Table 2). Of the 24 cases, A. equuli subsp. equuli was isolated 13 times, and hemolytic Actinobacillus spp. was isolated twice. From 1 blood culture, both hemolytic Actinobacillus spp. and A. equuli subsp. equuli were isolated. From 2 transtracheal washes, A. equuli subsp. equuli was isolated with Actinobacillus spp. in both cases. In addition, 6 of the transtracheal washes yielded Actinobacillus spp. Dual infections with S. equi subsp. zooepidemicus occurred in 9 of the respiratory cases and 1 osteomyelitis case. Klebsiella pneumoniae was isolated with S. equi subsp. zooepidemicus and hemolytic Actinobacillus spp. in 1 respiratory case. In these foals, there was a significantly greater (p < 0.05) number of A. equuli subsp. equuli or other Actinobacillus spp. isolated compared to the number of hemolytic Actinobacillus spp. isolated (Fig. 1).
Isolation site of Actinobacillus spp. from 70 clinical cases over the period of 1999–2011. Ages ranged from 1 day to 19 years old.
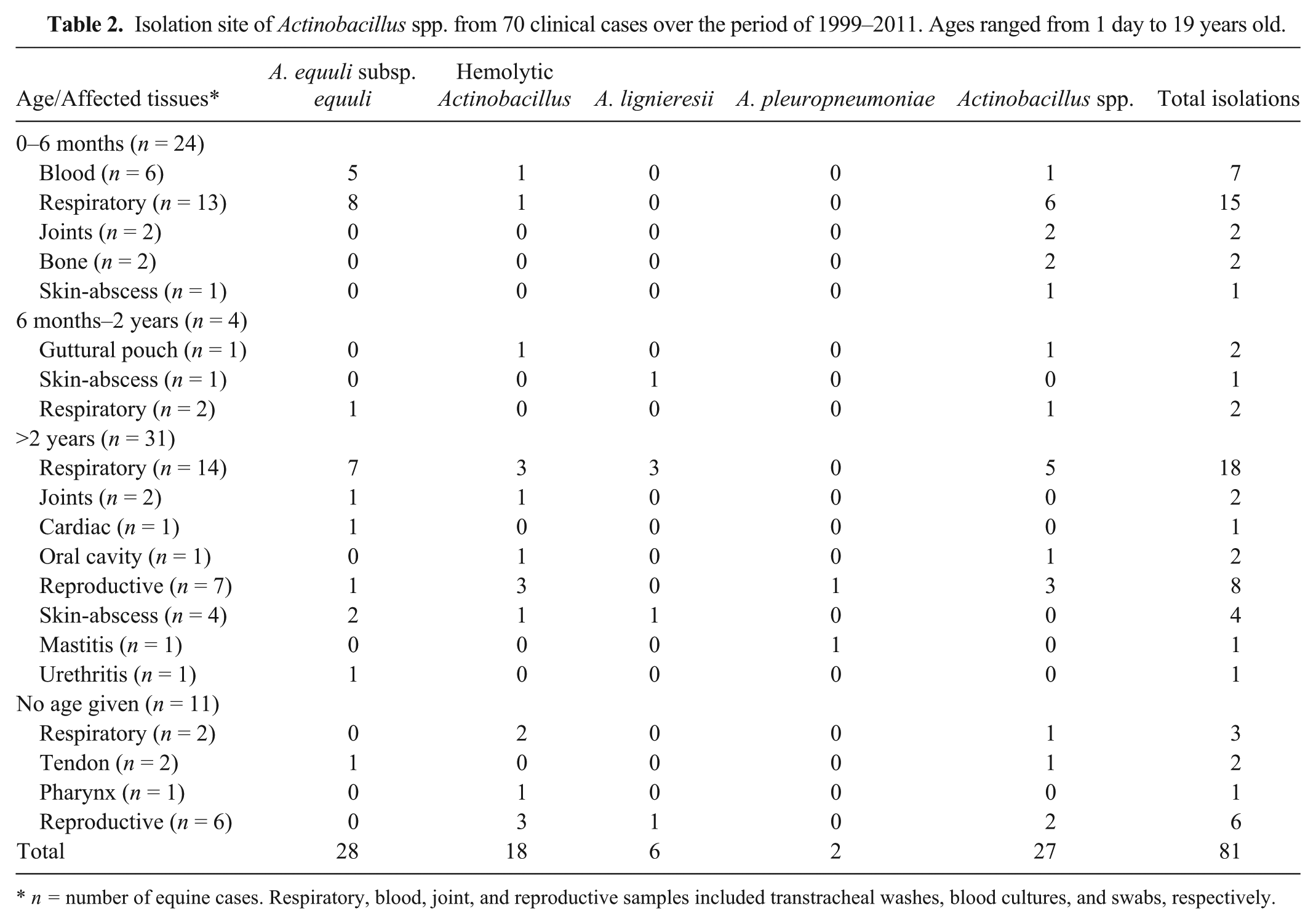
n = number of equine cases. Respiratory, blood, joint, and reproductive samples included transtracheal washes, blood cultures, and swabs, respectively.
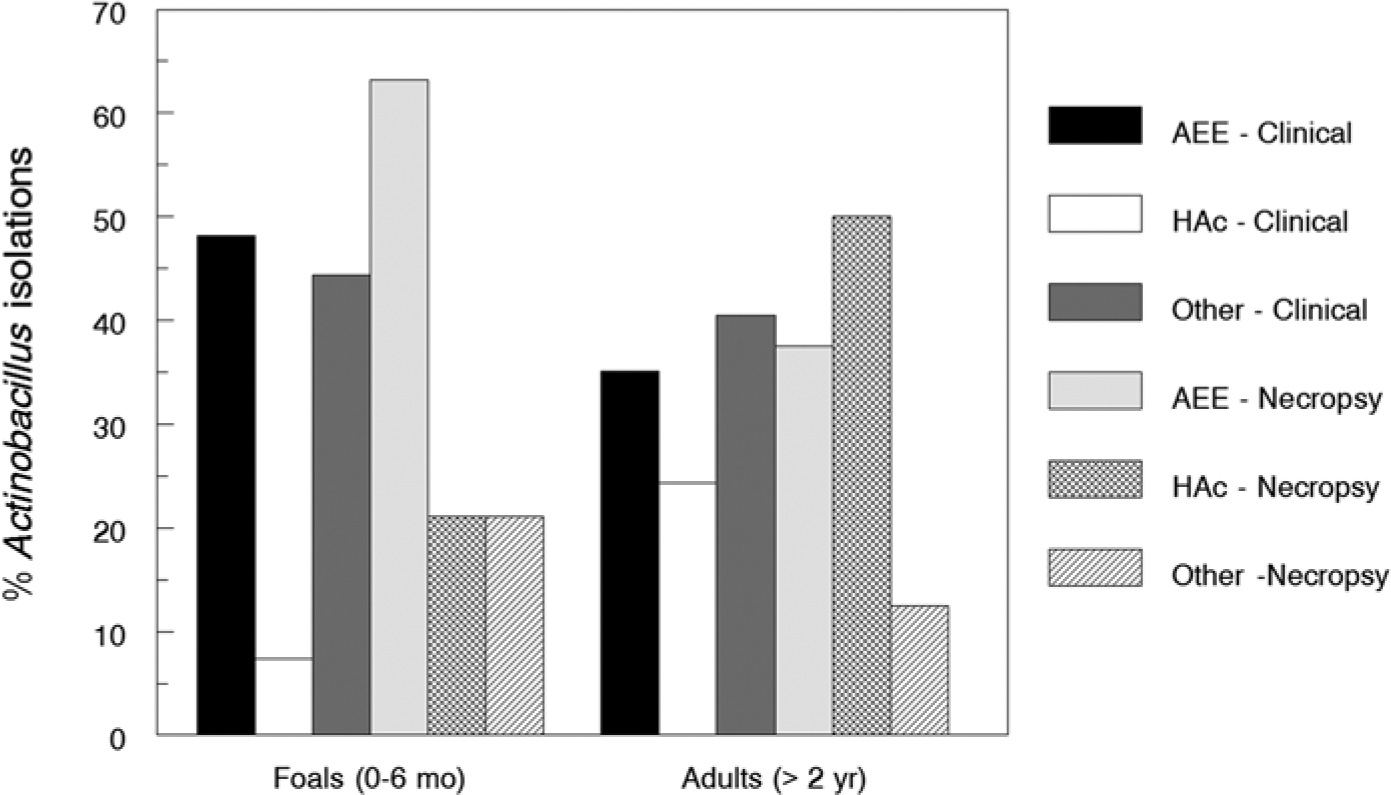
Comparison of percentages of Actinobacillus equuli subsp. equuli (AEE), hemolytic Actinobacillus spp. (HAc), and other Actinobacillus (Other) isolations from foal (0–6 months) and adult (>2 years) necropsy and clinical cases, 1999–2011. Percentage was calculated as number of AEE, HAc, or other divided by the total number of isolates for clinical or necropsy foals or adults (×100).
Four (5.7%) clinical cases were in horses 6 months to 2 years old. Two presented with respiratory signs and 1 each with guttural pouch eustachitis or cutaneous abscess. Actinobacillus equuli subsp. equuli and nonspeciated Actinobacillus spp. were isolated from the respiratory disease cases. Actinobacillus lignieresii was isolated from the cutaneous abscess, whereas both hemolytic Actinobacillus spp. and Actinobacillus spp. were isolated from the guttural pouch. Rhodococcus equi and Actinobacillus spp. were isolated from a transtracheal wash.
Thirty-one (44.3%) clinical cases were in adults (>2 years of age). Fourteen were presented for respiratory signs, 7 for reproductive failure, 4 with abscesses, 2 with synovitis, and single cases involving other locations (urethra, pericardial fluid, and teat canal). Of those clinical cases, A. equuli subsp. equuli was isolated 13 times, hemolytic Actinobacillus spp. was isolated 9 times, A. lignieresii 4 times, A. pleuropneumoniae twice, and Actinobacillus spp. 9 times. In 1 respiratory case, both A. equuli subsp. equuli and hemolytic Actinobacillus spp. were isolated from a transtracheal wash, whereas both A. equuli subsp. equuli and A. lignieresii were isolated from 2 cases of respiratory disease, a pleural aspirate and nasal swab. In addition, both A. equuli subsp. equuli and A. lignieresii were isolated from an abscess. Actinobacillus spp., hemolytic Actinobacillus spp., and A. equuli subsp. equuli were isolated from reproductive tracts. Streptococcus equi subsp. zooepidemicus occurred with Actinobacillus spp. in 3 of 6 reproductive tracts, 9 of 14 respiratory tracts, 1 of 3 abscesses, and 1 bone culture. There were no significant differences (P > 0.05) among the number of A. equuli subsp. equuli, hemolytic Actinobacillus spp., or other Actinobacillus spp. isolated from the adult cases.
Eleven (15.7%) clinical cases were in horses of unknown age. Uterine swabs were submitted from 6 cases of reproductive failure. Because of the history and procedure, it is assumed that the horses were most likely more than 2 years old. Two cases each were for respiratory signs or tendonitis, and 1 case was for pharyngitis. From those cases, A. equuli subsp. equuli was isolated once, hemolytic Actinobacillus spp. was isolated 6 times, A. lignieresii was isolated once, and Actinobacillus spp. was isolated 4 times. In 1 case, hemolytic Actinobacillus spp., Actinobacillus spp., and S. zooepidemicus subsp. equi were concurrently isolated from 1 transtracheal wash. The latter bacterium also was isolated from the pharyngeal swab and both tendonitis cases.
Necropsy cases
Two aborted fetuses were presented, and from stomach contents, hemolytic Actinobacillus spp. was isolated from one and Actinobacillus spp. from the other. Lesions were not present histologically, and in the fetus from which hemolytic Actinobacillus spp. was isolated, Streptococcus dysgalactiae subsp. equisimilis was also isolated.
For the 19 foal necropsy cases, 14 were diagnosed as primary Actinobacillus septicemia, and in 5 cases, clinical history indicated that FPT was present (Table 3). Of the 14 primary actinobacillosis septicemia cases, A. equuli subsp. equuli alone was isolated 9 times and hemolytic Actinobacillus spp. or Actinobacillus spp. were isolated from 2 cases each. In 1 septicemia case, both A. equuli subsp. equuli and hemolytic Actinobacillus spp. were isolated. In 3 additional Actinobacillus septicemia cases, concurrent infections were noted. In 1 case (case F17), the foal also had suppurative bronchopneumonia and was positive by fluorescent antibody test for EHV-1. In the other 2 septicemia cases, A. equuli subsp. equuli was isolated from multiple visceral organs concurrently with P. multocida (case F11) or concurrently with K. pneumoniae (case F7). Two foal cases were not typical neonatal septicemia. Of those cases, 1 foal (case F2) had pulmonary abscesses and meningoencephalitis with Actinobacillus spp. and S. equi subsp. zooepidemicus concurrently isolated from both sites. In the second foal (case F1), Actinobacillus spp. was the sole isolate from a mesentery lymph node associated with severe clostridial hemorrhagic enteritis. There was a significantly greater (P < 0.01) number of A. equuli subsp. equuli isolated than hemolytic Actinobacillus spp. or other Actinobacillus spp. (Fig. 1).
Microbiologic and histologic findings in 19 foals (<6 months of age) from which Actinobacillus spp. were isolated.*
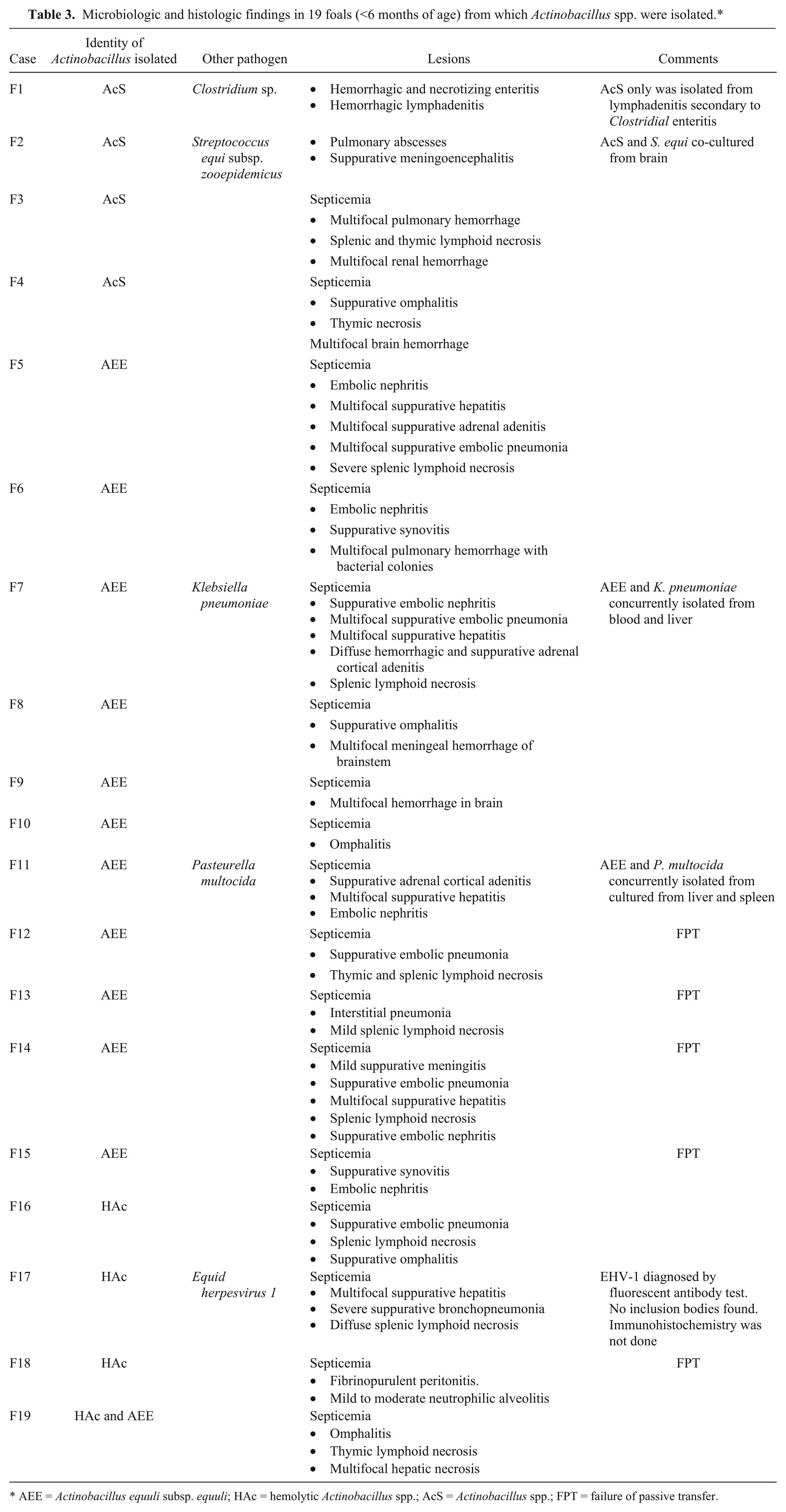
AEE = Actinobacillus equuli subsp. equuli; HAc = hemolytic Actinobacillus spp.; AcS = Actinobacillus spp.; FPT = failure of passive transfer.
For the 8 adult necropsy cases, 5 were diagnosed as septicemia cases, of which A. equuli subsp. equuli and hemolytic Actinobacillus spp. were each isolated twice, and Actinobacillus spp. was isolated once (Table 4). Three of those cases had concurrent infections. In 1 adult septicemia (case A5), E. coli was isolated with hemolytic Actinobacillus spp. from spleen and liver. In case A3, enteric salmonellosis was diagnosed with A. equuli subsp. equuli isolated from multiple visceral organs. In case A1, both Influenza A virus and EHV-1 were identified in lung samples by polymerase chain reaction; however, immunohistochemical staining was negative for the viruses in lung samples. Two cases had fibrinous peritonitis and pleuritis. From case A8, hemolytic Actinobacillus spp. was isolated from peritoneal and pleural cavities concurrently, whereas the horse also had parovarian hemangiosarcoma with serosal implants. In case A2, A. equuli subsp. equuli was isolated from lung, peritoneal cavity, and lymph nodes exhibiting fibrinous pleuropneumonia, peritonitis, and lymphadenitis, respectively. In addition, case A6 had aspiration pneumonia secondary to choke that yielded hemolytic Actinobacillus spp. and S. equi subsp. zooepidemicus. Because of the small number of adult necropsies, statistical analyses were not performed.
Microbiologic and histologic findings for 8 adult horses (>2 years old) that were necropsied and from which Actinobacillus spp. were isolated.*
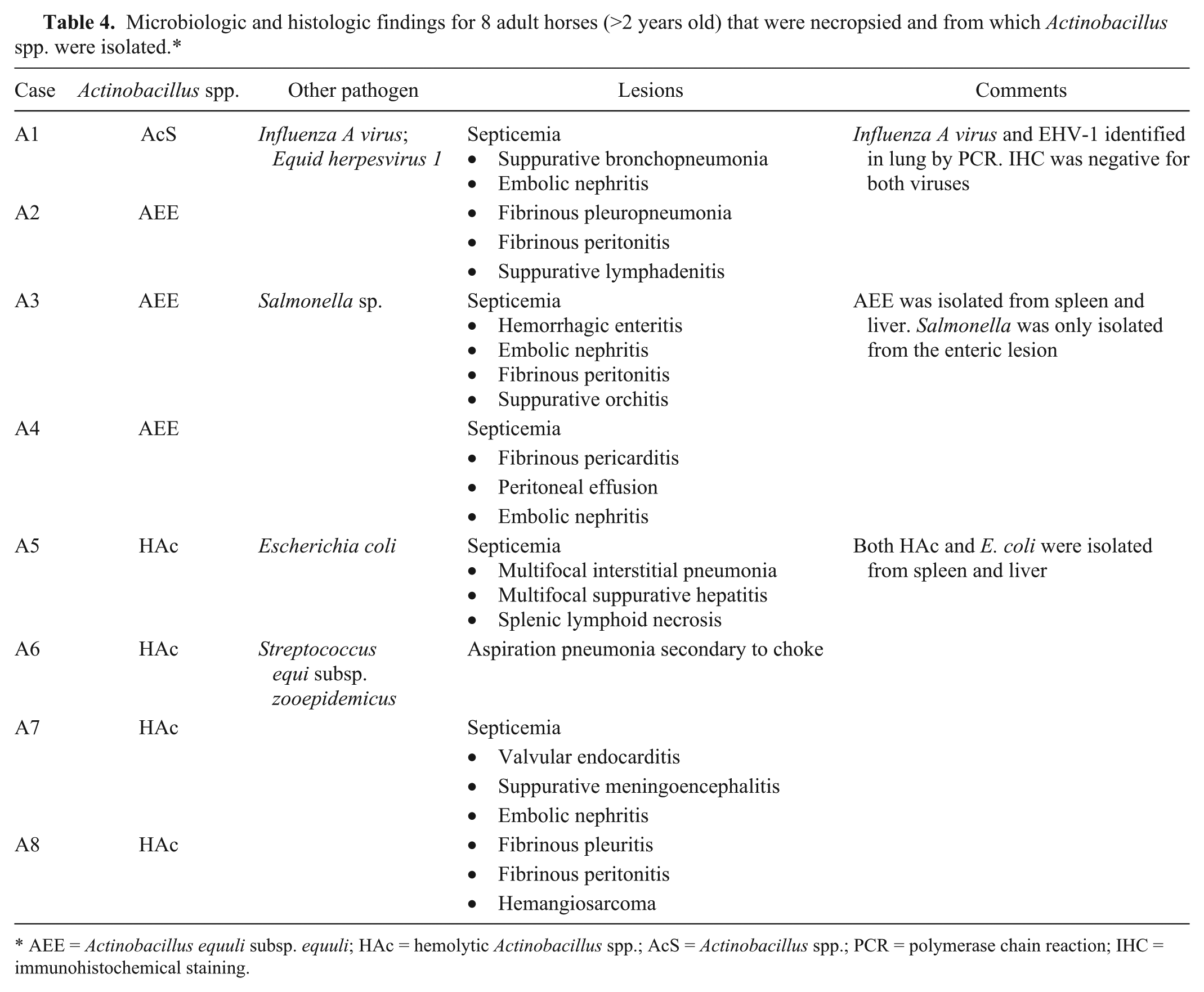
AEE = Actinobacillus equuli subsp. equuli; HAc = hemolytic Actinobacillus spp.; AcS = Actinobacillus spp.; PCR = polymerase chain reaction; IHC = immunohistochemical staining.
Pathologic changes
In cases of adult and foal septicemia, lesions varied among necropsy cases with respect to which organs were affected (Tables 3, 4). Lesions included several of the following: suppurative embolic pneumonia; lymphoid necrosis of lymph nodes, thymus, and spleen; multifocal suppurative hepatitis; suppurative embolic nephritis with microthrombi; multifocal adrenal cortical hemorrhage and/or suppurative adenitis; suppurative meningitis or meningoencephalitis; fibrinosuppurative serositis; valvular endocarditis; and suppurative omphalitis (Fig. 2). In most cases, there was necrotizing and suppurative vasculitis with perivascular hemorrhage, often containing dense bacterial thrombi. The classical equine actinobacillosis lesion of embolic nephritis with large bacterial thrombi was found in 6 out of 11 foal A. equuli subsp. equuli cases and in 1 hemolytic Actinobacillus spp. adult case that had valvular endocarditis (case A7). Adrenal adenitis was only found in cases infected with A. equuli subsp. equuli.
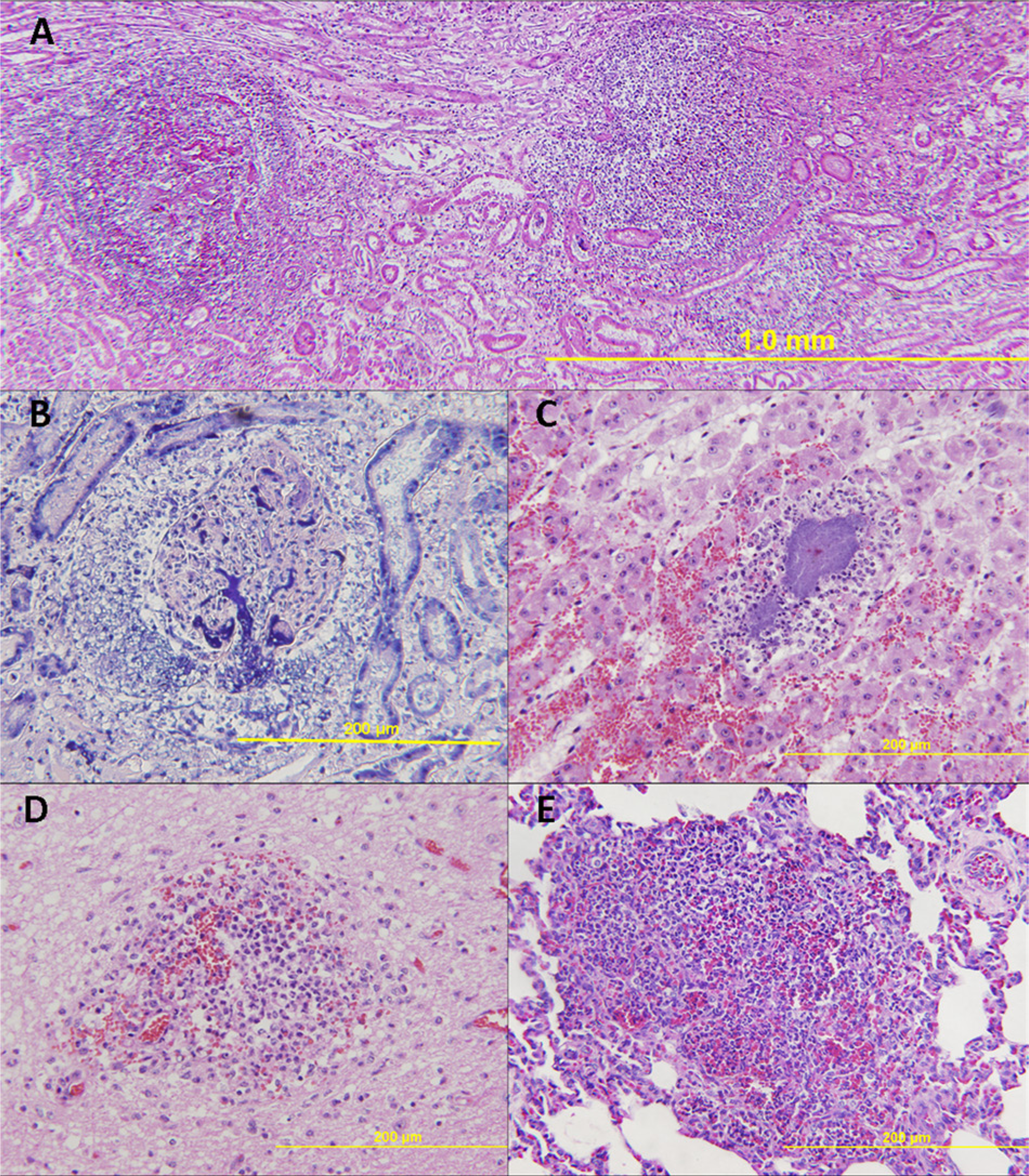
Histology of septicemic actinobacillosis.
Discussion
Actinobacillus equuli has traditionally been associated with neonatal septicemias, whereas hemolytic and other Actinobacillus spp. have been associated with peritonitis, reproductive failure, respiratory disease, or other sporadic infections in horses.9,10,17,27 In the current study, Actinobacillus spp. were associated with septicemia, meningitis, pneumonia, abortion, synovitis, osteomyelitis, tendonitis, lymphadenitis, endocarditis, guttural pouch inflammation, and cutaneous abscesses. In many cases, particularly with septicemia, Actinobacillus spp. were the primary infections. Likewise, primary infection of joints, bone, tendon, guttural pouch, and skin appeared likely, because no other bacteria or viruses were cultured, and there were no histories of other predisposing factors such as immunosuppression. In several other cases, particularly respiratory, concurrent viral and bacterial infections or predisposing lesions like choke were found, which indicate that Actinobacillus spp. were more likely secondary invaders.
In the current study, numerous cases of septicemic actinobacillosis were found in foals; however, the data indicates that A. equuli subsp. equuli and hemolytic Actinobacillus spp. (presumably A. equuli subsp. haemolyticus) can also cause septicemic actinobacillosis in adult horses with lesions similar to those associated with sleepy foal disease. Those lesions include multifocal embolic pneumonia and nephritis, with dense, intravascular bacterial colonies. 21 In foals with actinobacillosis, FPT is often associated with the disease, 30 and this was apparent in several of the cases reported in the current study. In foals F7 and F11, either K. pneumoniae or P. multocida were isolated concurrently with A. equuli subsp. equuli. In both cases, 2 separate bacteria were co-cultured from multiple sites. Therefore, whether A. equuli subsp. equuli was a primary or secondary pathogen in those cases cannot be determined.
In 1 adult and 1 foal with primary hemorrhagic enteritis, A. equuli subsp. equuli or Actinobacillus spp. were isolated from multiple sites or lymph nodes, respectively. Foal F1 had clostridial enteritis and Adult A3 had salmonellosis. Because Actinobacillus spp. are normal inhabitants of the gastrointestinal tract, loss of mucosal integrity allowed access to intestinal lymphatics and the blood stream, thus resulting in lymph node or blood colonization, as previously suggested. 17
Adult equine actinobacillosis can be associated with concurrent infectious agents or stressful events.5,21,31 In 4 of the 8 necropsied adult horses (A1, A3, A5, and A6), concurrent infections were found with enteric Salmonella spp., septicemic E. coli, Streptococcus spp., or respiratory viruses. In those cases, respiratory viruses, hemorrhagic enteritis, and aspiration pneumonia were most likely the primary events, with secondary Actinobacillus spp. infection. In case A5, the dual isolation of E. coli and hemolytic Actinobacillus spp. from the blood is highly suggestive of a concurrent enteric lesion allowing those bacteria to breach the mucosal barrier. No enteritis or intestinal lesion, however, was documented in the necropsy report for that horse. In 4 adult cases (A2, A4, A7, and A8), A. equuli subsp. equuli or hemolytic Actinobacillus spp. appear to have been the primary pathogen and responsible for septicemia, valvular endocarditis, or fibrinous polyserositis.
Actinobacillus equuli subsp. haemolyticus produces Aqx, which is an RTX toxin similar to the leukotoxins and hemolysins produced by related pathogenic bacteria such as Mannheimia haemolytica, Aggregatibacter actinomycetemcomitans, A. pleuropneumonia, A. suis, or hemolytic E. coli. 11 Many RTX toxins are host specific, and pathogenesis of those bacteria is related to RTX toxic activity. 12 The Aqx toxin is highly cytolytic to equine erythrocytes and lymphocytes and lesser so for porcine cells. 15 Most mares have serum antibodies against Aqx due to alimentary colonization, and subcutaneous injection of recombinant Aqx stimulates a strong antibody response to the toxin.13,28 Although, Aqx toxin is likely a major virulence factor in hemolytic Actinobacillus spp. infections, the higher isolation rates of A. equuli subsp. equuli over hemolytic Actinobacillus spp. from septicemia cases indicate that other virulence factors play a major role in the pathogenesis of neonatal septicemic actinobacillosis caused by A. equuli subsp. equuli. Besides Aqx, little is known about virulence factors associated with A. equuli. 17 Endotoxin, which is associated with all Gram-negative pathogens, damages endothelium, causing vasculitis and thrombosis. 22 The presence of vasculitis with bacterial emboli is characteristic of septicemic actinobacillosis and most likely indicates endotoxin damage to endothelium. 27 It is somewhat peculiar to equine actinobacillosis for large bacterial colonies to be present in affected vessels, whereas many other septicemic Gram-negative bacteria do not form such obvious intravascular colonies. 27 This observation suggests that A. equuli subsp. equuli, in particular, may express an adhesin for endothelium. In addition, there are likely other currently unknown virulence factors associated with A. equuli subsp. equuli as with other better characterized members of the genus, such as A. pleuropneumoniae; however, further investigation is needed. 25
In the current study, A. equuli subsp. equuli was isolated more frequently than hemolytic Actinobacillus spp. (presumably A. equuli subsp. haemolyticus) from the respiratory tract from both foals and adult horses with respiratory clinical signs. Therefore, the current study does not corroborate previous comments that only A. equuli subsp. haemolyticus has a propensity for the respiratory tract.14,15 That said, however, concurrent isolation of A. equuli subsp. equuli with other pathogens, especially S. equi subsp. zooepidemicus, supports the concept that in many cases, respiratory actinobacillosis is not a primary disease. In fact, in several cases, A. equuli subsp. equuli isolated from a transtracheal wash may be a contaminant from the oral cavity acquired during the sampling procedure.
Actinobacillus pleuropneumoniae and A. lignieresii, which rarely infect horses, were both isolated from multiple clinical cases. The 2 A. pleuropneumoniae cases consisted of a uterine culture from a barren mare and a bone marrow culture from osteomyelitis. Streptococcus equi subsp. zooepidemicus was concurrently isolated from both cases, and although the source of A. pleuropneumoniae infection is not known, the data suggests that it is likely a secondary infection. In 2 of the 3 clinical respiratory cases from which A. lignieresii was isolated, Streptococcus equi subsp. zooepidemicus was isolated concurrently from a transtracheal wash and from a pleural aspirate. In contrast, A. lignieresii was the sole isolate from 2 cases of cutaneous abscesses, from a single barren mare uterine culture, and from 3 transtracheal washes from adult horses with respiratory disease. Similarly, A. lignieresii infection of the skin and udder of 2 horses has been reported. 4 The current cases could indicate that A. lignieresii might be a primary equine pathogen under the appropriate conditions and in the proper location. Actinobacillus lignieresii is usually considered a normal inhabitant of the ruminant oral mucosa and a rare equine pathogen. The source of infection of horses with A. lignieresii is not known. It was shown that equine A. lignieresii isolates were a different genomospecies that cannot be phenotypically separated from the type-species ruminant A. lignieresii, and there is insufficient data to separate equine A. lignieresii into a new species. 7
Actinobacillus arthritidis was not identified in any of the cases in the present study. Actinobacillus arthritidis is considered to be an equine pathogen, being isolated from arthritis and septicemia. 25 Failure to identify any A. arthritidis isolates could indicate that it was not a pathogen in this set of cases. It is more likely, however, that several of the isolates listed only as Actinobacillus spp. in the current study were in fact A. arthritidis. Failure to identify A. arthritidis was inherent to the bacterial identification system used by the laboratory, which does not have criteria to identify A. arthritidis.
Finally, 3 hemolytic Actinobacillus spp., 1 A. lignieresii, and 2 Actinobacillus spp. were isolated from the nongravid reproductive tract of mares, and either hemolytic Actinobacillus spp. or Actinobacillus spp. were isolated from 2 cases of abortion. Streptococcus spp. were isolated from 3 of the reproductive tracts and from 1 of the aborted fetuses. Actinobacillus spp. and various streptococci have been associated with mare reproductive loss syndrome and late-term abortions. 27 Whether Actinobacillus spp. can be considered primary pathogens in equine reproductive disorders is unknown. In an acute-onset epidemic of abortions in Kentucky, A. equuli subsp. haemolyticus and A. equuli subsp. equuli accounted for 79 of 109 isolates cultured. 10 Various other Actinobacillus spp. were also isolated. In those cases, exoskeleton and attached setae from ingesting the eastern tent caterpillar (Malacosoma americanum) appear to have damaged the alimentary tract mucosa and allowed Actinobacillus spp. to breach the mucosal barrier.
In conclusion, the current study corroborates previous findings that A. equuli subsp. equuli is more commonly isolated from neonatal septicemias than is hemolytic Actinobacillus spp. and, therefore, brings into question the identifying virulence factors of A. equuli subsp. equuli. In addition, A. equuli subsp. equuli was isolated more frequently from respiratory tract infections than was hemolytic Actinobacillus spp., which is contrary to the prior concept that hemolytic Actinobacillus spp. are the more likely respiratory tract pathogen. All of this data, however, supports the notion that equine actinobacillosis is often a secondary invader or weak pathogen that requires a preexisting or predisposing event such as FPT, viral infection, concurrent bacterial infection, or neoplasia. There are numerous cases from which a predisposing event could not be determined, which indicates that certain Actinobacillus spp. can likely be primary pathogens under the right circumstances and in the right location.
Footnotes
Acknowledgements
The authors thank Ms. Teresa Blakely, Oklahoma Animal Disease Diagnostic Laboratory, for information on Actinobacillus spp. isolation protocol.
a.
TREK Diagnostic Systems Inc., Cleveland, OH.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was supported by Oklahoma State University, Department of Veterinary Pathobiology Externship Program.