
Abstract
Antibodies against Leishmania spp. are detected in most dogs with clinical signs of leishmaniasis due to Leishmania infantum. Accurate, rapid in-clinic serological tests may permit immediate confirmation of the diagnosis and implementation of therapeutic measures. The aim of the current study was to evaluate the diagnostic accuracy of 2 commercial, rapid in-clinic serological tests for the detection of anti-Leishmania antibodies in sera of dogs, the Snap Canine Leishmania Antibody Test kit (IDEXX Laboratories Inc., Westbrook, Maine) and the ImmunoRun Antibody Detection kit (Biogal Galed Labs, Kibbutz Galed, Israel), using indirect fluorescent antibody test (IFAT) as the reference method. A total of 109 sera collected from 65 seropositive and 44 seronegative dogs were used. The sensitivities of the Snap and ImmunoRun kits were 89.23% (95% confidence interval: 79.05–95.54%) and 86.15% (95% confidence interval: 75.33–93.45%), respectively, and the specificity of both tests was 100%. A good agreement between each of the rapid in-clinic serological tests and IFAT and between the 2 rapid in-clinic serological tests was witnessed. Both rapid in-clinic serological tests showed an adequate diagnostic accuracy and can be used for the fast detection of antibodies against L. infantum in dogs.
Canine leishmaniasis due to Leishmania infantum is endemic in Mediterranean countries, parts of Asia, Africa, and in Latin America. 3 Serological tests, such as indirect fluorescent antibody test (IFAT) and enzyme-linked immunosorbent assay (ELISA) are frequently used to diagnose canine leishmaniasis in everyday clinical practice.6,7,15 The variable and nonspecific clinical manifestations of the disease5,14,24 and the presence of clinically normal but seropositive dogs, underlines the usefulness of serology, not only to confirm the diagnosis of canine leishmaniasis, but also to identify a proportion of asymptomatically infected dogs that are capable of transmitting the parasite to the sandfly vectors.4,18
Rapid in-clinic serological tests may contribute in the immediate diagnosis of canine leishmaniasis and faster implementation of therapeutic measures, compared with the more time-consuming IFAT, ELISA, and the other serological tests that are performed in specialized diagnostic laboratories. 20 An immunochromatographic, rapid in-clinic serological test (Snap Canine Leishmania Antibody Test kit; hereafter Snap kit) a using L. infantum promastigote antigen that is prepared by sonic disruption, filtration, and diethylaminoethyl column purification, has commercially available for many years and is considered of adequate diagnostic accuracy.10,16 The ImmunoRun Antibody Detection kit b (hereafter, ImmunoRun kit) is a chromatographic, rapid in-clinic test for qualitative detection of anti–L. infantum antibodies in whole blood, serum, or plasma of dogs, and uses gold-conjugated L. infantum antigen. The IFAT is considered the reference method to be used for the evaluation of the diagnostic accuracy of all other serological tests, according to the guidelines of the World Organization for Animal Health. 26 The aim of the current study was to evaluate the diagnostic accuracy of the Snap and of ImmunoRun kits for the detection of anti-Leishmania antibodies in sera of dogs, using IFAT as the reference method.
Serum samples from dogs from an endemic area that had been admitted to the authors’ clinic and had been previously tested by IFAT for anti-Leishmania antibodies were used. These sera had been stored at −20°C until used for the purposes of this study. Because differences among tests are more likely to exist in serum samples with lower IFAT titers (i.e., from 1:50 to 1:400), sera selection was not random but more samples with such IFAT titers were selected for testing. Of the 109 serum samples used in the current study, 44 (40.4%) were IFAT negative and 65 (59.6%) were IFAT positive. The endpoint IFAT titers of the positive samples were 1:50 (13/65, 20%), 1:100 (8/65, 12.3%), 1:200 (12/65, 18.5%), 1:400 (14/65, 21.5%) and ≥1/800 (18/65, 27.7%).
For each serum sample the 2 rapid in-clinic serological tests were performed simultaneously, whereas IFAT was repeated on the same working day. The examiner was blinded to the results of the 2 rapid in-clinic serological tests and of the initial IFAT titer.
The Snap and ImmunoRun kits were performed according to their manufacturers’ instructions, and the results were recorded as positive, negative, or invalid. For IFAT, commercially available slides and conjugate c were used, and serum samples were tested at 2-fold dilutions in phosphate buffered saline, starting from 1:50, until reaching the endpoint titer. For statistical analysis, the results of IFAT were classified as positive (endpoint titer ≥1:50) or negative.
The results of the 2 rapid in-clinic serological tests were cross-tabulated against the respective IFAT titers. The sensitivity and negative likelihood ratio (NLR) of the 2 rapid in-clinic serological tests were calculated using commercial software d using IFAT as the reference method. The agreement (k) between each rapid in-clinic serological test and IFAT and between the 2 in-clinic serological tests was calculated using commercial software. e A k value of 1 indicates perfect agreement, whereas a k value of 0 indicates that the agreement is equivalent to chance agreement, as previously suggested.2,11 The interpretation of both rapid in-clinic serological test results was straightforward and the results were readily classified as negative or positive, with no invalid results.
The sensitivities of the Snap and ImmunoRun kits compared with IFAT were 89.23% (95% confidence interval [CI]: 79.05–95.54%) and 86.15% (95% CI: 75.33–93.45%), respectively, whereas the specificity of both rapid in-clinic serological tests was 100% (95% CI: 94.6–100%). The NLR was 0.11 (95% CI: 0.05–0.22) for Snap kit and 0.14 (95% CI: 0.08–0.25) for ImmunoRun kit. Agreement between each rapid in-clinic serological test and IFAT and between the 2 rapid in-clinic serological tests was good with all k values being >0.8 (Table 1). All 18 serum samples with an IFAT titer ≥1:800 were positive by both rapid in-clinic serological tests, whereas the sensitivity of the latter ranged from 61.54% to 100% for serum samples with IFAT titers between 1:50 and 1:400 (Tables 2, 3).
Agreement among indirect fluorescent antibody test (IFAT), Snap Canine Leishmania Antibody Test kit (Snap kit), and ImmunoRun Antibody Detection kit (ImmunoRun kit) for the detection of antibodies against Leishmania spp. in canine sera.*
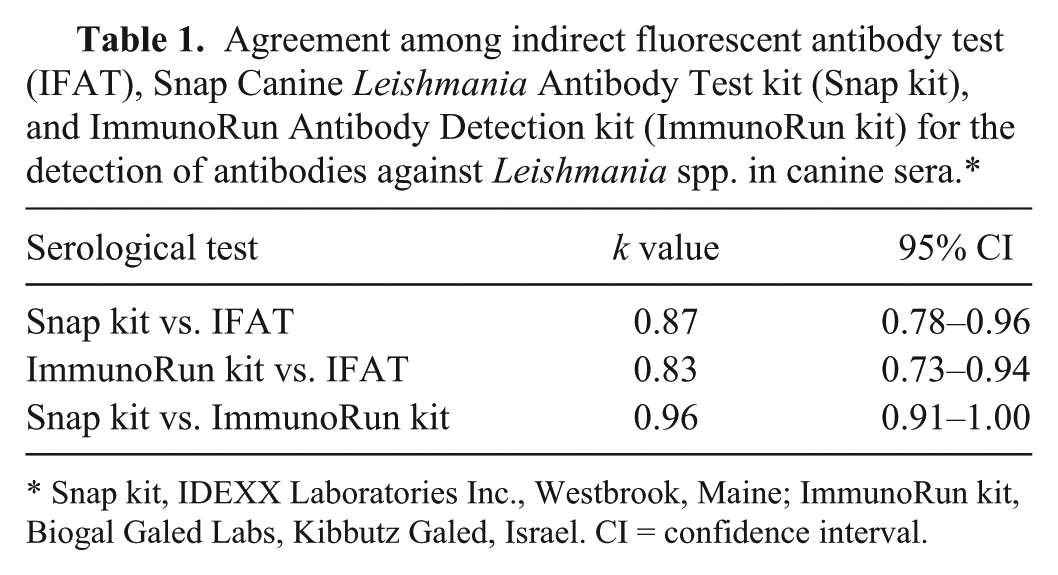
Snap kit, IDEXX Laboratories Inc., Westbrook, Maine; ImmunoRun kit, Biogal Galed Labs, Kibbutz Galed, Israel. CI = confidence interval.
Sensitivity and negative likelihood ratio (NLR) of Snap Canine Leishmania Antibody Test kit compared to indirect fluorescent antibody test (IFAT) for canine serum samples with IFAT titers against Leishmania spp. ranging between 1:50 and 1:800.*
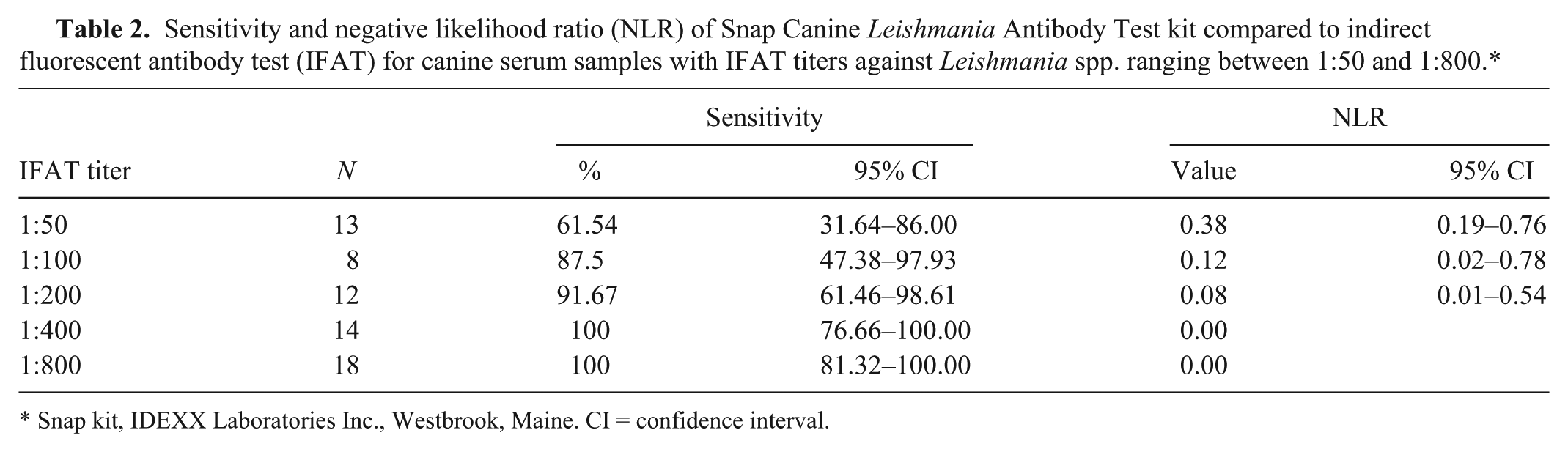
Snap kit, IDEXX Laboratories Inc., Westbrook, Maine. CI = confidence interval.
Sensitivity and negative likelihood ratio (NLR) of ImmunoRun Antibody Detection kit compared to indirect fluorescent antibody test (IFAT) for canine serum samples with IFAT titers against Leishmania spp. ranging between 1:50 and 1:800.*
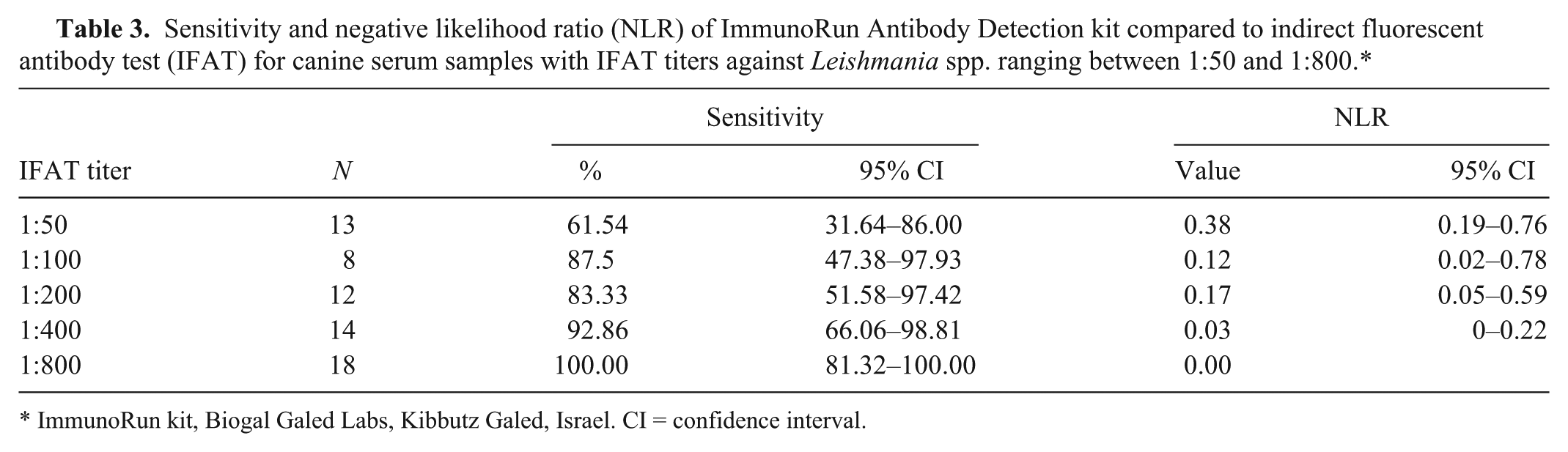
ImmunoRun kit, Biogal Galed Labs, Kibbutz Galed, Israel. CI = confidence interval.
Serology for the detection of immunoglobulin G (IgG) antibodies against Leishmania spp. is commonly employed in clinical practice in order to confirm the diagnosis of canine leishmaniasis in dogs with compatible clinical signs and/or laboratory abnormalities, to exclude the diagnosis in dogs with other diseases that mimic canine leishmaniasis, and to identify seropositive asymptomatic dogs that may develop canine leishmaniasis in the future and/or may transmit L. infantum to the sandfly vectors.4,13,17,24 Quantitative serological tests, like IFAT, are usually advocated because they permit the classification of positive results into the questionable, low-, medium-, and high-positive range, which is necessary for clinical staging and for therapeutic decisions.19,21,25 On the contrary, rapid in-clinic serological tests, like the Snap and ImmunoRun kits, provide only qualitative information; thus a positive test result should always be followed by quantitative serology and this is associated with an increased overall cost of the diagnostic investigation. On the other hand, the commercial availability, convenience, and immediacy of the results make such tests attractive for practitioners. 20 If rapid in-clinic serological tests prove to be accurate, they can offer several additional advantages, including the immediate implementation of therapeutic measures that do not depend on the clinical stage of canine leishmaniasis (e.g., allopurinol administration, use of insect repellents) when the result is positive or guiding diagnostic investigation toward other differential diagnoses when the result is negative.
Under our test conditions, all 18 serum samples with IFAT titers ≥1:800 were tested positive by both rapid in-clinic serological tests. In addition, all 44 IFAT-negative serum samples were tested negative by both rapid in-clinic serological tests and discrepant results were only witnessed in serum samples with IFAT titers that may be classified as questionable, low-positive, and medium-positive. 25
In the current study, the overall sensitivity and specificity of the 2 rapid in-clinic serological tests were calculated, considering all serum samples with detectable anti-Leishmania antibodies, even at the lowest dilution tested (1:50), as positive. This decision was based on the cutoff titer that is currently proposed by the manufacturer of the slides and the conjugate we used. However, our results should be interpreted keeping in mind that there is no perfect IFAT cutoff titer, its selection is, inevitably, a compromise in an effort to achieve the best possible combination of sensitivity and specificity, and variable cutoffs ranging from 1:40 to 1:200 are adopted in different geographical areas and in different diagnostic laboratories.1,22 If a different cutoff titer had been used, the results would not have been the same. For example, the sensitivity and the specificity of the Snap kit would had been 97.73% and 76.92%, respectively, if a 1:200 IFAT cutoff titer had been adopted and the relevant figures for the ImmunoRun kit would had been 93.18% and 76.92%, respectively (data not shown).
It is also important to emphasize the influence of the way that serum samples were selected on the sensitivity and specificity of the 2 rapid in-clinic serological tests. It is well known that the specificity of serology for L. infantum may be impaired due to cross-reactions with other organisms.8,16 In Mediterranean countries, like Greece, where Trypanosoma spp. infections do not occur and canine infections by other Leishmania species besides L. infantum are seemingly rare, false-positive results due to cross-reactions are not expected to occur frequently, independently of the serological test employed. 9 In addition, the serum samples that were tested in this study were not randomly selected and the distribution of the IFAT titers cannot be considered representative of the distribution that a diagnostic laboratory would normally encounter. Nevertheless, the calculated sensitivity (89.2%) and specificity (100%) of the Snap kit are quite close to the reported sensitivities (91.1%, 93.4%, and 94.7%) and specificities (99.2%, 98.4%, and 90.6%) of the same test using IFAT, Western blot, and ELISA as the gold standard, respectively.10,16 Similarly, a good agreement between this rapid in-clinic serological test and IFAT, Western blot, and ELISA has been previously shown.10,16 To the best of our knowledge no similar published information exists for the ImmunoRun kit.
Besides sensitivity and specificity, positive and negative predictive values are commonly used for the evaluation of the performance of various diagnostic tests. Predictive values are not reported herein because they depend, not only on the diagnostic accuracy (sensitivity and specificity), but also on the prevalence of the disease (in this case, on the prevalence of IFAT-based seropositivity) in the sample 23 ; the way serum samples were selected for the present study precludes any meaningful conclusion from positive and negative predictive values. Instead NLR, a measure of the degree that a negative test result decreases the possibility of the condition (in this case, of IFAT-based seropositivity) was calculated (Tables 2, 3). In general, NLR values >0.5 indicate poor performance of a diagnostic test and values <0.1 indicate good performance. 23 Apart for being independent of disease prevalence, likelihood ratios do not vary among different populations or settings. The interpretation of NLR is intuitive: the lower the value, the lesser the likelihood of the condition (in this case, of IFAT-based seropositivity) if the test result is negative; therefore this information can be used directly at the individual patient level. 12 In the current study, both rapid in-clinic serological tests almost reach the above set point of good performance. Finally, positive likelihood ratio could not be calculated because the 100% specificity of both rapid in-clinic serological tests results in the denominator of the equation being zero.
The 2 rapid in-clinic serological tests had an almost perfect agreement (k = 0.96); indeed, the only difference between them was witnessed in 2 serum samples with 1:200 and 1:400 IFAT titer, respectively, that were positive by Snap kit but negative by ImmunoRun kit. The possibility of handling or interpretation error was excluded because repeated testing of these samples gave identical results. Therefore, the reason for this discrepancy remains unknown and may be attributed to inherent differences of these 2 rapid in-clinic serological tests.
In conclusion, the Snap and ImmunoRun kits can be used, almost interchangeably, for the detection of anti-Leishmania IgG antibodies in canine serum samples and they are characterized by adequate sensitivity (86–89%) and specificity (100%) and by a good agreement with IFAT. However, negative results may be expected in seropositive dogs with IFAT titers between 1:50 and 1:400. Therefore, a positive test result almost certainly indicates the presence of anti-Leishmania antibodies and should be followed by quantitative serology. On the contrary, negative results do not preclude the possibility of anti-Leishmania IgG antibody presence in the serum sample.
Footnotes
a.
IDEXX Laboratories Inc., Westbrook, ME.
b.
Biogal Galed Labs, Kibbutz Galed, Israel.
c.
Fluoleish, Biovetotest Diagnostic Veterinaire, France.
d.
Calc v. 12.3.0.0, MedCalc Software, Ostend, Belgium.
e.
Graph Pad Prism v. 6, Graph Pad Inc., San Diego, CA.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors acknowledge the kind offer of the ImmunoRun kits by the manufacturer but it should be mentioned that the manufacturer was not involved in any stage of the study including study design, interpretation of results, and writing of the manuscript.