
Abstract
Fifteen cases of Francisella tularensis infection (tularemia) were identified in western gray (Sciurus griseus) and eastern gray (Sciurus carolinensis) squirrels submitted to the Washington Animal Disease Diagnostic Laboratory between 2008 and 2011. All of the squirrels originated in Washington State, a geographical area with endemic tularemia in wildlife. Nine of the 15 squirrels with F. tularensis infection had gross (2/15) or microscopic (9/15) multifocal necrotizing lesions in the spleen, liver, or lymph nodes, typical of tularemia. Special stains did not reliably identify intralesional bacteria microscopically. Six of the 15 squirrels infected with F. tularensis lacked gross and microscopic lesions typical of tularemia. All 15 squirrels with F. tularensis infection were identified by polymerase chain reaction tests on the spleen, liver, or lymph node (including all 6 squirrels without typical tularemia lesions); 8 out of 9 squirrels were positive by direct fluorescent antibody test of tissues, and 5 out of 15 squirrels were positive by culture of tissues. The findings underscore the importance of considering tularemia as a possible cause of death when no lesions of tularemia can be identified at necropsy. Furthermore, the findings suggest the possibility of subclinical infections in gray squirrels, and the importance of molecular diagnostics for definitive diagnosis of F. tularensis infection in wild squirrels.
Francisella tularensis is the causative agent of tularemia, an important bacterial disease with zoonotic potential. This highly pathogenic, Gram-negative, 0.1–3 µm, pleomorphic obligate aerobic coccobacillus requires only 10–50 colony forming units (CFU) for an infectious dose in immunocompetent human beings. The bacteria can be transmitted by aerosolization, ectoparasite vectors, ingestion, and direct inoculation into cutaneous or mucocutaneous wounds. 4 The bacterium is considered a List A select agent by the Centers for Disease Control and Prevention (CDC) with potential for use as a biological weapon (http://www.cdc.gov/Tularemia/). Francisella tularensis is divided into subspecies including the highly pathogenic F. tularensis biovar tularensis (Jellison type A) and F. tularensis biovar holarctica (Jellison type B; formerly palaearctica). 12
Commonly infected mammals include cottontail rabbits, ground squirrels, muskrats, and beavers, 13 although disease has also been reported in other mammals including domestic and wild sheep, felids and, less commonly, canids.4,5 Clinical or subclinical infection can occur in voles, mice, snowshoe hares,2,4 stone martens, 11 and possibly prairie dogs. 8 Bacterial persistence within mammalian macrophages and amoebae is reported. 7 Tularemia is present throughout the Northern Hemisphere including all of the United States except Hawaii. Disease in human beings in the contiguous United States is most commonly reported in the south central region, the Pacific Northwest, and the northeast, particularly in Massachusetts (http://www.cdc.gov/Tularemia/). Humans at increased risk for infection include veterinarians, trappers, and hunters, though disease has occurred in human beings handling infected pets such as a ground squirrel. 9
A presumptive diagnosis of tularemia in veterinary cases is most often suspected from appropriate signalment and clinical history obtained from a species of animal known to harbor endemic F. tularensis. The suspicion of tularemia is magnified by postmortem identification of gross and/or microscopic lesions associated with fulminant septicemia, including multifocal necrotizing or suppurative hepatitis, splenitis, and lymphadenitis, and in some species inflammation is granulomatous. 4 The high pathogenicity of F. tularensis and the high risk of transmission by aerosolization warrant handling suspect tissues (both as submissions and at necropsy) under enhanced biosafety level 2 or 3 procedures using a class II biosecurity cabinet or appropriate respiratory personal protective equipment. 1
The diagnostic and biosecurity plan for tularemia-suspect animals is most effective in cases of the septicemic form of the disease in a classic species from an endemic region. However, the classical form of disease is not always evident. For example, F. tularensis infection in a stone marten without expected lesions was detected by chance during an environmental screening study in Switzerland. 11 In order to provide an additional larger study of potential subclinical F. tularensis infection in a known host species, the current study has reviewed the findings from 29 western gray (Sciurus griseus) and eastern gray (Sciurus carolinensis) tree squirrels submitted from the Fort Lewis area in Washington State to the Washington Animal Disease Diagnostic Laboratory (WADDL; Pullman, Washington) from 2008 through 2011.
The squirrels examined were part of an ecology study conducted by the Washington Department of Fish and Wildlife (K. Mansfield; Spokane Valley, Washington) and were monitored by radio collars equipped with motion sensors allowing for detection of mortalities. Carcasses were recovered and submitted chilled or frozen for necropsy. Necropsies were performed on sample arrival unless thawing the carcass was necessary. Samples were fixed in 10% neutral buffered formalin, processed, and paraffin embedded for routine histology. Based on signalment, host species, and previous diagnosis of tularemia from the geographical area, necropsies were performed in a class II type A2 biological safety hood. Tissues collected at necropsy (fresh or fixed) were examined by histology, polymerase chain reaction (PCR), aerobic culture using select media, or direct fluorescent antibody test (FAT) for F. tularensis per the CDC Laboratory Response Network (CDC-LRN) for bioterrorism algorithm for F. tularensis identification (http://www.bt.cdc.gov/lrn/). Either fresh or paraffin-embedded tissues (liver and spleen) were first screened by PCR at WADDL for initial diagnosis, followed by confirmatory testing by PCR, culture, and/or FAT at a CDC reference laboratory. Gross and histological evaluations were performed by individual board-certified veterinary anatomic pathologists then reviewed in total by a single board-certified veterinary anatomic pathologist.
To identify the agent, DNA was extracted from fixed tissue blocks (liver and spleen) or fresh pooled samples of liver, kidney, and spleen using a commercial kita,3 and tested by 3 separate real-time PCR assays for F. tularensis using reagents and protocols from the CDC-LRN.6,10 Amplicons from the PCR assay were visualized on 1.5% agarose gels containing ethidium bromide. All samples were considered positive if they yielded amplicons of the correct sizes for the provided F. tularensis primer sets. Specificity was confirmed by sequencing the PCR amplicons and sequence analysis as previously described. 3
Diagnostic results from the gray squirrels infected with F. tularensis from the Fort Lewis area are summarized in Table 1. Fifteen of the 29 squirrels were positive by standard PCR for F. tularensis. The F. tularensis–specific target sequences obtained from all animals had 100% sequence identity to F. tularensis subsp. holarctica (GenBank accession no. BK006741) consistent with biotype B. Nine of the 15 PCR-positive squirrels were tested by FAT of tissues, and 8 were positive. Five of the 15 PCR-positive squirrels were also confirmed positive by aerobic culture with FAT-positive colonies at the regional reference laboratory, and 3 of the 15 had suspect aerobic isolates (morphology consistent with F. tularensis on chocolate agar plates) at WADDL. The culture-positive squirrels were identified as biotype B (consistent with the PCR results). Thirteen of the 15 positive squirrels lacked gross lesions of tularemia, and 6 also lacked typical histological lesions. Nine squirrels had necrotizing to suppurative hepatitis and splenitis. Other accompanying histological lesions included necrotizing to suppurative lymphadenitis (2 animals), suppurative orchitis (1 animal), and suppurative choroid plexitis (1 animal). Histological lesions were present in 6 of the 8 FAT-positive animals. Intralesional bacteria were often not observed histologically. Tularemia was deemed the immediate or proximate cause of death in 9 of the 15 F. tularensis–infected squirrels based on the lesions of septicemia (multifocal necrosis in multiple viscera).
Summary of pathology and microbiology findings from 15 adult western gray (Sciurus griseus) and eastern gray (Sciurus carolinensis) squirrels with Francisella tularensis infection identified at the Washington Animal Disease Diagnostic Laboratory between 2008 and 2011.*
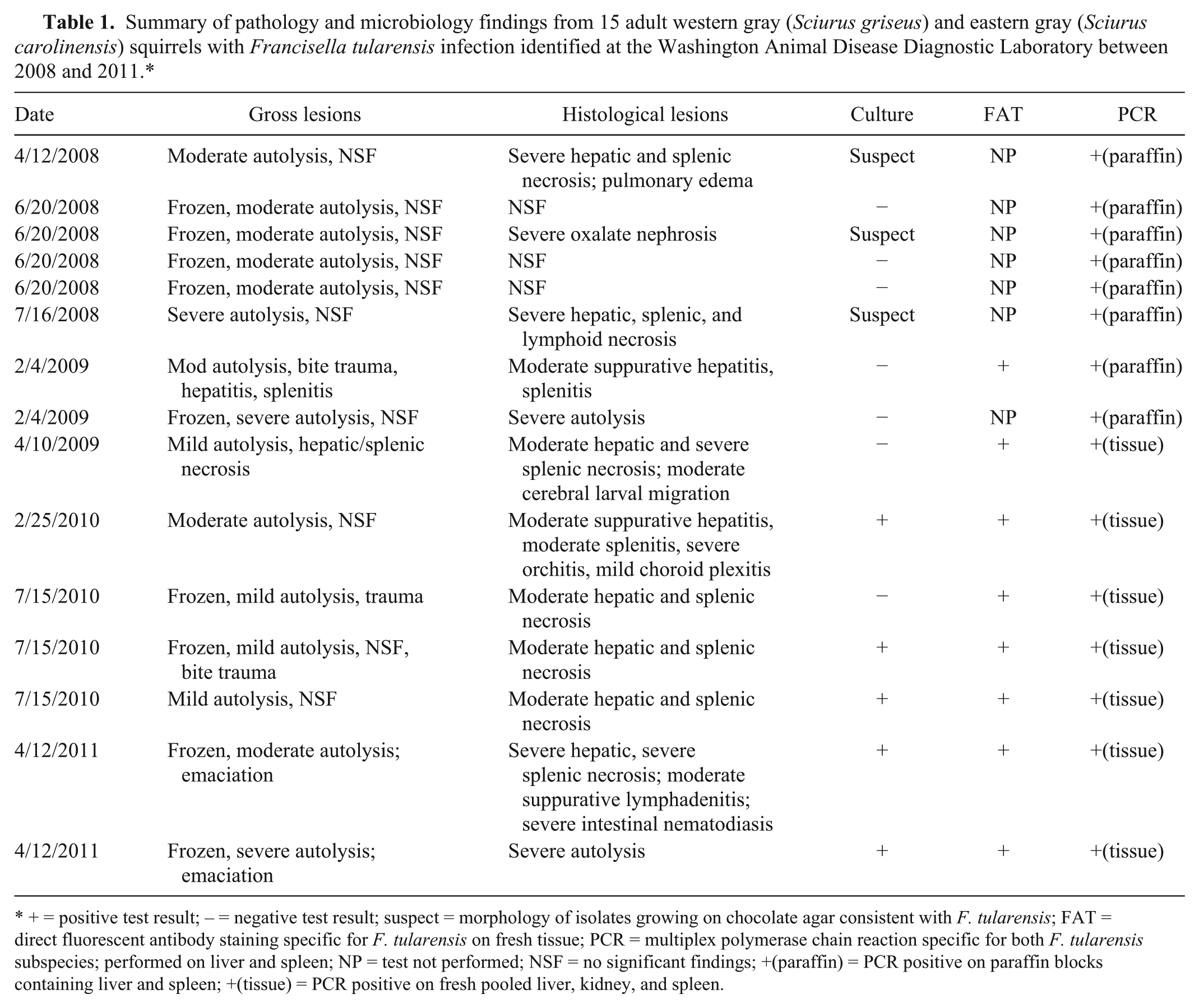
+ = positive test result; – = negative test result; suspect = morphology of isolates growing on chocolate agar consistent with F. tularensis; FAT = direct fluorescent antibody staining specific for F. tularensis on fresh tissue; PCR = multiplex polymerase chain reaction specific for both F. tularensis subspecies; performed on liver and spleen; NP = test not performed; NSF = no significant findings; +(paraffin) = PCR positive on paraffin blocks containing liver and spleen; +(tissue) = PCR positive on fresh pooled liver, kidney, and spleen.
The findings of the current study highlight the difficulty of diagnosing F. tularensis infection by gross or microscopic lesions alone as 40% of the squirrels in the study were identified with F. tularensis infection but lacked any pathological changes typical of tularemia. Identification of suspect cases can be complicated by the degree of autolysis and freeze–thaw artifact, and these conditions are particularly common with wildlife submissions. In addition to the septicemic form of disease, pneumonic, ocular, oropharyngeal, and glandular (lymphoid) forms of disease are also reported in human beings, 4 and the veterinary diagnostician at necropsy may not consider similar presentations in animals. Alternatively, the 6 squirrels lacking gross or histological lesions of tularemia could represent subclinical infections, which in voles can occur with or without lesions.2,4 Subclinical infection could be more likely with F. tularensis subsp. holarctica because this subspecies is known to be less pathogenic in rabbits and human beings than F. tularensis subsp. tularensis.4,13 There appear to be no reports correlating subclinical infection with bacterial loads and infectivity, and the significance of subclinical infection with regard to potential zoonosis is not known. However, subclinically infected voles shed the bacteria in urine, providing a potential source for environmental accumulation and disease transmission.2,4 Further studies are necessary in order to identify subclinical infection in live western and eastern gray tree squirrels, the frequency of subclinical infection in endemic regions, and the routes of bacterial shedding and transmission.
Of the 9 squirrels with lesions of clinical F. tularensis infection, all 9 were identified by PCR, while only 5 were definitively confirmed by culture. Of the remaining 4 animals, 3 were suspect culture positive, and the last remained culture negative. Though culture has traditionally been considered the gold standard, the current report suggests that testing by multiplex PCR is a more sensitive assay for identifying F. tularensis–infected animals.
Altogether, the findings of the current study demonstrate the challenges posed with the diagnosis of F. tularensis infection in animals, especially wildlife submitted to diagnostic laboratories in less than optimal postmortem condition. In those cases lacking signalment and lesions typical of tularemia, appropriate microbiological tests might not be pursued, resulting in the underdiagnosis of F. tularensis infection. Furthermore, the finding of F. tularensis in wild gray squirrels without typical tularemia lesions highlights the awareness to use appropriate biosafety measures at necropsy in all squirrels from regions with endemic F. tularensis in wildlife.
Footnotes
Acknowledgements
The authors thank the participating wildlife biologists, diagnostic pathologists, microbiologists, and technicians, including Dr. John Young from the CDC in Fort Collins, Colorado, who assisted with the diagnoses in these cases.
a.
DNeasy, Qiagen Inc., Valencia, CA.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.