
Abstract
Sustained transmission of canine Influenza A virus (CIV) H3N8 among U.S. dogs underscores the threat influenza continues to pose to canine health. Because rapid and accurate detection of infection is critical to the diagnosis and control of CIV, the 2 main objectives of the current study were to estimate and compare the sensitivities of CIV testing methods on canine swab samples and to evaluate the performance of Flu Detect™ (Synbiotics Corp., Kansas City, MO) for detecting CIV nasal shedding in high-risk shelter dogs. To address the first objective, nasal and pharyngeal swab samples were collected from 124 shelter and household dogs seen by Colorado State University Veterinary Teaching Hospital clinicians for canine infectious respiratory disease between April 2006 and March 2007 and tested for CIV shedding using virus isolation, the rapid influenza diagnostic test Directigen Flu A+B™ (BD Diagnostic Systems, Sparks, MD), and real-time reverse transcription polymerase chain reaction (RT-PCR). For the second objective, 1,372 dogs with unknown respiratory health status were sampled from 6 U.S. shelters from December 2009 to November 2010. Samples were tested for presence of CIV using real-time RT-PCR and Flu Detect. Using a stochastic latent class modeling approach, the median sensitivities of virus isolation, rapid influenza diagnostic test, and real-time RT-PCR were 72%, 65%, and 95%, respectively. The Flu Detect test performed poorly for detecting CIV nasal shedding compared to real-time RT-PCR. In conclusion, the real-time RT-PCR has the highest sensitivity for detecting virus nasal shedding and can be used as a rapid diagnostic test for CIV.
Keywords
Canine Influenza A virus (CIV; family Orthomyxoviridae, genus Influenzavirus A) was first detected in greyhounds at a Florida racetrack in 2004 4 and has since been isolated from dogs throughout the United States (Cornell Animal Health Diagnostic Center: 2012, Test summary for canine influenza virus in dogs not affiliated with greyhound racetracks. Available at http://ahdc.vet.cornell.edu/docs/Statistics_for_Canine_Influenza_Virus.pdf. Accessed on November 21, 2012). Symptoms of CIV infection include nasal discharge; fever (>39.4°C); dry, persistent, nonproductive cough; weight loss; anorexia; and lethargy. 5 Because the clinical signs of CIV mirror those of other causes of canine infectious respiratory disease complex (CIRDC), the ability to diagnostically differentiate respiratory illness caused by CIV from other CIRDC pathogens is paramount to initiation of optimal therapeutic and control measures. While serologic tests are a key tool in the diagnosis of CIV infection, a single positive serum antibody titer only indicates exposure to the virus, not necessarily active infection or disease. Therefore, virus isolation (VI) in embryonated chicken eggs or cell culture, traditionally considered the “gold standard” in influenza diagnostics, 19 is often employed to confirm CIV infection. However, due to the fact that the procedure can be time consuming and cumbersome, other sensitive diagnostic methods have been developed for detecting influenza virus shedding, including reverse transcription polymerase chain reaction (RT-PCR) and rapid influenza detection tests (RIDTs). The RIDTs, such as the enzyme immunoassay Directigen Flu A+B™ (FluAB) a and the lateral flow avian Influenza A virus antigen test Flu Detect™, b have become popular in the hospital and field setting, despite reports of low sensitivity for detecting influenza virus.6,7,11 Alternatively, highly sensitive quantitative or real-time RT-PCR–based and multiplex RT-PCR assays have been developed and implemented in many diagnostic laboratories for detecting Influenza A virus strains,10,12,15 including for CIV.9,13 The advantages of real-time RT-PCR over other diagnostic methods include its high sensitivity, high specificity, and rapid turnaround time.3,10,12,16 To assess various diagnostic tests used for detecting CIV in dogs, the present study sought to 1) estimate and compare the sensitivities of CIV testing methods (VI, FluAB, and real-time RT-PCR) and 2) evaluate the performance of the Flu Detect RIDT in detecting CIV nasal shedding in high-risk shelter dogs.
Two studies were completed to assess the performance of various CIV diagnostic methods. For the first study, a total of 124 shelter and household dogs demonstrating symptoms of CIRDC were swabbed between March 2006 and April 2007 by clinicians at Colorado State University Veterinary Teaching Hospital (CSU-VTH; Fort Collins, CO) or on-site at shelters reporting CIRDC. Briefly, a sterile polyester-tipped swab was inserted into the nostril of each dog and, if possible, a second swab was collected from the pharynx of each animal. The swab samples were immediately placed in different vials of 1 ml of viral transport medium (phosphate buffered saline, 5 mg/ml of bovine serum albumin, 2,000 U/ml of potassium penicillin G, 4 mg/ml of streptomycin, 16 µg/ml of gentamicin, and 100 U/ml of nystatin) and stored at −80°C until VI, FluAB RIDT, and real-time RT-PCR assay could be performed. For the second study, 2 nasal swabs were simultaneously collected between December 2009 and November 2010 from 1,372 dogs housed in 1 of 6 different humane shelters participating in a large-scale U.S. CIV surveillance program. One swab was processed on-site according to the recommendation of the manufacturer of Flu Detect. The second nasal swab sample was stored at 4°C before being shipped to the laboratory overnight on ice for real-time RT-PCR assay. All studies were reviewed and approved for conduct by the CSU Institutional Animal Care and Use Committee prior to initiation.
Influenza viruses from swabs were isolated by inoculating both Madin–Darby canine kidney (MDCK) cells and the allantoic cavity of 10-day-old embryonated chicken eggs with 200 µl of thawed viral transport medium and incubated for 48–72 hr at 37°C. Incubation for the inoculation of MDCK cells included 5% CO2. After cell culture inoculation, 2 ml of Eagle minimum essential medium c supplemented with 2.25 mg/ml of bovine serum albumin, 50 mg/ml penicillin–streptomycin, 250 μg/ml amphotericin B, and 1 µg/ml of tolylsulfonyl phenylalanyl chloromethyl ketone–treated trypsin d were added to each well. Cell and egg cultures were passaged up to 3 times. Influenza virus was confirmed by immunocytochemistry staining with an anti–influenza A nucleoprotein antibody e and RT-PCR amplification using SZAHA primers 20 for the hemagglutinin and neuraminidase genes. The PCR products were analyzed by direct cycle sequencing f at the CSU Proteomics and Metabolomics Facility (Fort Collins, CO). Nucleotide and amino acid sequences were assembled using commercial g software.
For the 1-step real-time RT-PCR assay, primers and probes were designed using commercial h software and based on 9 matrix (M) gene sequences from equine and canine Influenza A virus H3N8 strains isolated in North America. A 144-bp M gene product was amplified with forward (5’-GAACACCGATCTTGAGGCACTC-3’) and reverse (5’-GGCATTTTGGACAAAGCGTCTAC-3’) primers. The 5’ reporter dye (6-carboxyfluorescein) labeled probe consisted of 23 nucleotides (5’-AGTCCTCGCTCACTGGGC ACGGT-3’). Five-microliter aliquots of viral RNA, extracted i from 140 μl of viral transport medium, were mixed with 20 μl of premixed reaction solution j containing 200 nmol each of the forward and reverse primers, and 80 nmol of the probe. Amplification and detection were performed using a commercial instrument k under the following conditions: 10 min at 52°C, 5 min at 95°C, followed by 45 cycles of 10 sec at 95°C and 45 sec at 68.4°C. SYBR Green j was used for optimization of the thermal-amplification profile and concentration of primers. The minimum detection level of viral RNA was determined to be 103 M gene copies per reaction from serial dilutions (107–100 genomic equivalents/μl) of purified M gene, which had been cloned into a vector system. l The threshold of the real-time RT-PCR assay was defined as Rn = 0.1 based on the midpoint of the linear region of the amplicon parametric receiver operating characteristic curve analysis. Swab samples were run in duplicate, while ribonuclease-free water served as the negative control, and 10 TCID50 of A/canine/CO/224986/2006 (H3N8) served as the positive control. Standardization was performed using dilution series of 4 H3N8 isolates grown in MDCK cultures (A/equine/KY/1/1981, m A/equine/WI/1/2003, n and clinical isolates A/canine/CO/224986/2006 and A/canine/CO/148902/2006).
Sensitivity estimates for VI, FluAB, and real-time RT-PCR were determined by a stochastic latent class modeling approach described previously 2 using Gibbs sampling. 18 The CSU-VTH study data set was divided into shelter (n = 97) or household (n = 27) populations, and VI, FluAB, and real-time RT-PCR assay results (Table 1) were compared for the analysis. Prior probabilities (Table 2) were based on sensitivity, specificity, and prevalence estimates from previous studies.1,4,6 -8,11 Inferences were based on 100,000 iterations (with a burn-in of 5,000 iterations) after 6 chains indicated there was no lack of convergence. All models were run with specific software. 14 Estimates showed that real-time RT-PCR was the most sensitive assay with a median sensitivity of 0.95 (95% probability interval [PI]: 0.83–0.99) compared to VI (median sensitivity 0.72; 95% PI: 0.47–0.96) and FluAB (median sensitivity 0.65; 95% PI: 0.48–0.80). There are several assumptions for the stochastic latent class analysis to consider: 1) 2 tests should be dependent and 1 test independent, 2) the data set must consist of 2 different populations, and 3) there needs to be constant specificity and sensitivity for each diagnostic test evaluated. For the first assumption, FluAB and PCR both detect the same biological phenomenon (gene or gene products) and can, therefore, be considered the dependent tests, while VI relies on the presence of infectious virus and is considered the independent test. For the second assumption, there is a clear environmental difference between dogs residing in households versus dogs that are located within humane shelters where they often comingle with other dogs and are introduced to dogs with unknown health histories. Moreover, seroprevalence studies conducted in shelters reporting CIRDC4,8 show much higher seropositivity compared to the few studies done in household dogs.1,17 For the third assumption, there is no indication that the sensitivity and specificity of the diagnostic tests evaluated are different for different populations. The high sensitivity of real-time RT-PCR is not surprising, as other real-time RT-PCR assays used in Influenza A virus detection show similar sensitivities.3,10 It is important to note that for VI, swab samples had been frozen within 12 hr of collection and then subsequently thawed before inoculations. This single freeze–thaw could have resulted in a reduction of infectious virus titer and, thus, reduction in the sensitivity of virus detection. However, as RT-PCR has been shown to be able to detect influenza viruses even in samples repeatedly frozen and thawed, 7 the relatively high sensitivity of real-time RT-PCR and its rapid turnaround makes it the ideal test for first-step CIV analysis.
Comparison of canine Influenza A virus shedding detection by real-time reverse transcription polymerase chain reaction (RT-PCR), FluAB rapid influenza diagnostic test, and virus isolation (VI), and from nasal and pharyngeal swabs.*
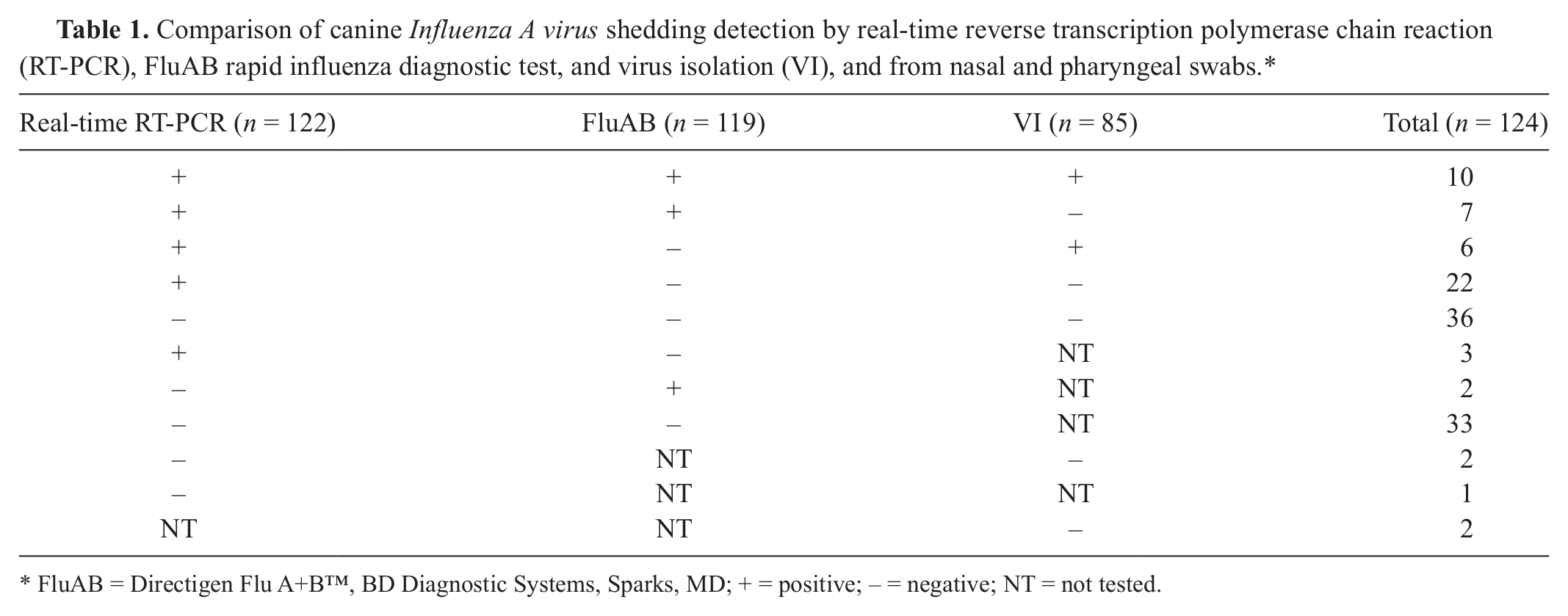
FluAB = Directigen Flu A+B™, BD Diagnostic Systems, Sparks, MD; + = positive; − = negative; NT = not tested.
Estimates, modes, 95% probability intervals (PI), and beta distributions used for prior distributions in the stochastic latent class models.
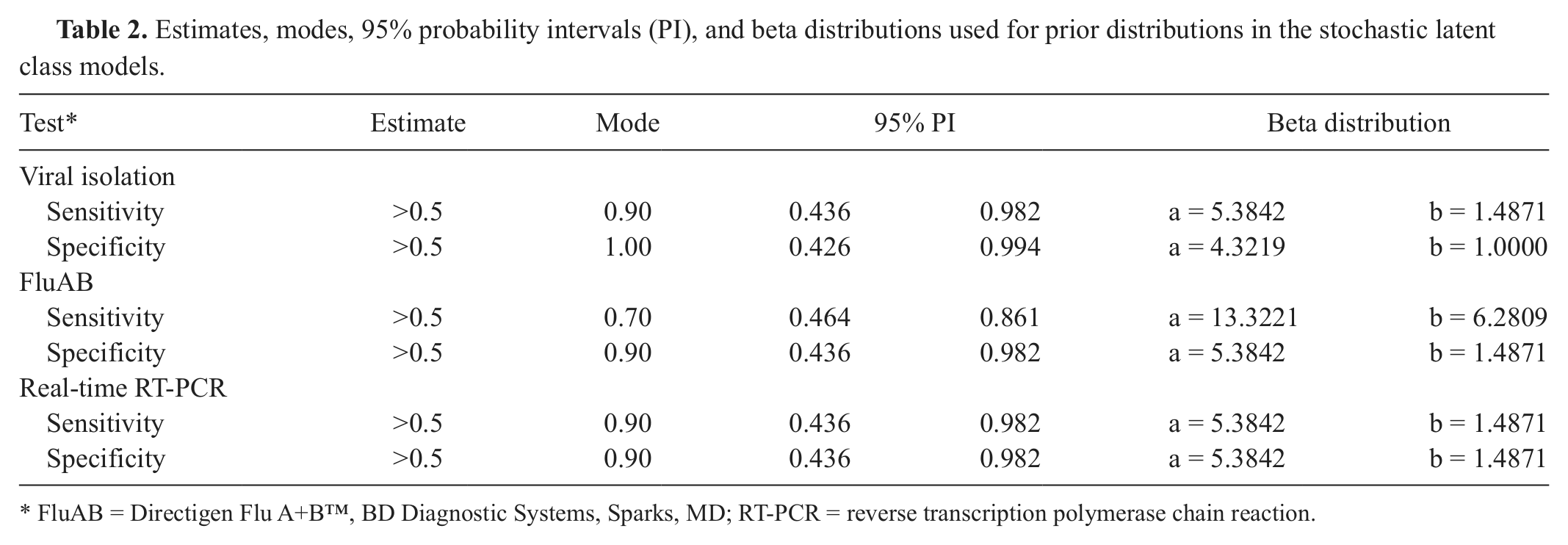
FluAB = Directigen Flu A+B™, BD Diagnostic Systems, Sparks, MD; RT-PCR = reverse transcription polymerase chain reaction.
As there was only 1 population (shelter dogs) sampled for the Flu Detect RIDT analysis, the sensitivity, specificity, positive predictive value, and negative predictive value were determined using traditional calculations from a 2 × 2 contingency table. Of the 1,372 shelter dog nasal swab samples used for the evaluation of the Flu Detect RIDT, only 3 of the 38 tests that were positive by real-time RT-PCR were also positive by Flu Detect, while Flu Detect was negative in 35 nasal swab samples that were positive by real-time RT-PCR. Conversely, Flu Detect was positive for 218 of the 1,334 samples that were negative by real-time RT-PCR. Using real-time RT-PCR as the reference, the Flu Detect RIDT had a sensitivity of 7.9% (3/38), specificity of 83.7% (1,116/1,334), positive predictive value of 1.4% (3/221), and negative predictive value of 97.0% (1,116/1,151). All 6 shelters in the study showed similar inconsistencies between real-time RT-PCR and Flu Detect results. Although FluAB was clearly better than the Flu Detect test at diagnosing canine influenza in dogs, the 95% PI for FluAB sensitivity ranged from 48% to 80%, suggesting that true-positive samples in the current study might have been misdiagnosed as negative. Similarly, the Flu Detect test is poorly suited for CIV diagnosis, and, in fact, was more likely to give a false-positive rather than a true-positive result. It should be noted, however, that PPV is generally low when there is low prevalence of disease and, indeed, the true prevalence of CIV is currently unknown in all dog populations.
In conclusion, the findings in the current study suggest that real-time RT-PCR has the highest sensitivity of the 3 methods evaluated for detecting CIV nasal shedding and can be used as a rapid diagnostic test for CIV. If real-time RT-PCR cannot be performed for a suspected case of CIV, isolation and quarantine remain the safest approaches. However, this strategy is impractical for many facilities, and the cost for real-time RT-PCR might be higher than RIDTs. Facilities with financial constraints could consider testing in series, starting with FluAB RIDT performed on-site, followed by real-time RT-PCR confirmation while the potentially infected dog is isolated to minimize CIV transmission to naïve dogs. As turnaround time for real-time RT-PCR is approximately 1 day, the quarantine period could range from 48 hr (for a negative real-time RT-PCR sample) to 7 days (for a positive real-time RT-PCR sample). Ultimately, the real-time assay has the highest sensitivity for detecting virus nasal shedding and is recommended as a rapid diagnostic test for CIV.
Footnotes
Acknowledgements
The authors thank the veterinarians and staff from CSU-VTH and from the participating humane shelters for sample collection and performing the on-site test strips, and Dr. Katharine Benedict for help with the stochastic latent class modeling.
a.
BD Diagnostic Systems, Sparks, MD.
b.
Synbiotics Corp., Kansas City, MO.
c.
Gibco, Invitrogen Corp., Carlsbad, CA.
d.
Worthington Biochemical Corp., Lakewood, NJ.
e.
Kindly provided by Drs. M. McGregor and Y. Kawaoka, University of Wisconsin–Madison, Madison, WI.
f.
PE, Applied Biosystems, Foster City, CA.
g.
Lasergene 7.0, DNASTAR Inc., Madison, WI.
h.
Beacon Designer, Premier Biosoft Inc., Palo Alto, CA.
i.
QIAamp Viral RNA Mini Kit, Qiagen GmBH, Hilden, Germany.
j.
iScript One-Step RT-PCR Kit, Bio-Rad Laboratories, Hercules, CA.
k.
Mastercycler Realplex, Eppendorf AG, Hamburg, Germany.
l.
pGEM-T Easy vector, Promega Corp., Madison, WI.
m.
Kindly provided by Dr. D. P. Lunn, North Carolina State University, Raleigh, NC.
n.
Kindly provided by Dr. C. W. Olsen, University of Wisconsin–Madison, Madison, WI.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by a grant from the Morris Animal Foundation (D09CA-009).