
Abstract
A 1-day-old female Holstein–Friesian calf was presented for severe dyspnea. Physical examination revealed respiratory distress, moderate edema of the ventral neck, and swollen jugular veins. The calf died and was submitted for necropsy. A severely enlarged thymus (40 cm × 20 cm × 10 cm) weighing 1.37 kg was detected on gross examination. Histomorphology was normal but no tingible body macrophages were observed in the medullary areas. Immunohistochemistry was characterized by the lack of thymic cluster of differentiation 3 and major histocompatibility complex class II expression compared to age-matched controls. The findings were consistent with severe thymic hyperplasia, a rare congenital condition that is also described in children. Immunohistochemical findings were suggestive of impaired T-cell development and selection associated with lack of apoptosis of thymic cells (lack of tingible body macrophages). Thymic hyperplasia in juvenile animals should be considered among the differential diagnoses of mediastinal masses as a rare cause of respiratory distress in newborn calves.
Thymic hyperplasia is a rare condition reported mostly in young animals. The disease is characterized by the finding of a histologically normal, severely enlarged thymus, extending from the neck to the cranial mediastinum. The lesion may compress and embrace adjacent organs such as the veins and heart, resulting in heart failure. 19 The lesion has been reported in several domestic animals such as cats, tortoises, rabbits, birds, and cattle.3,6,19 It has previously been reported that repeated immunizations in calves, rabbits, and birds can lead to diffuse thymic hyperplasia. 19 In calves, a case of enlarged thymus has been described in a stillborn malformed calf, but no information on histological or immunohistochemical findings was reported. 2 The following report describes gross, histological, and immunohistochemical findings of massive thymic hyperplasia in a newborn calf.
A 1-day-old female, 60-kg, Holstein–Friesian calf was referred to the Clinic for Ruminants and Pigs of the Veterinary University Hospital of Lodi (Università degli Studi di Milano, Italy) because of severe dyspnea. The calf had been delivered spontaneously with a few days delay by a heifer. The latter was immunized for Bovine herpesvirus 1 and Bovine viral diarrhea virus. The farmer reported that the placenta was expelled in a few hours. The calf was fed 1 liter of colostrum and treated with corticosteroids. At physical examination, the subject was macrosomic and unable to stand. Rectal temperature was 34.4°C, mucous membranes were cyanotic, and episcleral veins were severely hyperemic and dilated. The pulse was rhythmic but reduced in frequency (72 beats per minute); breathing was abdominal (60 breaths/min), superficial, and characterized by inspiratory effort. At lung auscultation, a reinforced inspiratory murmur associated with diffuse crackling sounds was present. The examination of the neck revealed moderate edema of the ventral part with swollen jugular veins. Auricular and menace reflexes were absent, and suckling reflex was weak. Venous blood gas analysis showed the following: uncompensated respiratory acidosis with pH 7.29, partial pressure of carbon dioxide (pCO2) at 71 mmHg, partial pressure of oxygen (pO2) at 30 mmHg, base excess at 4.8 mmol/l, HCO3 at 33.2 mmol/l, and anion gap at 11.8 mmol/l. On clinical examination, an initial diagnosis of right heart failure associated with severe respiratory distress was made. Although the calf was placed under a heat lamp and infused with saline solution, it died spontaneously and was submitted to necropsy.
Gross examination was performed, and tissues samples were fixed in 10% buffered formalin, processed routinely, and embedded in paraffin wax. Serial sections (3–5 µm) were stained with hematoxylin and eosin. Immunohistochemistry was performed on tissue samples from lymphoid organs (thymus, spleen, lymph nodes) by means of polyclonal antihuman cluster of differentiation (CD)20 a at 1:400 for B-cell recognition, polyclonal anti-CD3 b at 1:900 dilution for T-cell identification, and monoclonal antihuman HLA-DR c at 1:300 dilution for the identification of antigen-presenting cells. These antibodies recognize epitopes conserved in many species, including bovids.14,18,20 As positive control, a normal thymus from an age-matched newborn calf was utilized. Negative controls consisted of substitution of specific antibodies with an isotype-matched, irrelevant monoclonal antibody or omission of the primary antibody. Briefly, heat-induced antigen retrieval was performed for CD3 and CD20 antibodies by incubation in citrate buffer (pH 6.4) and heated in a microwave oven at maximum power for 1 min and twice at 750 watt for 3 min, then cooled for 20 min. Primary antibodies were incubated overnight in a humidified chamber at 4°C. Secondary detection was performed with the avidin–biotin enzyme complex d for 30 min. The reaction was developed with the peroxidase 9-ethylcarbazol-3-amine (AEC) substrate kit for CD3 and CD20 antibodies and with the diaminobenzidine substrate kit for major histocompatibility complex class II (MHCII). e Slides were counterstained with Mayer hematoxylin for 3 min and then coverslipped. f
Postmortem examination identified a severely enlarged thymus that extended from the retromandibular area to the cranial mediastinum, reaching the heart. The typical cranial “V-form” of the young bovine thymus was lost. The organ measured 40 cm × 20 cm × 10 cm and weighed 1.37 kg. The thymus was lobulated, pale pink, soft, and homogeneous (Fig. 1). The intermandibular region and the visceral space of the neck were characterized by diffuse severe edema. The dorsocranial part of the thorax revealed mild subcutaneous petechial hemorrhages. Additional congenital anomalies included interatrial septal defect, patent ductus arteriosus, mild right ventricle dilation, and complete duplication of the gallbladder. Lymph nodes were unremarkable, and no other macroscopic abnormalities were found.
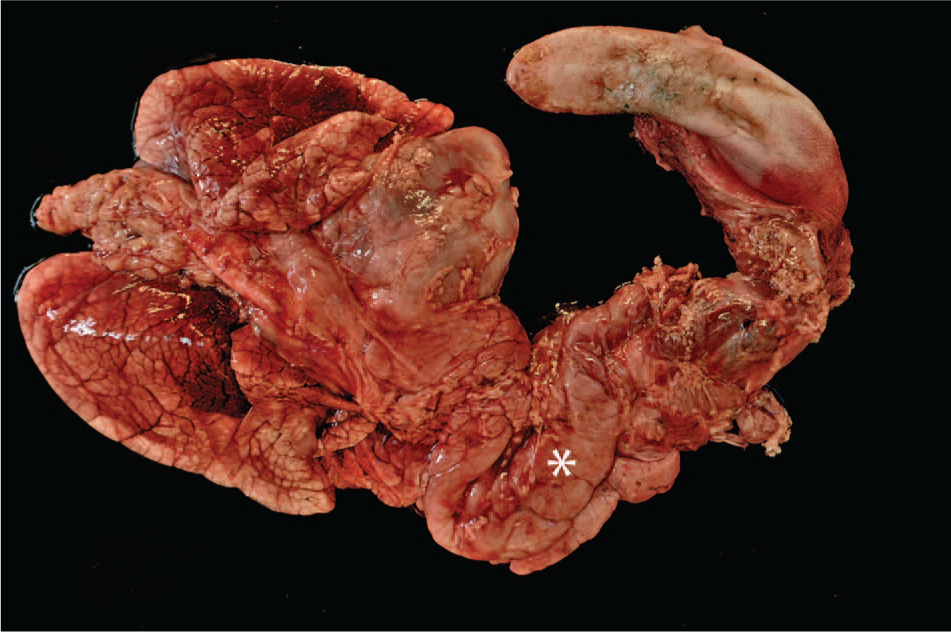
The thoracic organs of a bovine calf diagnosed with severe thymic hyperplasia. Note the severe thymic enlargement, extending from the larynx to the heart base (asterisk). Severe diffuse edema and lung atelectasis are also present.
Histological examination of the thymus revealed a normal corticomedullar ratio with well-demarcated lobules (Fig. 2). Hassall corpuscles were normal in number, morphology, and distribution, but neither tingible body macrophages (TBM) nor apoptotic bodies were identifiable in medullary areas. Lymph nodes and spleen were characterized by diffuse moderate lymphoid depletion. All other organs were microscopically normal.
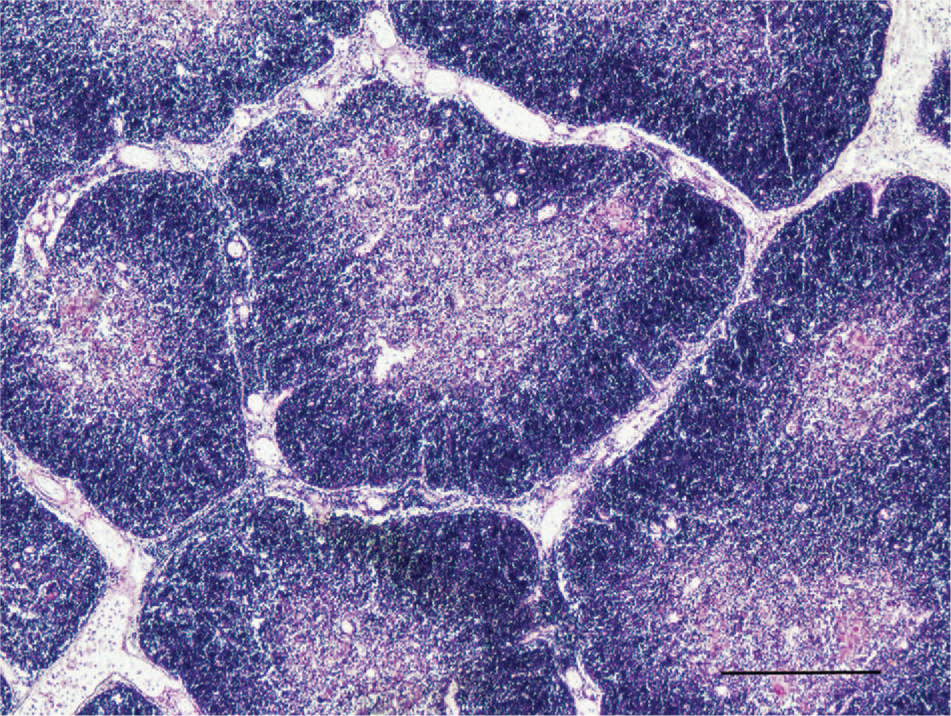
The thymus of a bovine calf with severe thymic hyperplasia. Note the normal distribution of lymphocytes in cortical and medullary areas. Hematoxylin and eosin. Bar = 750 µ.
Immunohistochemical examination of the thymus utilized as positive control was characterized by diffuse CD3 immunolabeling (Fig. 3A), with major intensity in the medulla. Malformed thymus showed very rare CD3-positive cells, both in the medulla and in the cortex (Fig. 3B). Similar immunohistochemical findings were recorded in lymph nodes and spleen, where only rare CD3-positive T cells were present (data not shown). A moderate number of lymphocytes were positive for CD20 in the control thymus (Fig. 3C), while the malformed calf evidenced rare scattered CD20-positive B cells in the thymic medulla (Fig. 3D).
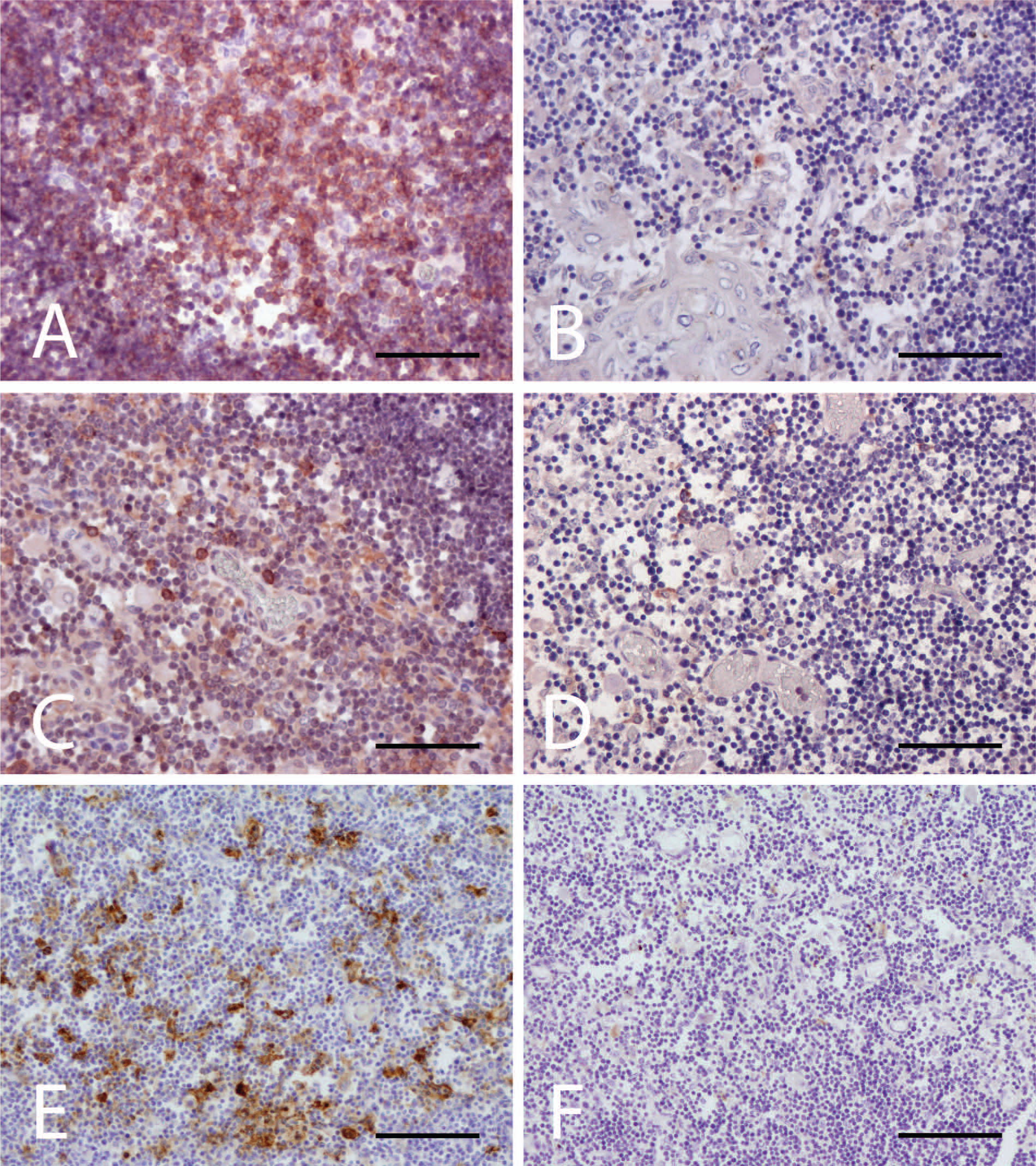
The thymus of a bovine calf with severe thymic hyperplasia compared to the thymus of a normal bovine calf of the same age.
Tissue expression of the MHCII molecule was observed in the thymus of both control and affected calves. Numerous MHCII-positive cells, with strong labeling, were detected in the thymic medulla of the control animal (Fig. 3E); most of the positive cells presented a stellate shape consistent with dendritic cells, which are very important in both positive and negative selection during T-cell development. A moderate number of MHCII-positive cells were polygonal in shape, compatible with macrophages.
In the malformed animal, immunolabeling against MHCII was restricted to the thymic medulla, where rare and weak immunoreactivity was observed (Fig. 3F). Positive cells had a dendritic morphology; macrophages were not observed in the sections examined.
Immunohistochemical results were suggestive of impaired T-cell development. The presence of a severe, diffuse enlarged thymus with a histologically normal architecture was consistent with a diagnosis of a congenital thymic hyperplasia.
The normal bovine thymus is situated in the anterior mediastinum, and organ involution occurs physiologically and progressively from the fourth to sixth year of life. A typical newborn calf thymus weighs approximately 92 g. 15 The thymus weight of a calf 1–3 weeks of age ranges from 100 g to 200 g, with an increase to 400–600 g at 4–6 weeks of age. At slaughter, a normal calf thymus weighs 600–800 g. 7 In the current case, the organ weighed 1.37 kg just after birth, which is 14 times heavier than the thymus of a normal newborn calf.
In children, occasional congenital thymic enlargement has been reported. Two entities are well recognized: true thymic hyperplasia (TTH)5,9,12 and massive thymic hyperplasia (MTH).10,11,13,16 In human medicine, TTH and MTH are characterized by a variably severe enlargement of the thymus (beyond the normal age range) with the standard microscopic structure.5,9,12 The main difference between TTH and MTH is represented by the severity of thymus hyperplasia. In MTH, thymus weight represents over 2% of body mass, with preservation of normal thymic architecture.10,11,13,16 According to a previous study, the organ weight relative to body weight in a newborn calf should be approximately 0.2%. 15 In the present case, the calf weighed 60 kg, and the thymus represented more than 2% of body mass.
The etiology and prognostic significance of human MTH is unknown. This abnormality occurs in young infants with no apparent cause, such as preexisting pathologies, and in the absence of immunologic diseases or previous systemic stressors.5,10,12 Histological examination is required to differentiate this kind of thymic hyperplasia from other thymic disorders such as thymic follicular hyperplasia of myasthenia gravis, thymoma, and thymic lymphoma. 10 In calves, the most common cause of congenital thymic enlargement is Bovine leukemia virus. 1 A second possible differential diagnosis includes thymoma; however, this is an extremely rare neoplasm in juvenile cattle. 4 In the current case, gross and microscopic examination enabled the exclusion of both tumors. Congenital myasthenia gravis-like syndrome has been described in calves, but no pathological thymic alterations have been reported previously (Thompson PN: 2006, Congenital myasthenic syndrome of Brahman cattle. PhD Thesis, University of Utrecht, Faculty of Veterinary Medicine, Utrecht, The Netherlands). 22
In human fetal thymic development, CD3-positive cells are present from week 9.5 of gestation. 8 Immunohistochemical investigation revealed the lack of CD3 expression in T cells of calf thymus, spleen, and lymph nodes in the current study. This anomalous expression could be related to an altered T-lymphocyte development leading to a putative lack of negative and positive selection. Macrophages in thymus are involved in lymphocyte selection; negatively selected T cells will physiologically undergo apoptosis with apoptotic bodies phagocytized by reactive macrophages termed TBM. In the present case, the severe increase of thymus size could have been related to an altered T-lymphocyte selection with no removal of autoreactive or nonreactive T cells. The lack of TBM supports this hypothesis, with lack of apoptosis leading to accumulation of T cells leading to thymic hyperplasia. The absence of CD3 expression identified in other lymphoid organs may derive from the disorder evidenced in the thymus. In human medicine, there are no immunohistochemically comparable data, and a pathogenic hypothesis on the origin of the severe hyperplasia has not been reported to the authors’ knowledge.
Human thymic hyperplasia is often asymptomatic, but the most common clinical sign is, as in the present case, respiratory distress.5,10,11,13,16 Moreover, the calf showed congenital neck swelling, as in a reported case of thymic hyperplasia in a Galapagos giant tortoise (Chelonoidis nigra; syn. Geochelona nigra), 6 with edema of the ventral part of the neck, and turgor of jugular veins due to the mass compression effect. In the present case, in addition to thymic enlargement, the calf had a combination of severe congenital lesions including interatrial septal defect, patent ductus arteriosus, and mild right ventricular dilation. In human medicine, concurrent congenital heart defects are reported in conjunction with thymic abnormalities.17,21 To the best of the authors’ knowledge no case of severe thymic hyperplasia has been described in calves before; therefore the possibility that heart and thymic malformations represent a more complex congenital syndrome cannot be ruled out.
In conclusion, the thymic lesion observed in this calf closely resembled cases of human MTH. Severe thymic hyperplasia should be considered among the differential diagnosis of mediastinal masses as a rare cause of respiratory distress in newborn calves; this condition in veterinary medicine should be further characterized by observing multiple cases.
Footnotes
Acknowledgements
The authors thank Prof. Paola Roccabianca and Prof. Giuseppe Sironi for assistance in the discussion of the case and for critically reviewing the manuscript.
a.
NeoMarkers Inc., Freemont, CA.
b.
Dako Denmark A/S, Glostrup, Denmark.
c.
Dako Denmark A/S, Glostrup, Denmark.
d.
Vectastain ABC kit, Vector Laboratories Inc., Burlingame, CA.
e.
Dako Denmark A/S, Glostrup, Denmark.
f.
Glicerine, Sigma-Aldrich, St. Louis, MO.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.