
Abstract
Tuberculosis pathology was studied on 19 African buffalo (Syncerus caffer) from a herd in the Hluhluwe-iMfolozi Park in South Africa. The animals tested positive with the comparative intradermal tuberculin test and were euthanized during a test-and-cull operation to decrease prevalence of bovine tuberculosis (bTB) in the park. The lymph nodes and lungs were examined grossly for presence of tuberculous lesions, which were scored on a 0–5 scale for macroscopic changes. The gross lesions were examined histologically and classified into grade I, II, III, or IV according to a grading system used for bTB lesions in domestic cattle. Macroscopic lesions were limited to the retropharyngeal, bronchial, and mediastinal lymph nodes and the lungs. The most frequently affected lymph nodes were the bronchial (in 16 animals) and mediastinal (in 11 animals). All four grades of microscopic lesions were observed, grade II lesions were the most frequent. Mycobacterium bovis was detected by PCR in 8 out of 19 animals, and acid-fast bacilli were seen in 7 out of 19 animals, together both techniques identified mycobacteria in 5 out of 19 animals. Lesions were paucibacillary, as acid-fast bacilli were only rarely observed. The absence of lesions in the mesenteric lymph nodes and the high frequency of lesions in respiratory tract associated lymph nodes suggest that the main route of M. bovis infection in African buffalo is by inhalation.
Mycobacterium bovis has a wide host range and infects many wild and domestic animal species as well as human beings. Bovine tuberculosis (bTB) is an important disease in many parts of the world because of its zoonotic potential and its economic and conservation impacts.3,5 The African buffalo (Syncerus caffer) is considered to be a wildlife reservoir of M. bovis in certain environments in South Africa, such as in the Kruger National Park (KNP) and Hluhluwe-iMfolozi Park (HiP). 17 Bovine TB was first diagnosed in buffalo in HiP in 1986. Currently, within herd prevalence varies from 5% to 50% between herds (D. Cooper, unpublished data). The gregarious nature of buffalo facilitates the spread of the disease within herds. 8 Infected buffalo can contaminate the environment 8 and are considered to be a source of infection to other wild animal species, including predators and scavengers, as well as livestock.3,14 Previous reports of bTB in African buffalo2,8 describe lesions as being most often located in the lymph nodes (LNs) of the head, in the bronchial and mediastinal LNs, and in the tonsils and lungs. Affected LNs are enlarged and show lesions of variable size, which may contain foci of caseous necrosis and mineralization. In the lungs, bTB lesions can be distributed as either disseminated or diffuse pneumonia, or as single individual granulomas. Generalized forms of bTB in buffalo have also been described and can affect various internal organs as well as visceral and peripheral LNs.2,13
The current study provides a systematic and detailed description of the macroscopic and histopathologic lesions caused by natural M. bovis infection in African buffalo, and applies a scoring system to classify lesions according to their size, cellular composition, and degree of development. The purposes of the present study were 1) to contribute to the understanding of the pathogenesis of natural disease in African buffalo, and 2) to provide a semiquantitative evaluation of the severity of the lesions, which can be used as a comparative base for experimental infection and vaccine efficacy evaluation studies.
The buffalo used in the present study were obtained from a test-and-cull operation, aimed at reducing the prevalence of bTB in the species. The program started in 1999 in HiP and includes annual buffalo capture for standard bovine comparative intradermal test, using both avian and bovine Dutch tuberculin, a followed by culling of bTB-positive buffalo. 12 All positive reactors in 1 test-and-cull operation (24 buffalo) were killed by a gunshot to the brain and transported to the HiP abattoir. At slaughter inspection, 19 out of 24 animals showed visible gross lesions suggestive of tuberculosis, and these buffalo were selected for further pathology studies.
The age category, subadult or adult (Table 1), was determined based on tooth eruption patterns. The lungs were sliced at 2-cm intervals, and each slice was inspected and palpated. The following LNs were sliced (approximately 2-mm thick slices), and each slice was visually inspected: head-associated LN (paired mandibular, parotid, and medial retropharyngeal), thoracic LN (mediastinal and bronchial), abdominal LN (mesenteric, hepatic, omasal, and abomasal), and paired peripheral superficial LN (superficial cervical, axillary, and popliteal). Tissues with lesions were fixed in formalin for histopathology.
Nineteen African buffalo (Syncerus caffer) from a herd in the Hluhluwe-iMfolozi Park in South Africa examined for bovine tuberculosis.
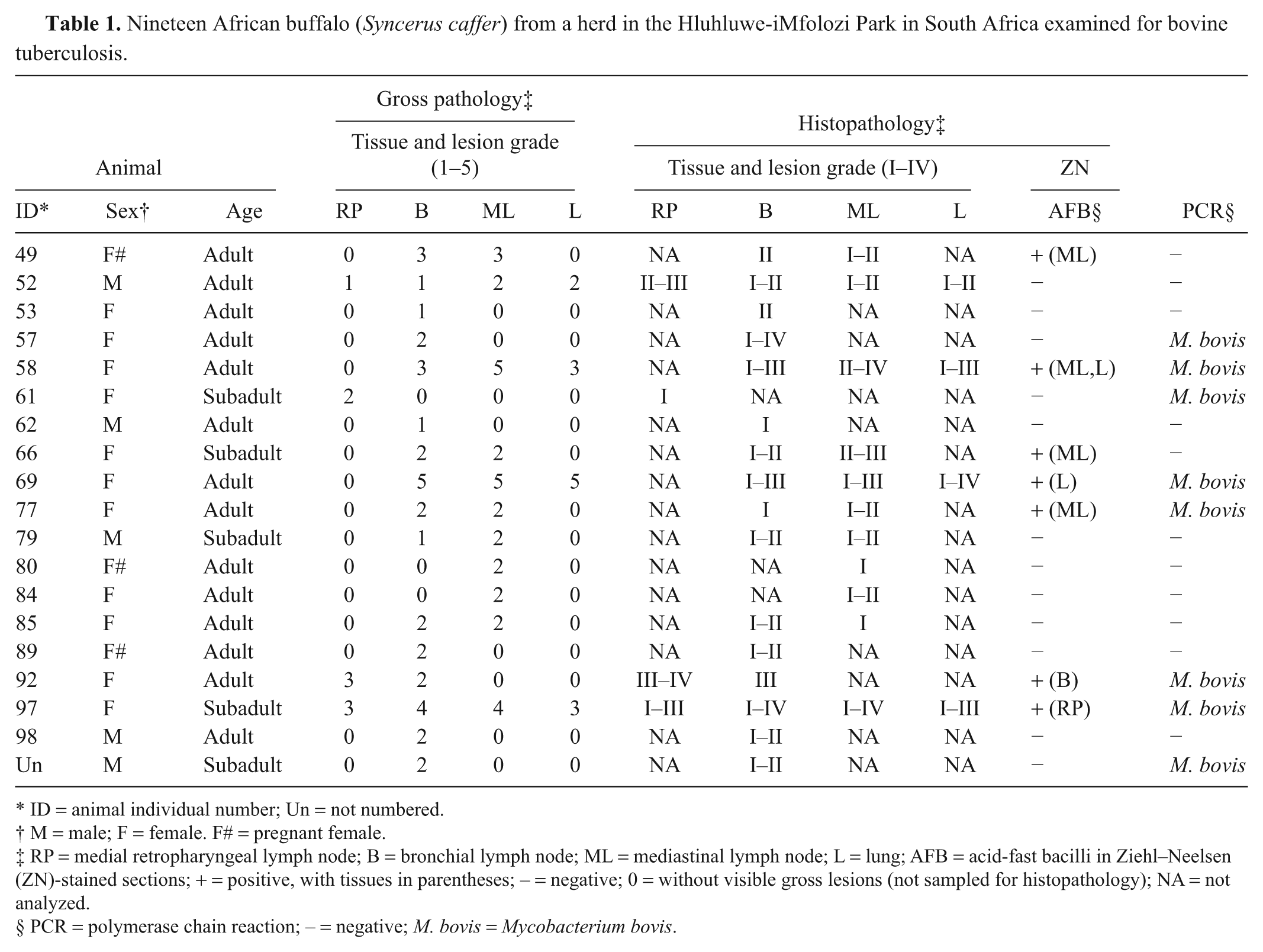
ID = animal individual number; Un = not numbered.
M = male; F = female. F# = pregnant female.
RP = medial retropharyngeal lymph node; B = bronchial lymph node; ML = mediastinal lymph node; L = lung; AFB = acid-fast bacilli in Ziehl–Neelsen (ZN)-stained sections; + = positive, with tissues in parentheses; – = negative; 0 = without visible gross lesions (not sampled for histopathology); NA = not analyzed.
PCR = polymerase chain reaction; – = negative; M. bovis = Mycobacterium bovis.
Any focus, foci, or nodules, either as a single lesion, or multifocal or confluent, that were yellow–white, circumscribed, and solid, or necrotic, with or without apparent caseation and mineralization, were considered and graded as macroscopic tuberculous lesions. The lung and LN lesions were categorized in grades 0–5 according to the size and number of their gross lesions. Grade 1 was used for a single minimal lesion, up to 1 mm; grade 2 for 2–4 lesions of 2–5 mm; grade 3 for 5–8 lesions, up to 10 mm, or many small lesions affecting approximately 50% of a LN; grade 4 for confluent and extensive lesions in most slices but with some normal looking tissue left; and grade 5 for abundant lesions, with none or nearly no apparently healthy tissue left. The lungs and LNs that did not show visible lesions were classified as grade 0 and were not sampled for further histopathology (Table 1). Histological sections were stained with hematoxylin and eosin, with Ziehl–Neelsen stain to identify acid-fast bacilli (AFB) and with Masson trichrome to visualize fibrous tissue.
The tuberculous granulomas in the LNs and lungs were microscopically classified into 4 categories of development according to criteria previously described for cattle. 22 The lesions were evaluated for their size, presence of AFB, type and extension of necrosis and mineralization, abundance and distribution of inflammatory cell components, and degree and architecture of fibrosis. Briefly, the granulomas were classified into 4 categories, namely: stage I (initial or early lesions); stage II (solid granulomas); stage III (minimal necrosis); or stage IV (necrosis and mineralization).
DNA was extracted from formalin-fixed, paraffin-embedded tissue sections as previously described. 11 Real-time polymerase chain reaction (PCR) was performed by using a commercial system. b The real-time PCR mixtures for amplification of DNA consisted of 50-μl total volume containing: 25 μl of 2× power SYBR Green, c 5 μl of template, and 10 pmol of each oligonucleotide primer (myc1 and myc3) d in a final 50-μl reaction volume. These primers simultaneously amplify the Mycobacterium tuberculosis complex (M. bovis and M. tuberculosis) and the Mycobacterium avium complex (M. avium and M. avium subsp. paratuberculosis) producing different amplicon sizes of 178 bp and 257 bp, respectively. 4 Samples were heated at 95ºC for 10 min. Temperature cycling consisted of 45 cycles of 95ºC for 30 sec, 58ºC for 45 sec, and 72ºC for 30 sec, with an increase of 1 sec per cycle for the denaturation and extension steps. Dissociation curve analysis was performed to check the specificity of the amplified products. All reactions were run in duplicate. Mycobacterium tuberculosis complex and M. avium complex PCR products were differentiated based on the melting temperatures as previously described. 11
Results showed all animals to be in good body condition. Postmortem lesions consistent with tuberculosis were found in the LNs of the head, thoracic cavity, and/or lungs of the 19 animals (Table 1). Lesions suggestive of tuberculosis were not detected in other organs or LNs. The spectrum (macroscopic grades 1–5) of lesions in the LNs ranged from small (1 mm in diameter) white foci, to single or multiple encapsulated granulomas of different sizes, with central caseation and mineralization, or to diffuse, nonencapsulated lesions effacing and replacing normal lymphoid tissue.
A majority of the animals showed tuberculous lesions in the bronchial (16/19) and mediastinal (11/19) LNs. Twenty-one percent (4/19) of the animals presented tuberculous lesions in the lungs and 21% (4/19) in the retropharyngeal LNs. Forty-seven percent (9/19) of the animals presented lesions in only one LN, 31.6% (6/19) in 2 LNs, 10.5% (2/19) in 2 LNs as well as in the lungs, and 10.5% (2/19) showed lesions in 3 different LNs and in the lung. Most buffalo (73.7%) presented macroscopic tuberculous lesions of early stages (grade 1 and/or 2) while 26.3% (5/19) presented moderate to high severity gross lesions (grades 3–5). Grade 5 lesions were observed in only 2 (10.5%) animals, no. 58 (in the mediastinal LN) and no. 69 (in the bronchial and mediastinal LNs and lung; Table 1). All 4 microscopic stages were found. Stage I lesions were characterized by irregular, unencapsulated clusters of predominantly epithelioid macrophages, lymphocytes, and few multinucleated giant cells, without necrosis (Fig. 1); stage II were partly or completely thinly encapsulated granulomas formed by predominantly epithelioid macrophages, Langhans giant cells, and lymphocytes surrounding minimal areas of necrosis; stage III were encapsulated granulomas with central necrosis, often caseous and mineralized, surrounded by epithelioid cells, Langhans giant cells, and lymphocytes at the periphery (Fig. 2); and stage IV were large, thickly encapsulated, multicentric granulomas with extensive caseous necrosis and often multiple areas of mineralization surrounded by epithelioid cells, giant cells and lymphocytes. Extensive lesions formed by multifocal to coalescing stage I granulomas were frequently observed. Some granulomatous lung lesions involved the wall of the bronchioles, occasionally extending into the lumen. Most animals presented microscopic TB lesions of stage II. There were often several lesions of different stage within a single LN. The most chronic or advanced microscopic stage (IV) was seen in 5 animals. One buffalo with severe macroscopic lesions presented microscopic granulomas of stage III. In LNs with macroscopic lesions of grades 4 and 5, it was common to find lesions of microscopic stage IV in that tissue. Neovascularization was a frequent finding in the peripheral connective tissue in stages III and IV granulomas. Acid-fast bacilli were observed in tissues from 7 animals (36.8%), most with macroscopic lesions of grades 3–4. The AFB were detected in mediastinal LNs (4/7), lung (2/7), bronchial LNs (1/7), and retropharyngeal LNs (1/7). When present, AFB were found in low numbers, mostly as a single bacillus in multinucleated giant cells (Table 1). Amplification of DNA by real-time PCR identified the genome of M. bovis in 8 out of 19 African buffalo (Table 1). Dissociation curve analysis showed that positive samples presented an amplicon melting temperature of 87.8 ± 0.3ºC. The technique was validated using positive controls of M. bovis culture (courtesy of Dr. Parra, Spain) and by means of sequencing. The macroscopic and histologic morphology of the tuberculous lesions in the buffalo closely resembled that of cattle. The microscopic classification described for domestic cattle, 22 could be applied to the buffalo lesions. Due to logistic difficulties during fieldwork in remote areas of HiP, fresh or frozen samples could not be used for mycobacterial culture. However, M. bovis has regularly been isolated from culled buffalo within the HiP bTB test-and-culling program. 12
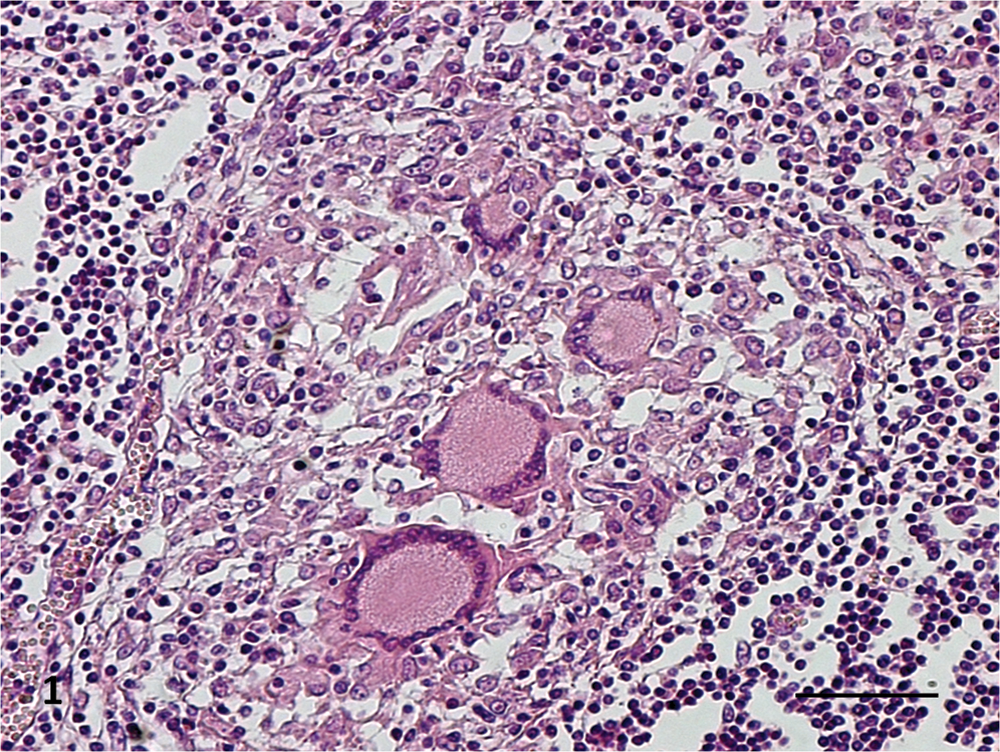
Histological section of a mediastinal lymph node of an African buffalo (Syncerus caffer) with bovine tuberculosis. Stage I granuloma, epithelioid cell, and multinucleated giant cells surrounded by lymphocytes. Hematoxylin and eosin. Bar = 50 µm.
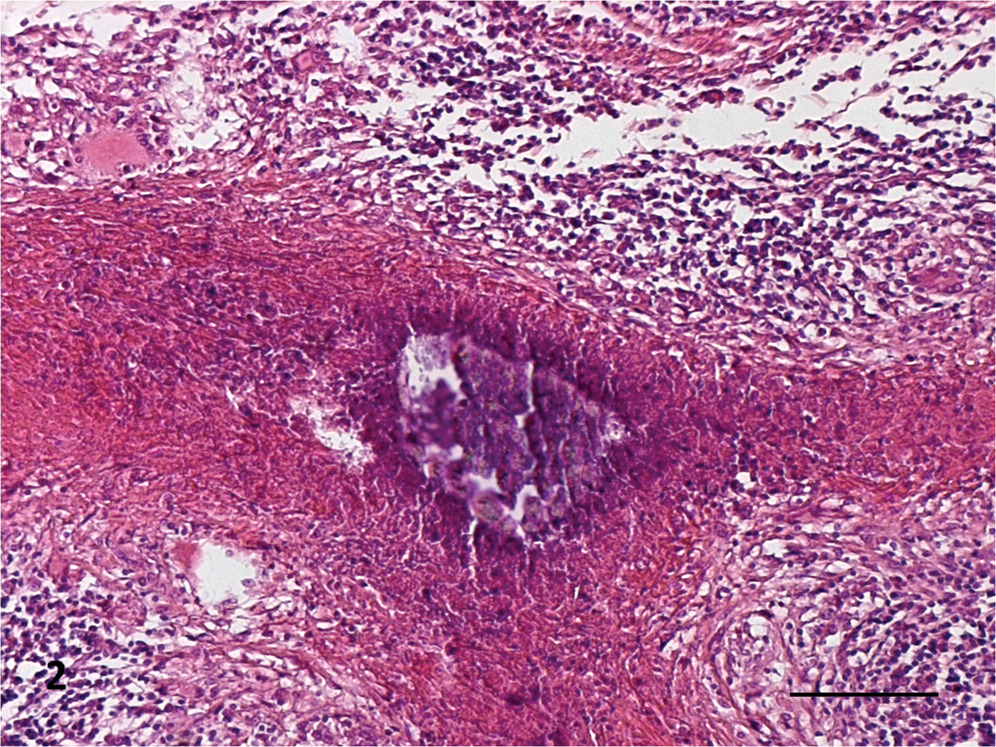
Histological section of a bronchial lymph node of an African buffalo (Syncerus caffer) with bovine tuberculosis. Stage III granuloma: central area of caseous necrosis and mineralization, surrounded by multinucleated giant cells and lymphocytes. Hematoxylin and eosin. Bar = 100 µm.
Of the 24 animals that tested positive with the tuberculin skin test and were slaughtered, 19 (79.2%) presented macroscopic and microscopic tuberculous lesions. The animals were in good body condition, and the lesions affected only a few LNs, indicating an early or limited disease stage. Only 3 animals (nos. 58, 97, and 69) presented more severe lesions in 2 or 3 LNs, as well as in the lung. Advanced cases are less likely to be found in the herds subjected to test-and-cull program, since many of the positive animals that may have had advanced disease have probably been removed since the program in HiP began in 1999. A study in HiP demonstrated that approximately 70% of bTB cases in buffalo were mild, 12 and it was considered unlikely that they had shown clinical signs.2,6 This supports the assertion that bTB in buffalo is a disease of limited and slow development in the majority of the cases. 12
Studies have shown that gross examination at slaughter fails to detect some of the M. bovis–infected animals, mostly those with very small (approximately <1 mm in size) or no visible lesions (NVL).1,10 In the study reported herein, such NVL cases may have occurred but were not investigated.
The buffalo presented lesions most frequently in the LNs associated with the respiratory tract (mediastinal and bronchial LNs) and in the lungs, suggesting that the most likely route of infection was inhalation. The findings are consistent with previous descriptions in African buffalo,7,13 water buffalo, 9 and are also similar to bTB in cattle. 15 Similar to other studies in cattle 16 and buffalo, 8 the tuberculous lesions in the lungs were common in the caudal lobes. Most of the buffalo (80%) did not show bTB lesions in the lungs, but had gross lesions in bronchial and mediastinal LNs. This agrees with descriptions of early stages of bTB in cattle, and is most likely due to the difficulties of detecting very small lesions in the lungs at inspection, due to their large volume. 15 In the present study, pulmonary lesions were detected in 21% of the buffalo, and they were of the higher grades. The absence of lesions in the gastrointestinal tract suggests that the oral route is not the main route of infection in buffalo. 13
As in other studies, most of the animals (73.7%) included in the current study were adults.12,19 It has been reported that young buffalo have a lower risk of being positive for bTB than older buffalo, but that the risk for both age groups increases with increasing prevalence of the disease within the herd. 19 Microscopically, in 2 animals with severe lung lesions, the granulomas had eroded the wall of bronchioles, indicating that these animals could excrete M. bovis and be a source of infection for other animals. 16
Animals that presented higher macroscopic lesions, grades 3–5, were the most likely to present up to 4 different microscopic grades in the same section. This result agrees with a previous report in naturally TB-infected cattle, 15 and it likely represents repeated seeding of the LNs by M. bovis with development of lesions at different times. The degree of peripheral fibrosis in advanced tuberculous granulomas appears to be a feature related to the species of the host. 18 In the buffalo, fibrosis in advanced granulomas is a prominent feature, as in cattle.18,22 In the current study, Langhans multi-nucleated giant cells occurred in the 4 stages but were more frequent in grades III and IV. This finding is similar to the results reported in cattle. 22 Few AFB were observed histologically, usually in giant cells, indicating that the lesions were paucibacillary.
Polymerase chain reaction identified 3 animals in which acid-fast bacteria were not detected, but conversely, acid-fast staining identified organisms in 2 animals that were negative by real-time PCR. Overall, the 2 methods combined identified DNA and/or acid-fast organisms in 10 out of 19 animals that had gross postmortem and histological lesions compatible with M. bovis infection. With paucibacillary lesions, acid-fast staining can have low sensitivity, which might be increased by examining multiple or serial sections. The low positivity of real-time PCR may be due to insufficient DNA template in a small sample or the negative effects of formalin fixation on DNA amplification. 21 Mycobacterial culture would have likely increased the number of animals confirmed, as it has higher sensitivity than PCR. 20 However, it cannot be ruled out that the lesions in which M. bovis or AFB were not demonstrated were actually caused by other pathogens. The inability to confirm the presence of AFB in mycobacterial infection is a common problem in veterinary diagnostics. 20 In the present study, the animals were positive at the tuberculin skin test, and the histological features of the lesions were highly characteristic of TB, indicating that the granulomas were likely caused by M. bovis, though this can unfortunately not be confirmed.
In conclusion, the gross and microscopic morphology of TB in the African buffalo closely resembles TB in cattle. The current study presents a systematic evaluation and semiquantification of the severity and stages of development of tuberculous lesions in naturally infected buffalo. The results may contribute to 1) the understanding of the pathogenesis of the disease, 2) the evaluation of experimental models of M. bovis infection in Syncerus caffer, and 3) the interpretation of pathology data from vaccination trials. Experimental studies in buffalo are needed to understand the pathogenesis of bTB, specifically the time between infection and development of the different lesion stages.
Footnotes
Acknowledgements
The authors thank Dr Dave Cooper, from HiP, for providing the excellent facilities and appropriate environment for the sampling. The staff of the division of Pathology, Veterinary Faculty, Eduardo Mondlane University is acknowledged for the work with cutting and staining of histological sections.
a.
PPD, Institute for Animal Science and Health, Lelystad, The Netherlands.
b.
7300, Applied Biosystems, Foster City, CA.
c.
Applied Biosystems, Warrington, United Kingdom.
d.
TIB Molbiol, Berlin, Germany.
The authors declared that they had no conflicts of interest with respect to their authorship or the publication of this article.
This study was funded by SIDA-SAREC, with contribution of the European Union Seventh Framework Programme grant agreement no. 222633 (WildTech).